
Abstract
Interferon-alpha (IFN-α)-based therapy is associated with several hematological adverse events in hepatitis C virus (HCV)-infected patients with advanced fibrosis. We performed this study to evaluate the association between Fibrosis-4 (Fib-4) index and hematological adverse events in patients with chronic HCV infection, undergoing IFN-α-based triple therapy. We included 120 HCV-infected patients, receiving triple therapy: weekly PegIFN-α, daily ribavirin (1,000–1,200 mg), and daily sofosbuvir (400 mg) for 12 weeks. We compared Fib-4 scores for patients who developed hematological adverse events at weeks 4 (w4) and w12 of treatment and w12 post-treatment versus those who did not. Treatment with the aforementioned triple regimen was associated with a sustained virological response (SVR)-12 rate of 93.9%. We found no significant associations (P > 0.05) between SVR12 rate and the degree of fibrosis or the risk of hematological adverse events. The Fib-4 score could predict patients who developed hematological adverse events (anemia, leukopenia, and neutropenia) in the first month of treatment, but not in later stages. A Fib-4 cutoff value of 3.59 had high specificity for anemia, leukopenia, and neutropenia (85.1%, 87.2%, and 88.2%, respectively), but had low sensitivity for detecting the 3 events. In conclusion, the Fib-4 score may predict early hematological adverse effects in HCV-infected patients on IFN-based triple therapy.
Introduction
According to the most recent global prevalence report (2015), ∼1% of the world population (71.1 million individuals) is infected with hepatitis C virus (HCV) (Blach and others 2017). Although the global prevalence of HCV has been decreasing, HCV-related mortality has been increasing (Ly and others 2016). Chronic HCV infection often leads to cirrhosis, liver cell failure, and hepatocellular carcinoma (HCC) (Petruzziello and others 2016). Before the introduction of direct-acting antiviral (DAA) agents, the standard pharmacotherapy for chronic HCV infection was a combination of ribavirin (RBV) plus pegylated interferon (PegIFN) (Ward and Kugelmas 2005). This combination achieved a sustained virological response (SVR) rate that reached 50% in HCV genotypes 1 and 4, and 80% in genotypes 2 and 3 (Poordad and Dieterich 2012). However, it has been associated with several adverse events that limited its use (Ward and Kugelmas 2005).
In 2013, sofosbuvir (a nucleotide analog inhibitor of HCV-RNA polymerase) was first approved, followed by daclatasvir, simeprevir, ledipasvir, grazoprevir/elbasvir, and ombitasvir/paritaprevir/ritonavir and dasabuvir (EASL 2018). These agents significantly increased the SVR12 rates (Ahmed and others 2017a, 2017b, 2017c, 2018) and led to significant reductions in liver-related and all-cause mortality rates (Gimeno-Ballester and others 2016).
Egypt has the highest HCV prevalence in the world (WHO 2011). According to the Egyptian Demographic Health Survey (Ministry of Health and Population [Egypt] 2015), 14.7% of Egyptians had positive anti-HCV antibody testing, whereas 8.5% had viremia (Razavi and others 2014). Among the 6 major HCV genotypes, genotype 4 is the most predominant in Egypt (Simmonds and others 1993), with genotype 4a as the dominant subtype (Ray and others 2000; Blach and others 2017). Since 2015, Egyptian patients adhered to the Ministry of Health protocol that uses IFN-based triple therapy of weekly PegIFN alpha, daily RBV, and daily sofosbuvir for 12 weeks (Gomaa and others 2017). This combination was associated with several hematological adverse events in HCV genotype 1 patients (anemia in 14%, neutropenia in 23%, and thrombocytopenia grade III in 4% as reported in the study by Kowdley and others 2013). These adverse events were found to reduce the treatment compliance and SVR, especially in patients with advanced degrees of fibrosis (Sherman 2012). Despite the introduction of DAA regimens, low-income countries with poor resources (in which the majority of HCV infection burden exists) still use IFN-based regimens to treat HCV infection (Hlaing and others 2016).
The Fibrosis-4 (Fib-4) index is a formula that predicts the degree of liver fibrosis based on the standard biochemical values of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and platelet count and age, thus providing a non-invasive, simple, rapid, and low-cost test, with high sensitivity and specificity in detecting liver fibrosis. The Fib-4 was initially developed in 2006 by Sterling and others to measure the degree of fibrosis in patients co-infected with HCV/HIV (Sterling and others 2006). Several studies later established its accuracy in assessing the degree of fibrosis in HCV mono-infection (Vallet‐Pichard and others 2006; Adler and others 2008). The threshold value of <1.45 has a sensitivity of 74% and specificity of 80% in excluding significant fibrosis. A threshold value of >3.25 has a specificity of 98% in confirming cirrhosis (Vallet-Pichard and others 2007).
Compared with other noninvasive markers of fibrosis (whether morphological as elastometry/Fibroscan or biochemical as FibroTest), the Fib-4 index is easier to calculate (results are available within the same patient visit), less costly (does not require a specific device as Fibroscan), and does not require standardization (as FibroTest) (Adler and others 2008; Özkara and Övünç 2011).
The aim of this study was to evaluate the association between Fib-4 index and the risk of hematological adverse events in Egyptian patients with chronic HCV infection, undergoing IFN-based triple therapy and to determine the SVR12 of HCV to such therapy and its relation to the fibrosis degree as assessed by Fib-4.
Methods
Study design
We performed an observational prospective study to compare Fib-4 scores in chronic HCV patients who developed hematological adverse events versus those who did not upon treatment with IFN-based triple therapy. All patients were recruited from the outpatient clinic at Damietta Fever Hospital, Damietta, Egypt, between January and September 2015. Informed verbal consents were obtained from all participants before enrollment and were then documented by the attending physician. All procedures, involving human participants in this study, were performed in accordance with the Declaration of Helsinki 1964 and its later amendments.
Patients
A total of 120 HCV-infected patients (genotype 4) who received triple therapy in the form of weekly PegIFN-α, daily RBV (1,000 mg in patients <75 kg or 1,200 mg in patients ≥75 kg), and daily sofosbuvir (400 mg) for 12 weeks were included in this study.
Inclusion criteria
Patients were enrolled in this study if they had all the following criteria: age between 18 and 70 years, HCV-RNA positivity, treatment naïve or treatment experienced, baseline hemoglobin >13 g/dL for men and >12 g/dL for women, with total leukocyte count (TLC) >4,000/mm3, absolute neutrophil count (ANC) >1,500/mm3, and platelets count >150,000/mm3.
Exclusion criteria
Patients with any of the following criteria were excluded: pregnant women, women in childbearing age with no effective contraception, patients with advanced kidney disease (serum creatinine >2.5 mg/dL and/or creatinine clearance <60 mL/min), autoimmune diseases, uncontrolled depression or mental illness, decompensated liver failure (Child–Turcotte–Pugh score >7 as illustrated in Supplementary Table S1, glycated hemoglobin (HbA1c) >8.5%, patients with decompensated cardiac or pulmonary disease, a history of ascites or encephalopathy, and those with active HCC (except after successful treatment with stable condition for at least 1 month).
To confirm the lack of the previous exclusion criteria, we used abdominal ultrasonography (Ultrasonic; Sonix SP, Canada, 2010) and triphasic spiral CT scan (Balance Somatom; Spiral CT Siemens, 1999). Moreover, we performed pregnancy tests for women in the childbearing age, and antinuclear antibody, thyroid-stimulating hormone (TSH), and echocardiogram for all patients. Serum creatinine was determined according to Taylor (1989).
In addition, serum alpha-fetoprotein (AFP) levels were quantified using chemiluminescence quantitative immunoassay kits and the IMMULITE automated quantitative immunoassay analyzer (Siemens Healthcare Diagnostic Products, Ltd) (Gurakar and others 2011). For the enzymatic determination of fasting blood glucose, we used the glucose PAP SL kit manufactured by ELITech, France according to Trinder (1969). Whole blood was used in a latex-enhanced immunoassay to quantify HbA1c and the samples' optical density was assessed at a wavelength of 430 nm (Owen 2015).
Outcomes
Liver status and HCV quantification
The follow-up continued through w1, w2, w4, w8, w12 of treatment and at w12 posttreatment. At each follow-up visit, we checked the liver enzymes [AST, ALT according to Bergmeyer and others (1978)], serum albumin [according to Grant and Kachmar (1976)], bilirubin [spectrophotometrically using Hitachi 902 analyzer according to Webster (1974)], and prothrombin time (using blood coagulometer model SEAC S2; Biostec Liquiplstin, Egypt). The Abbott Real-Time (RT-qPCR) kit was used to quantify HCV-RNA in serum samples at w4 and w12 of treatment and w12 posttreatment (Myers and Gelfand 1991). The Fib-4 score was calculated using the following equation: [Age (years) × AST (U/L)/√ALT (U/L) × PLT (109/L)] (Sterling and others 2006).
Hematological indices
The complete blood count was determined by Cell Dyn 1800 (Abbott Diagnostics, IL). The blood hemoglobin (Hb) concentration was determined by photometric quantification of cyanmethemoglobin at 540 nm (Amatuzio and others 1962). During each visit, hematological adverse events were recorded and graded according to the Common Terminology Criteria for Adverse Events version III (Supplementary Table S2) (Dueck and others 2015).
Statistical analysis
We calculated the sample size in this study based on the number of patients who attend Damietta Fever Hospital on an annual basis, assuming a power of 95% and an alpha error level of 0.05. For this calculation, we used the “StatCalc” option in the “Epi Info” software, developed by the Centers for Disease Control and Prevention. We used the IBM Statistical Package for the Social Sciences (version 16.0) for data analysis. Continuous parametric data were expressed as mean ± standard deviation (SD), whereas nonparametric data were expressed as median (min-max). Categorical data were expressed as frequencies (percentages). Continuous variables were tested for normality using the Shapiro–Wilk test. The Mann–Whitney U-test was used to compare 2 groups with nonparametric data and the independent t-test was used for normally distributed data. Categorical variables were compared using the Chi-square (χ2) test and Fisher's exact test for parametric and nonparametric data, respectively. All tests were 2 tailed. The receiver operating characteristic (ROC) curves were used to determine the cutoff points for Fib-4 in detecting hematological adverse events. A P-value ≤0.05 was considered statistically significant.
Results
Baseline demographic and biochemical characteristics
A total of 120 Egyptian HCV-infected patients, attending Damietta Fever Hospital were enrolled in this study. The mean age in the enrolled participants was 52.4 (±6.29) years and the majority of patients were men (57.5%). The mean BMI was 30.17 (±3.72) kg/m2. According to the liver biopsy results of 86 enrolled patients, 51 (42.5%) patients were cirrhotic and 35 (29.1%) patients were noncirrhotic. The majority of patients were treatment naïve (n = 80; 66.7%). The baseline values of all measured hematological parameters and Fib-4 (median = 2.43, range [0.83–5.2]) were within the normal ranges (Table 1).
Demographic and Baseline Biochemical Indices of Enrolled Patients
AFP, alpha-fetoprotein; ALT, alanine aminotransferase; ANC, absolute neutrophil count; AST, aspartate aminotransferase; BMI, body mass index; Hb, hemoglobin; HbA1c, glycated hemoglobin; TSH, thyroid-stimulating hormone; WBCs, white blood cells.
Virological outcomes of treatment
After the initiation of treatment, 95% of patients tested negative qPCR at w4 (rapid virological response, RVR), and 95.8% at w12 of treatment (end of treatment response, ETR). At w12 post-treatment, 5 positively tested patients were missed to follow-up. Among the remaining 115 patients, 108 (93.9%) tested negative qPCR and 8 (6.1%) experienced viral relapse. Older patients were at higher risk of viral relapse (P = 0.04). The analysis of all biochemical and hematological indices (including AST, ALT, albumin, bilirubin, prothrombin, AFP, TSH, creatinine, Hb, white blood cells, ANC, and platelets) showed no significant differences between patients who achieved RVR, ETR, or SVR12 and those who did not (Table 2).
Association Between Virological Response (qPCR) with Biochemical Indices, Fib-4, and Demographic Factors of Patients at w4 (RVR), w12 (ETR) of Treatment, and w12 Posttreatment (SVR12)
Categorical data are described as frequencies and percentages. All quantitative parameters are described as median, except Hb, WBCs, platelets, albumin, and prothrombin (described as mean ± SD).
Analysis by Fisher's exact test.
Significance at P < 0.05.
Association between hematological outcomes and virological response
All over the follow-up period, 20 patients (16.7%) developed anemia, 52 patients (43.3%) developed leukopenia, 82 patients (68.3%) developed neutropenia, and 12 patients (10%) developed thrombocytopenia. By w12 of treatment, 3, 2, and 8 patients have developed grade III anemia, leukopenia, and neutropenia, respectively (Supplementary Table S3). The difference in the progression of adverse hematological events was insignificant between patients who achieved SVR12 and those who did not (total 115 after withdrawals) (Table 3).
Association Between the Frequency of Hematological Adverse Events and SV12 in the Enrolled Hepatitis C Virus-Infected Patients on IFN-Based Triple Therapy
All presented data are frequency and percentage of adverse effects among patients who achieved SVR12 and those who did not. Analysis by Fisher's exact test.
Association of Fib-4 score with the RVR, ETR, and SVR12
Our analysis showed no significant association between liver fibrosis (as assessed by Fib-4 score) and the achievement of RVR (P = 0.72), ETR (P = 0.95), or SVR12 (P = 0.85) (Fig. 1).

Fib-4 in patients who achieved negative qPCR at
Association between Fib-4 score and the development of hematological adverse events
Higher Fib-4 scores were significantly associated with the development of anemia (P = 0.03), leukopenia (P = 0.003), and neutropenia (P = 0.02) at w4 of treatment (Fig. 2a–c). A 3.59 cutoff point for Fib-4 score showed significant association with the development of the 3 events at w4 of treatment (P = 0.004, 0.01, and 0.03 for anemia, leukopenia, and neutropenia, respectively). At this cutoff point, Fib-4 scores displayed low sensitivity in detecting anemia, leukopenia, and neutropenia (57.1%, 34.8%, and 28.2%, respectively), but had high specificity in detecting the 3 events (85.1%, 87.2%, and 88.2%, respectively) (Table 4). Interestingly, no significant association was found between Fib-4 scores and the risk of thrombocytopenia at w4 of treatment (P = 0.86). Figure 3 shows the ROC curves for using Fib-4 score in the prediction of anemia, leukopenia, and neutropenia at w4 of treatment.

Box plots representing Fib-4 scores in
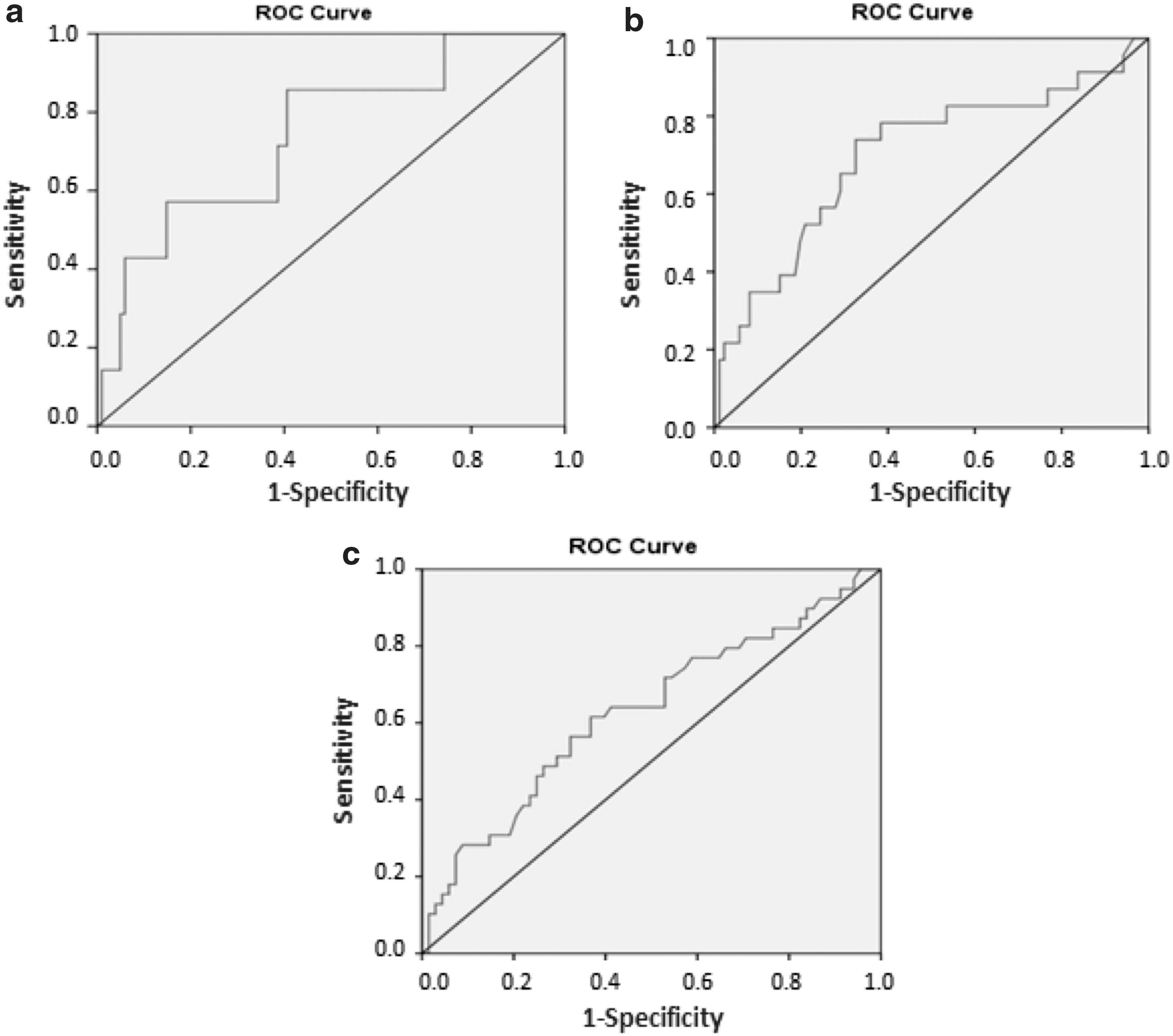
Receiver operator curve for Fib-4 diagnostic value in detecting
Fib-4 Cutoff (a) Determination, (b) Sensitivity, Specificity, Positive and Negative Predictive Values for a 3.59 Fib-4 Score to Predict Anemia, Leukopenia, and Neutropenia in Hepatitis C Virus-Infected Patients on IFN-Based Triple Therapy
Data are given as frequencies and percentages.
NPV, negative predictive value; PPV, positive predictive value.
Our analysis showed no significant associations between Fib-4 scores and the development of anemia, leukopenia, and neutropenia at w12 of treatment. Similar results were obtained at w12 post-treatment (P = 0.08, 0.09, 0.32, and 0.86 for anemia, leukopenia, neutropenia, and thrombocytopenia, respectively). This indicates that higher Fib-4 scores are significantly associated with the development of hematological adverse events early in the course of treatment, but not in the later stages (w12 of treatment and w12 posttreatment).
Discussion
The goal of antiviral therapy in HCV-infected patients is to cure the infection and achieve a steady SVR. This can reduce the risk of liver-related mortality and hepatic decompensation (by 70%–80%) and the risk of HCC by 75% at most stages of fibrosis (Smith and others 2012). Recently, treatments based on sofosbuvir have become the gold standard of care, with different levels of evidence supporting different regimens (Lawitz and others 2013b). In our study, we included patients infected with HCV genotype-4, who were on triple therapy (sofosbuvir/Peg-IFN/RBV). Our analysis showed that this regimen achieved RVR and ETR rates of 95% and 95.8%, respectively.
At w12 posttreatment, the SVR rate was 93.9% with a relapse rate of 6.1%. This response rate is similar to that reported by Lawitz and others (2013a). Moreover, real-life results reported in 8742 Egyptian patients with HCV (genotype 4; 35% cirrhotics and 27.2% treatment-experienced), receiving the same triple therapy, are similar with an overall SVR12 of 94%, treatment failure rate of 1.6%, and relapse rate of 4.4% (Elsharkawy and others 2017). However, a recent study of 205 Egyptian patients reported a 100% SVR12 with sofosbuvir and RBV combination therapy for 24 weeks (Nagaty and El-wahab 2017). This difference could be because of the variation in sample size and baseline characteristics in the enrolled patients. On the other hand, our results (with triple therapy) are higher than the SVR rates obtained in patients treated with dual therapy (PegIFN and RBV) (Taha and others 2010; Esmat and others 2014).
Interestingly, we did not find significant differences in SVR12 rates between cirrhotic and noncirrhotic patients (as assessed by Fib-4). This finding is in agreement with previous studies that did not find an association between Fib-4 scores and SVR12 (Lawitz and others 2013b; Nagaty and El-wahab 2017). However, the opposite was reported by the National Egyptian Committee for Control of Viral Hepatitis, which suggested lower SVR rates associated with higher Fib-4 scores (Doss and others 2015). Likewise, Jensen and others (2014) reported lower SVR4 rates among cirrhotic (70%) versus noncirrhotic (90%) patients, whereas Bacon and others (2014) reported SVR12 rates of 62% in cirrhotic patients versus 76% in non-cirrhotic patients. In accordance with Doss and others (2015), we did not find significant difference in SVR rates between treatment-naïve and experienced patients.
Relatively high rates of hematological adverse events (anemia, leukopenia, neutropenia, and thrombocytopenia) were reported in our study. Unlike IFN-free regimens, IFN-containing regimens are associated with higher rates of hematological adverse events (Gilead Sciences 2013; Solbach and Wedemeyer 2015). Similar to previous studies, we found female sex, older age, higher BMI, and lower baseline hemoglobin levels to be significantly associated with higher risk of developing anemia after IFN-containing therapy (Hayat and others 2009; Butt and others 2011; Fawzy and others 2013). On the other hand, achieving SVR was not associated with the development of hematological adverse events, which is similar to previous findings (Mancino and others 2010).
Previous studies have suggested a possible association between hematological adverse events after IFN-based therapy and the degree of cirrhosis (whether measured by Fib-4 score or by other means) (Sherman 2012; Hafez and others 2014). Our study is the first to assess the Fib-4 score as a predictor of the risk of these adverse events. We concluded that a Fib-4 cutoff value of 3.59 can provide a reliable, fast, and easy measure to predict the risk of developing anemia, neutropenia, and leukopenia, early in the course of treatment (w4). We found this test to have an acceptable specificity. However, the main limitation is its relatively low sensitivity, making continued follow-up of patients testing negative by the Fib-4 index advisable. In contrast with previous reports, the Fib-4 score was not associated with the risk of thrombocytopenia (Sherman 2012; Hafez and others 2014). However, a possible explanation for this is the high baseline platelets count in our sample.
Limitations and Future Research Recommendations
Although our study is the first (to our knowledge) to investigate the diagnostic value of Fib-4 in predicting the hematological adverse events related to IFN-based therapy, it has some limitations. First, the relatively small sample size reduces the generalization of our results. Second, to exclude confounding variables that may alter the risk of hematological adverse events, we excluded patients with kidney and autoimmune diseases. Therefore, our results are not generalizable to subgroups of HCV-infected patients who have other comorbidities. Future studies should use a larger sample size and enroll HCV-infected patients with various comorbidities. Moreover, combining Fib-4 with another score of liver function may improve its sensitivity; however, this needs to be tested in future studies.
Conclusion and Significance
After the introduction of new DAA regimens, the use of IFN-based regimens is no longer recommended because of the associated high risk of adverse events. However, in many developing countries with poor resources, IFN-based regimens are still in use. Therefore, it is important to follow these patients strictly to detect and manage possible adverse events. Measuring the Fib-4 score before initiation of treatment can provide a reliable measure with high specificity to predict the risk of developing anemia, leukopenia, and neutropenia in the early course of treatment.
Footnotes
Acknowledgments
The authors thank the National Committee for Control of Viral Hepatitis, Egypt, for approving this work.
The authors received no funding from private or non-for-profit organizations. The authors declare no honorarium, grant, or other form of payment was given to anyone to produce the article.
Ethics Approval
All patients were residents in Damietta Fever Hospital, Damietta, Egypt. Informed verbal consents were obtained from all participants before enrollment in the study, and the verbal consents were then documented by the attending physician. All procedures performed in this study involving human participants were in accordance with the ethical standards of the Declaration of Helsinki 1964 and its later amendments.
Authors' Contributions
All authors contributed to conception, design, data analysis, and writing the article. MA provided the ENDNOTE X8 software for the production of this article.
Author Disclosure Statement
All authors declare that they have no conflict of interest.