
Abstract
Pentraxin-3 (PTX-3) is derived from the secretion of macrophages, neutrophils, endothelial cells, epithelial cells, and vascular smooth muscle cells, which can regulate the immune activity of macrophages. The objectives of our study were to investigate the serum PTX-3 levels and analyze this correlation with vasculitis (Vas), with hypertension. A total of 155 cases consisting 51 patients with Vas [including 7 cases of takayasu arteritis (TA), 24 cases of polyarteritis nodosa (PAN), and 20 cases of antineutrophil cytoplasmic antibody-associated Vas (AAV)] were screened by angiography and/or biopsy; 46 patients with essential hypertensions (PH) and 58 healthy controls (HC) were enrolled in this study from January 2013 to December 2016. Serum PTX-3 levels were determined by enzyme-linked immunosorbent assay. Compared with the HC and PH, the serum PTX-3 levels in systemic Vas were significantly higher (both P < 0.001, 4.42 ± 0.95 vs. 2.67 ± 0.92 and 4.42 ± 0.95 vs. 2.95 ± 0.60), and there was no significant difference between HC and essential hypertension (P = 0.886, 2.67 ± 0.92 vs. 2.95 ± 0.60). There was no significant difference of PTX-3 levels among TA, PAN, and AAV, as well as active and inactive groups, and renal and nonrenal groups even if they had a significant difference from EH and HC, respectively. There was no significant correlation between PTX-3 levels and blood pressure, erythrocyte sedimentation rate, or Birmingham Vasculitis Activity Score. Receiver operating characteristic analysis has shown that the best cutoff point was at 3.618 ng/μL; the sensitivity and specificity were calculated as 84.3% and 93.5% for the diagnosis of Vas from heath control, and the best cutoff point was at 3.425 ng/μL, The sensitivity and specificity were calculated as 88.2% and 82.6% for the diagnosis of Vas from essential hypertension. Serum PTX-3 levels were significantly higher in patients with Vas than essential hypertension or health control, and elevated PTX-3 levels can help identify Vas patients from healthy or essential hypertensive populations.
Introduction
Systemic vasculitis is a rare and disabling disease. The clinical manifestations are different, varied and complex systemic vasculitis often involving multiple systems, such as skin, kidneys, lungs, and nervous system, and cause multiple organ dysfunction and hypertension syndrome, and seriously threaten the life of patients.
Within each form of vasculitis (Vas), there is great diversity in the severity of disease and the extent of organ-system involvement. Systemic Vas has complex and varied clinical manifestations; angiography and biopsy are the primary means of diagnosis and assess disease activity in small- and medium-vessel Vas, but they are invasive tests that have greater damage to the patient's body, and the lesion of Vas is periodic and segmental, so the positive rate of biopsy is lower. The early symptoms of Vas are atypical, previous indicators to diagnose and assess disease activity such as blood sedimentation and C-reactive protein (CRP) have poorer specificity.
Due to the lack of specific laboratory inspection, the diagnosis and assessment of disease activity of Vas is difficult and challenging. Therefore, a new diagnostic biomarker is needed to identify Vas for more effective targeted treatment. Pentraxin-3 (PTX-3) and CRP belonged to a member of the pentraxin family, CRP is a systemic inflammatory marker protein; however, PTX-3 belongs to the same family as CRP and is more specific, and some report suggested that the CRP was in normal range when PTX-3 was higher in some disease.
PTX-3 is derived from the secretion of macrophages, neutrophils, endothelial cells, epithelial cells and vascular smooth muscle cells (Alibaz-Oner and others 2016), which can regulate immune activity of macrophages, participate in the classic pathway to complement activates and acute phase of the immune response, and is associated with the clinical process and activity of autoimmune diseases such as Vas. Previous research has shown that Takayasu arteritis (TA) had higher plasmatic PTX-3 and CRP concentrations than healthy controls (HC), and the activity of the disease is associated with PTX-3, but not CRP (Tombetti and others 2014). In addition, PTX-3 also has a high level of expression in the cytoplasmic antibody-associated glomerulonephritis. The PTX-3 level may be a marker of antineutrophil cytoplasmic antibody (ANCA) activity, especially when serum CRP levels are within normal range (Ishida and others 2015).
Previous research has shown that the production of PTX-3 is stimulated by interleukin (IL)-1 and tumor necrosis factor (TNF) (Bassi and others 2009; Simon and others 2016), IL-6 is not known to directly induce PTX-3 expression and release (Sağ 2018; Sağ 2018a); however, it could induce the generation of TNF-α and IL-1β, thus indirectly modulating PTX-3 levels (Tombetti and others 2014). Also, recent studies have shown that serum PTX-3 is not associated with increased IL-1, IL-6, IL-8, and TNF- levels (Sağ 2018).
In the previous studies, PTX-3 has an important function in TA and a few small-vessel Vas. Thus, we aimed to investigate the serum PTX-3 levels and analyze this correlation with Vas with hypertension.
Methods
Patients
We reviewed all patients admitted to our center for the etiology screening of hypertension between January 2013 and December 2016. The diagnosis of systemic Vas is based on the patient's clinical manifestations (such as malaise, weight loss, fever, arthralgia, and myalgia), laboratory tests (such as elevated erythrocyte sedimentation rate, CRP, ANA, ANCA, and other acute phase reactants, proteinuria, hematuria, and increased creatinine), and typical imaging finding (such as artery occlusion and stenosis or arterial saccular or fusiform microaneurysms) and pathological biopsy (such as crescent formation or vascular wall thickening, stenosis, surrounded by inflammatory cell infiltration, and the lack of immune complex deposition) (Fig. 1). All Vas were diagnosed by a rheumatologist and fulfilled the American College of Rheumatology (ACR) 1990 criteria or the 2012 revised International Chapel Hill Consensus Conference classification criteria for polyarteritis nodosa (PAN) and antineutrophil cytoplasmic antibody-associated Vas (AAV) (Leavitt and others 1990; Lightfoot and others 1990; Masi and others 1990; Bacciu and others 2006; Mohammad and others 2007; Jennette 2013).
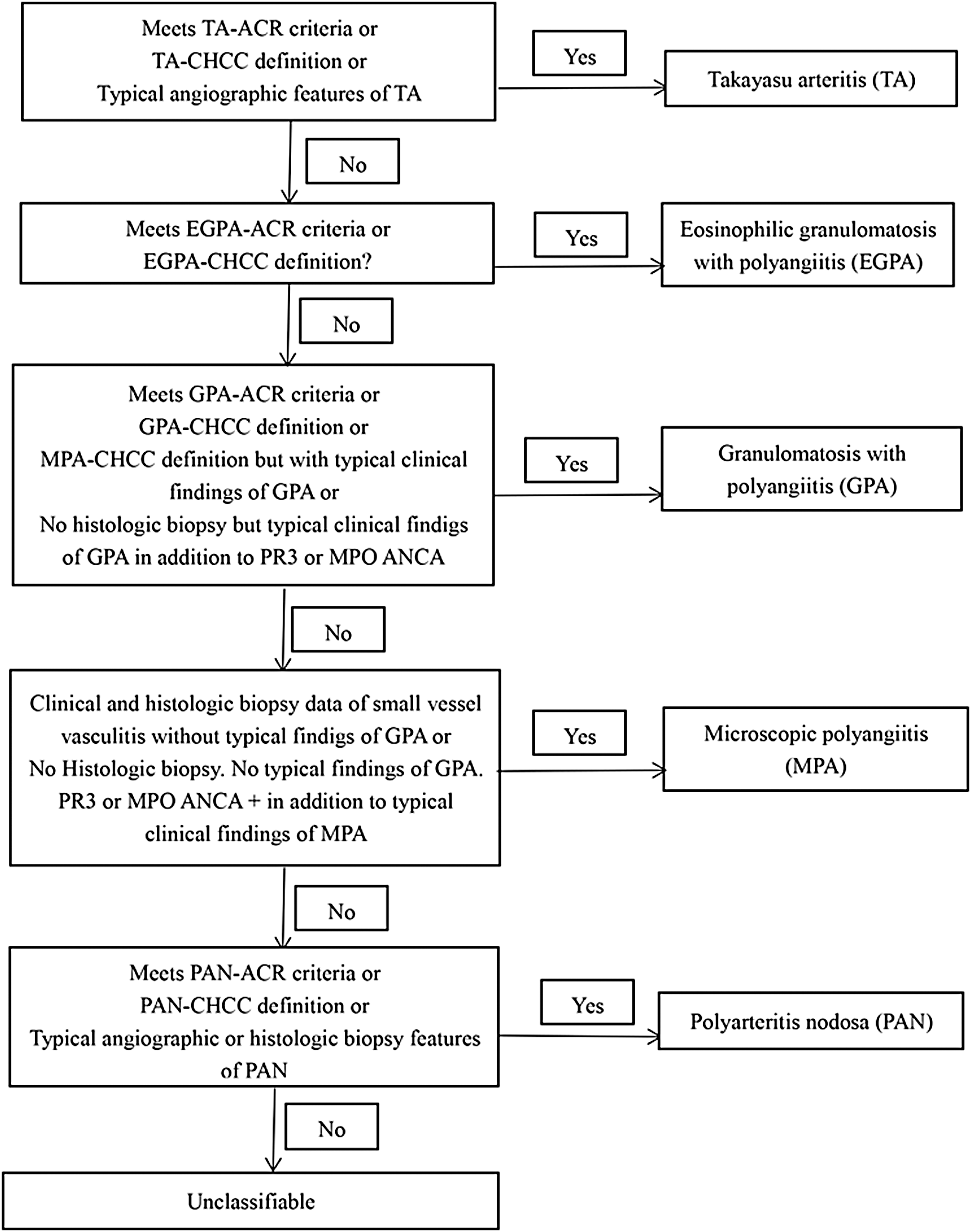
The criteria of diagnosis of systemic vasculitis. ACR, American College of Rheumatology; ANCA, antineutrophil cytoplasmic antibody; CHCC, Chapel Hill Consensus Conference; EGPA, eosinophilic granulomatosis with polyangiitis; GPA, granulomatosis with polyangiitis; MPA, microscopic polyangiitis; MPO, myeloperoxidase; PAN, polyarteritis nodosa; PR3, proteinase 3; TA, takayasu arteritis.
Patients with secondary Vas, systemic lupus erythematosus, rheumatoid arthritis, malignancy, infection, or any other coexisting renal disease, such as antiglomerular basement membrane nephritis, IgA nephropathy, diabetic nephropathy, or lupus nephritis, and patients with incomplete data were excluded.
We consecutively selected 51 patients with systemic Vas (including 7 cases of TA, 24 cases of PAN, and 20 cases of AAV).
Age- and sex-matched HC were recruited from the Center for Medical examination of the People's Hospital of Xinjiang Uygur Autonomous Region after excluding those with evidence of any acute or active chronic infection as well as diseases that cause vascular damage, such as hypertension, diabetes, and atherosclerosis, by clinical examination, and eventually 58 HC were included.
We recruited 46 essential hypertension patients. The diagnosis of hypertension was established if patients were on antihypertensive medication or if the mean of 3 measurements of systolic blood pressure was ≥140 mmHg or diastolic blood pressure was ≥90 mmHg in different days, respectively. Secondary hypertensive patients, such as aldosterone-producing adenoma, aldosterone carcinoma, secondary hyperaldosteronism, Cushing syndrome, hypertension kidney disease, renal vascular hypertension, and pheochromocytoma were excluded.
Ethical approval of the study protocol
Written informed consent was obtained from all participants. All participants explicitly provided permission for collection of relevant clinical data. This study was approved by the Ethics Committee of the People's Hospital of Xinjiang Uygur Autonomous Region (Urumqi, China). The number of Ethical approval is KY2018011866. It was conducted according to the standards of the Declaration of Helsinki.
Data collection and measurements
All information of clinical data came from the patient's medical records during hospitalization (including demographics, clinical, biologic, imaging, and biopsy findings).
The following clinical manifestations were recorded:
General symptoms (fever, weakness, asitia, and weight loss); myalgias and arthralgias; peripheral neuropathy (mononeuritis multiplex or polyneuropathy); central nervous system involvement; urologic and renal involvement (orchitis, dialysis, peripheral limb edema, and recent-onset or severe hypertension); cutaneous symptoms (nodules, purpura, erythra, and livedo); alimentary manifestations (nausea, vomiting abdominal pain, hemorrhage, pancreatitis, and peritonitis); cardiovascular involvement (pectoralgia, cardiomyopathy, pericarditis, and ischemic); ophthalmologic involvement (retinal Vas/exudates, visual impairment, conjunctivitis, keratitis, and uveitis); and pulmonary involvement (cough, hemoptysis, dyspnea, pleural effusion, and lung infiltrates).
Biologic parameters
Blood cell counts; renal parameters [proteinuria, hematuria, 24-h proteinuria, and serum creatinine (Scr)]; erythrocyte sedimentation rate (ESR); CRP; hypersensitive C-reactive protein (Hs-CRP); and the ANCA testing by indirect immunofluorescence and enzyme-linked immunosorbent assay (ELISA).
Imaging examination
The angiographies result as abnormal when showing blood vessels are sparse, irregular stenoses, and/or microaneurysms; chest X-ray showed that nodules and infiltrating lesions and/or cavity. The results were determined by 2 radiologists.
Biopsy findings
The biopsy showed inflammatory infiltration of small and medium vessels and/or formation of crescent immunofluorescence demonstrated no or little immune complex deposition in the mesangial area, vascular loops, or small vascular walls. The results were determined by 2 pathologists.
Definitions of disease activity
Disease activity was assessed in accordance with the third version of Birmingham Vasculitis Activity Score (Leavitt and others 1990; Lightfoot and others 1990; Masi and others 1990; Bacciu and others 2006; Mohammad and others 2007; Jennette 2013; Mukhtyar and others 2009).
Definitions of renal injury
Renal injury was defined as the presence of any hematuria and/or proteinuria, and/or Scr increased. Hematuria was defined as more than 5 red blood cells per high-power field in urine sediment. Proteinuria was defined as more than 1+ in urine routine and/or 24-h urine collection containing more than 150 mg of proteins. Scr increased was defined as male Scr >104 μM or female Scr >84 μM.
Measurement of PTX-3 in human serum samples
Venous blood was collected into serum tubes and allowed to clot at room temperature before being centrifuged at 3,000 r/min for 10 min at 4°C. Serum was removed and stored at −80°C until assayed. Serum PTX-3 levels were determined by ELISA (Uscn Life Science, Inc., Wuhan, China) following the manufacturer's instructions. The results of serum PTX-3 levels are expressed in ng/μL.
Statistical analysis
Analyses were performed using SPSS software version 20.0 (IBM Corp, Armonk, NY) and graphs were built using Graph Pad Prism version 5.0 (GraphPad Software, La Jolla, CA). Data were expressed as mean ± standard deviation (for data that were normally distributed) or median and interquartile range (for data that were not normally distributed). Differences of quantitative parameters between groups were assessed using the t-test (for data that were normally distributed) or the nonparametric test (for data that were not normally distributed). Correlation between numerical data was calculated using Spearman's or Pearson's correlation coefficient. Receiver operating characteristic (ROC) curve analysis was used to identify optimal cutoff values of PTX-3. P values <0.05 were considered statistically significant.
Results
Baseline features of Vas patients, essential hypertension patients, and HC
In this study, of the 51 Vas patients, 29 were male and 22 were female, of the 46 essential hypertention patients, 31 were male and 15 were female, and of the 46 HC, 20 were male and 26 were female. The mean age of Vas patients, essential hypertension patients, and healthy controls was 40.22, 43.74, and 42.61 years, respectively. There was no significant difference between the 3 groups with respect to demographic characteristics (Table 1). Among Vas patients, 7 patients were diagnosed as TA, 20 patients were diagnosed as AAV, and 24 patients were diagnosed as PAN. Clinical and laboratory features of the 51 Vas patients, 46 essential hypertension patients, and 43 healthy controls included in the study are presented in Tables 1 and 2.
Demographic and Laboratory Features of Patients with Vasculitis, Essential Hypertension and Healthy Controls
Continuous variables are presented as median and interquartile range or as mean ± SD.
AAV, ANCA-associated vasculitis; ANCA, antineutrophil cytoplasmic antibody; BMI, body mass index; DBP, diastolic blood pressure; EH, essential hypertension; ESR, erythrocyte sedimentation rate; HB, hemoglobin; HC, healthy controls; Hs-CRP, hypersensitive C-reactive protein; PAN, polyarteritis nodosa; PLT, platelet; PTX-3, pentraxin-3; SBP, systolic blood pressure; Scr, serum creatinine; SD, standard deviation; SV, systemic vasculitis; TA, takayasu arteritis; Vas, vasculitis; WBC, white blood cell.
Clinical Features of Patients with Systemic Vasculitis
Continuous variables are presented as mean ± SD.
AAV, antineutrophil cytoplasmic antibody-associated vasculitis; BVAS, Birmingham Vasculitis Activity Score.
Serum PTX-3 levels of Vas are higher than essential hypertension and HC
The PTX-3 level in Vas is significantly higher than essential hypertension (EH) and HC (4.42 ± 0.95 vs. 2.92 ± 0.6 ng/μL, P < 0.001 between Vas and EH; 4.42 ± 0.95 vs. 2.67 ± 0.92 ng/μL, P < 0.001 between Vas and HC), There was no significant difference between EH and HC (2.92 ± 0.6 vs. 2.67 ± 0.92 ng/μL, P = 0.142). When Vas were divided into subgroups (TA, AAV, and PAN), we found that PTX-3 level in PAN is no significantly different between TA, AAV, and PAN (Fig. 2).
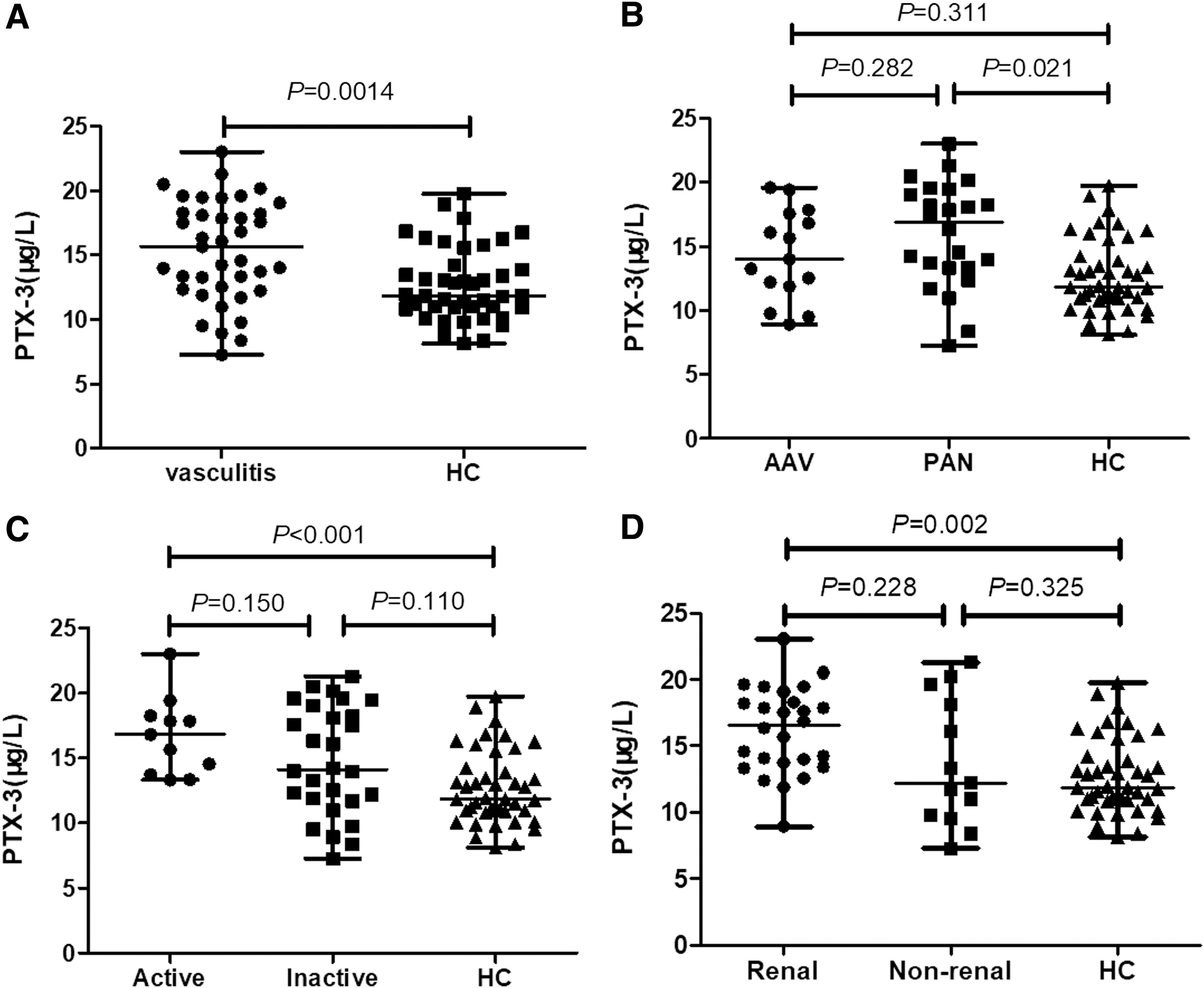
PTX-3 levels in different groups.
Serum PTX-3 levels in the Vas patients with active stage and inactive stage, or renal involvement patients and nonrenal involvement patients.
There was no significant difference in PTX-3 levels between the active stage and inactive stage (4.42 ± 0.16 vs. 4.41 ± 0.25 ng/μL, P = 0.978), and there was no significant difference between renal involvement patients and nonrenal involvement patients (4.30 ± 0.17 vs. 4.61 ± 0.22 ng/μL, P = 0.264) (Fig. 2).
Correlations of serum PTX-3 levels with clinical and laboratory variables
We evaluated the correlations between serum PTX-3 levels with clinical and laboratory variables in Vas. The results showed no significant correlation between PTX-3 levels and blood pressure, ESR, BAVS, or CRP (Fig. 3).
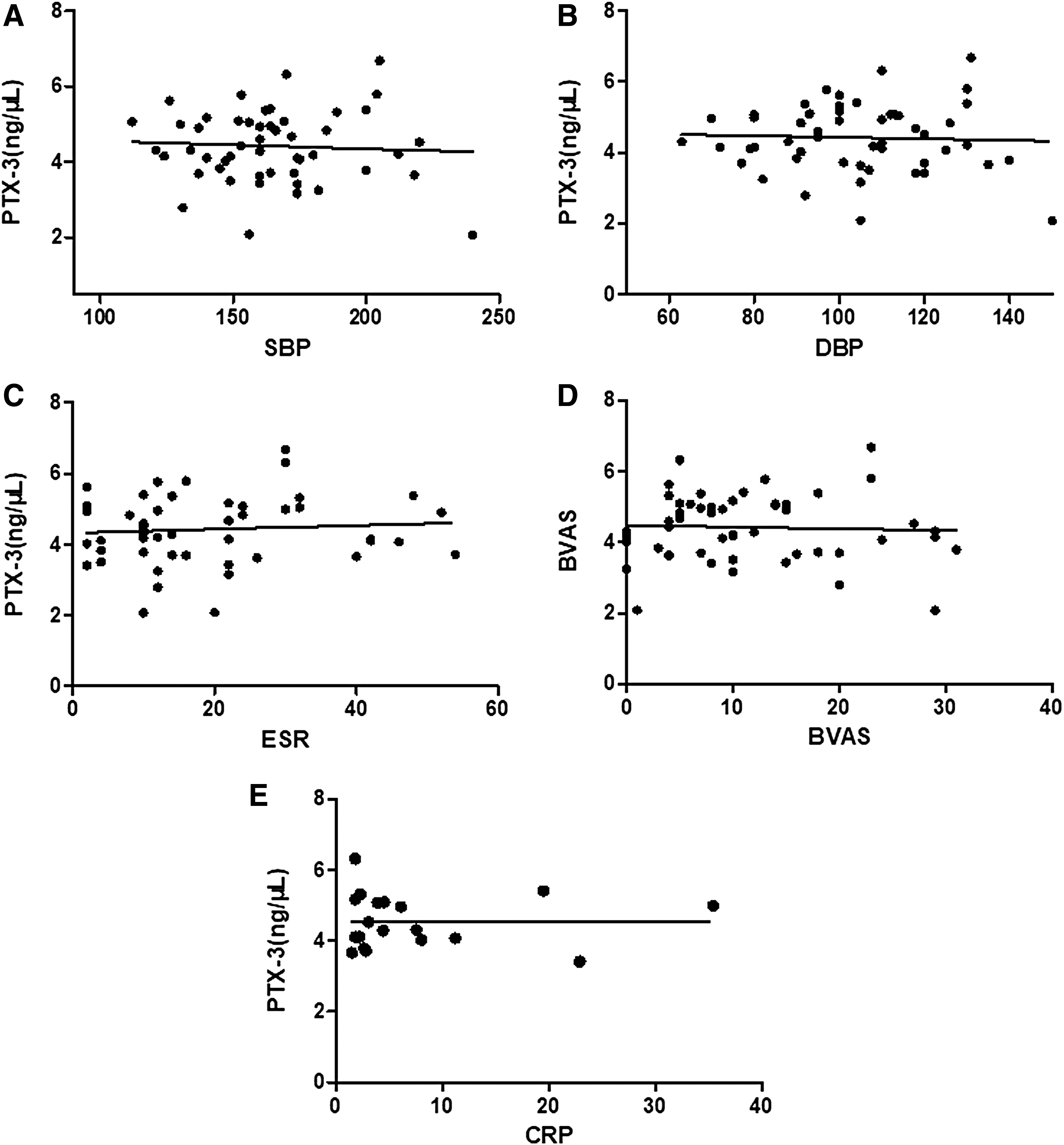
Correlations of PTX-3 levels with SBP
The ROC curve of serum PTX-3 levels in Vas
The ROC curve showed that the best cutoff value of serum PTX-3 levels was investigated by calculating ROC curves. For the diagnosis of Vas, the best cutoff point was 3.618 ng/μL. The sensitivity and specificity were calculated as 84.3% and 93.5% for the diagnosis of Vas from healthy control, and the best cutoff point was 3.425 ng/μL, The sensitivity and specificity were calculated as 88.2% and 82.6% for the diagnosis of Vas from essential hypertension. All estimated values are shown in Fig. 4.

The ROC curve of PTX-3. The ROC curve of the diagnosis of vasculitis from heath control
Discussion
Systemic Vas is an autoimmune disease with latent, multiorgan, and systemic injury. The representative subtypes mainly include TA, PAN, and AAV. Unfortunately, laboratory, imaging, and other common tests have limited ability to help clinicians solve these problems. Therefore, it is a challenge of the evaluation of clinical diagnosis and disease activity of systemic Vas. Reliable biomarkers are needed to help clinical diagnosis and assessment of small and medium angioinflammatory disease activities.
Pentraxins are a family of evolutionarily conserved, soluble, multifunctional, pattern recognition proteins characterized by a cyclic multimeric structure (Introna and others 1996). Pentraxins are classes of acute reactive protein that can recognize a series of exogenous substances. They are pivotal components of the innate immune system. Pentraxins are divided into 2 groups: short and long pentraxins (Deban and others, 2011; Moalli and others 2011). Short pentraxins are the conservative evolution protein with classical short-chain pentraxin proteins, including CRP and serum amyloid P component (SAP). They have a similar circular disk of 5 polymers, and the amino acid sequence is homologous. PTX-3 and other subsequently identified proteins represent the long pentraxin arm of the family. This molecule shares similarities with the classical, short pentraxins, but differs from them by the presence of an unrelated long N-terminal domain as well as in the fields of gene organization, cellular source, and ligands that it recognizes (Bottazzi and others 2006; Jaillon and others 2014; Roy and others 2017). In contrast to CRP and SAP, PTX-3 is considered a more efficient independent biomarker of inflammatory diseases because PTX-3 can undergo extra hepatic synthesis. PTX-3 is derived from the secretion of macrophages, neutrophils, endothelial cells, epithelial cells, and vascular smooth muscle cells, which can regulate the immune activity of macrophages (Shiraki and others 2016). When inflammation or immune attack occurs in the blood vessel wall, PTX-3 is also released in the first time, and macrophages are activated to different degrees to play a role in infiltrating into the blood vessel wall. PTX-3 also plays an important role in macrophage polarization (Pucci and others 2014) and switched M1 macrophages toward an M2 phenotype (Pucci and others 2014; Sun and others 2015). When Vas occurs, the macrophages activated, and fibrinoid necrosis and intimal hyperplasia occur in the vascular wall, leading to vascular stenosis.
In addition, PTX-3 acts as a precursor for antibodies by activating the complement and phagocytes to promote pathogen recognition. PTX-3 combined with a variety of soluble receptor ligands to participate in a variety of biological effects, such as immune prevention apoptosis, inflammation, and atherosclerotic vascular remodeling. PTX-3 participates in the classic way to complement activation, which may be the important mechanism of the inflammation. Studies have shown that PTX-3 can be used as a novel biomarker of cardiovascular diseases, infectious diseases, and chronic kidney diseases. Our results show that PTX-3 levels in Vas were higher than that in the control group. It is consistent with the research of Fausto and others (2001).
Further analysis showed that PTX-3 levels in Vas patients with active stage were significantly higher than HC group, while there is no significant difference between active stage and inactive stage. In previous study, Fazzini and others (2001) and Tombetti and others (2014) reported that compared with health control, PTX-3 level is higher in Wegener's granulomatosis, microscopic polyangiitis, and TA, while in nonactivity patients, PTX-3 levels is similar to those of control group. This research suggests that PTX-3 levels are associated with Vas and disease activity (Sahin and others 2017). However, another report found that The PTX-3 level is not associated with disease activity, The results are controversial with previous studies. Our research supports the latter result of previous studies. The lack of complete angiographic evaluation of the Birmingham score in our study of patients in Vas with hypertension may be another reason for the discrepancy with Sahin's findings.
Recent studies have shown that PTX–3 is not only related to the disease activity but also plays an important role in renal injury; PTX-3 inhibits acute renal injury-induced interstitial fibrosis through suppression of IL-6/Stat3 pathway (Lech and others 2013). Acute kidney injury increased PTX-3 protein in the kidney and the plasma (Chen and others 2012). The average level of serum PTX-3 in the discovery cohort of lupus nephritis was significantly higher than that in nonrenal involvement systemic lupus erythematosus group and normal controls, which was confirmed by the validation cohort (Pang and others 2016). In our study, PTX-3 level in renal injury patients is higher than the control group, but there is no significant difference between renal injury patients and nonrenal injury patients. This result is different from previous research, may be due to little sample size.
Further analysis showed that serum PTX-3 levels were not significantly correlated with blood pressure, ESR, or BAVS. These results might imply that PTX-3 levels could not reflect the severity of Vas.
Previous research has shown that patients with TA had higher plasmatic PTX-3 and CRP concentrations than HC. PTX-3 levels did not correlate with those of CRP (Tombetti and others 2014). Pentraxin3 and high-sensitive CRP are independent inflammatory markers (Nakajima and others 2010). The levels of CRP accurately reflect the burden of systemic inflammation, while PTX-3 is mainly produced at inflammatory sites. These results support the contention that PTX-3 reflects different aspects of inflammation than CRP. Our results show that PTX-3 level is not associated with CRP. This result supports the previous study.
Our study did have some limitations as well. Since our case group was from the Hypertension Center, there is a possibility of selective bias. In addition, our study lacked positive controls (such as systemic lupus erythematosus). Further validation is required to apply the results of this study to other populations.
Conclusion
Elevated PTX-3 is a risk factor for small- and medium-vessel Vas with hypertension and correlated with blood pressure level, but not associated with disease activity or renal injury.
Footnotes
Acknowledgments
This research was supported by the Region Natural Science Foundation of Xinjiang Uygur Autonomous (No. 2018D01C117). The authors are very grateful to Department of Rheumatology, Medical Examination Center, Department of Pathology, Department of Dermatology and Department of Nephropathy, and Xinjiang Uygur Autonomous Region People's Hospital for their contribution to this study. The authors are very grateful to 27th Scientific Meeting of the International Society of Hypertension for giving us an opportunity to present a summary, because part of the material in this article was published in the conference proceedings.
Author Disclosure Statement
No competing financial interests exist.