
Abstract
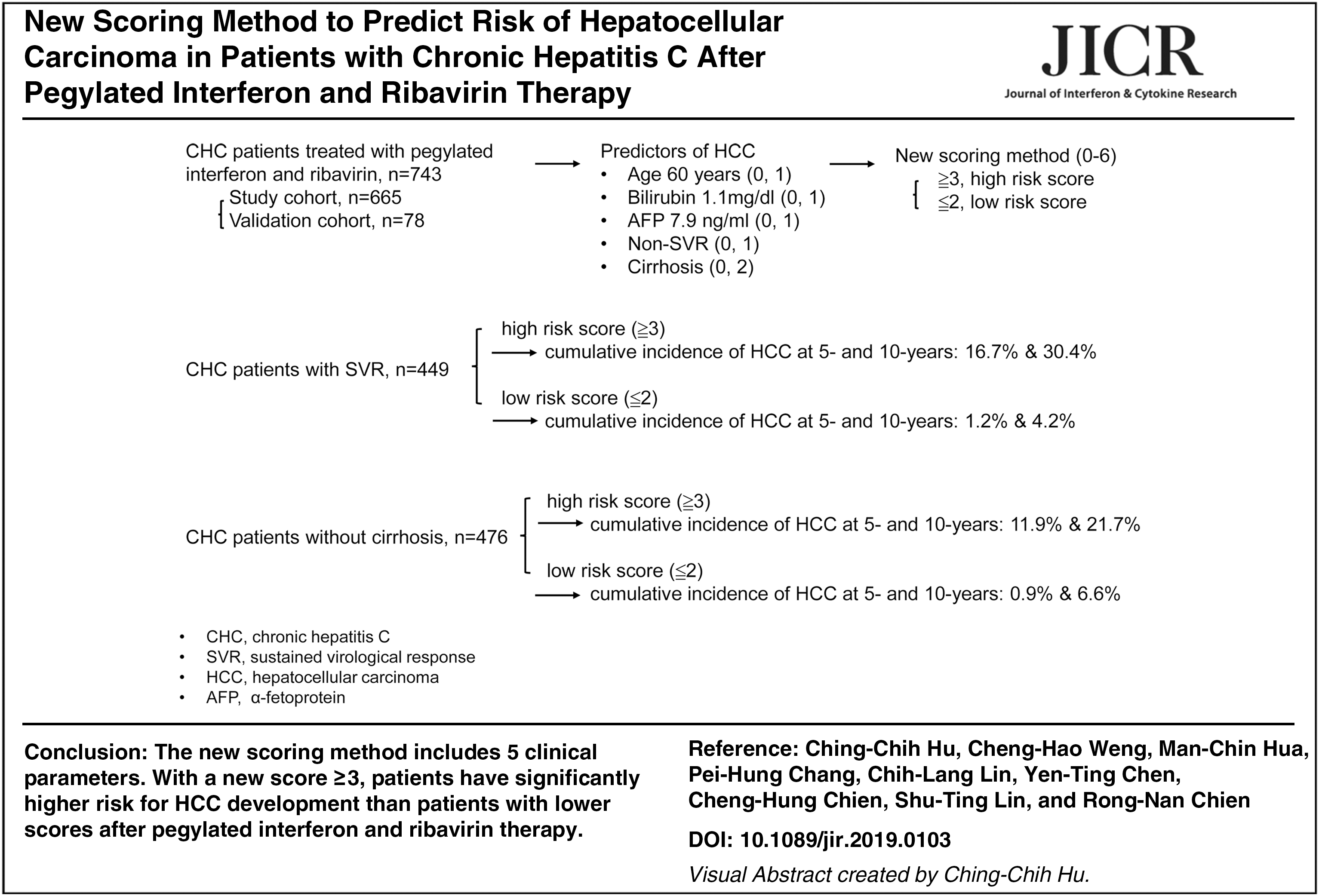
Antiviral therapy for chronic hepatitis C (CHC) infection using pegylated interferon and ribavirin (PR) therapy can reduce the risk of hepatocellular carcinoma (HCC). Our study developed a new scoring method for predicting HCC risk after PR therapy. Between 2002 and 2016, 743 PR-treated patients with CHC were enrolled. Significant predictors for HCC were identified using multiple Cox regression analysis in study cohort: treatment age ≥60 years (hazard ratio [HR]: 2.04, 95% confidence interval [CI] = 1.3–3.7), pretreatment bilirubin ≥1.1 mg/dL (HR: 1.99, 95% CI = 1.08–3.67), α-fetoprotein ≥7.9 ng/mL (HR: 2.44, 95% CI = 1.16–5.32), no sustained virological response (SVR; HR: 1.91, 95% CI = 1.05–3.45), and baseline cirrhosis (HR: 4.45, 95% CI = 2.07–9.73). These predictors form the new HCC prediction scoring method with an area under the receiver operating characteristic curve of 0.884, sensitivity of 86.2%, and specificity of 74%. In patients with CHC and SVR, the cumulative incidence of HCC at 5 and 10 years was 16.7% and 30.4%, respectively, in patients with high risk scores and 1.2% and 4.2%, respectively, in patients with low risk scores (P < 0.001). Patients with SVR and high risk scores after viral eradication should remain under an intensive surveillance program for HCC.
Introduction
Chronic hepatitis C virus (HCV) infection is a major global health problem, and an estimated 71 million people worldwide have the disease (Polaris Observatory 2017). A substantial proportion of patients with chronic hepatitis C (CHC) develop complications such as liver cirrhosis and hepatocellular carcinoma (HCC) (Perz and others 2006; Alter 2007; Fassio 2010). The seroprevalence rate of antibodies to HCV (anti-HCV) is 1%–5.5% of the adult population in Taiwan but may be even higher in hyperendemic areas (Chen and others 1990; Lee and others 2011).
Several risk factors are associated with HCC development in patients with CHC, including failure to achieve sustained virological response (SVR), male sex, relative old age at infection and during therapy, HCV genotype 1b, advanced fibrosis, low serum albumin levels and platelet counts, high α-fetoprotein (AFP) and alkaline phosphatase levels, and the presence of esophageal varices (Ikeda and others 1993; Tsukuma and others 1993; Bruno and others 2007a; Pradat and others 2007; Cardoso and others 2010; Morgan and others 2010; Aleman and others 2013; Asahina and others 2013; Rutter and others 2015).
Other studies have demonstrated that eradication of HCV through an interferon (IFN)-based regimen reduced the risk of HCC and improved patient survival rates (Cardoso and others 2010; Hsu and others 2013; Morgan and others 2013; Rutter and others 2015; Tada and others 2016). However, yet other studies have reported contrasting results (Coverdale and others 2004; Pradat and others 2007; Fernandez-Rodriguez and others 2010). Because pegylated IFN and ribavirin (PR) therapy greatly improves the rate of SVR in comparison with conventional IFN therapy, it had been the standard of care therapy for chronic HCV infection before the introduction of direct-acting antiviral agents (DAAs) (Manns and others 2001; Fried and others 2002; Hu and others 2013).
Although DAAs are currently the primary therapy, a high proportion of chronic HCV infections were successfully eradicated with PR therapy before the DAAs became commonly available. However, only a few studies have focused on assessing the risk of HCC development in patients with CHC after treatment with PR therapy (Chang and others 2012, 2013; Aleman and others 2013; Hu and others 2018). Therefore, this retrospective study elucidates the effect of PR therapy on the development of HCC and develops and validates a new scoring method for post-treatment HCC prediction in patients with CHC using clinical parameters and identifies high-risk patients, specifically ones with SVR, that warrant intensive monitoring after therapy.
Materials and Methods
Study population
From February 2002 to September 2016, 743 patients with CHC were enrolled in this study. Chronic HCV infection was defined as being seropositive for anti-HCV and HCV RNA for more than 6 months. Clinical and laboratory data were recorded for 3 months before initiation of PR therapy. Six hundred sixty-five patients who were negative for hepatitis B surface antigen (HBsAg) were assigned to the study cohort, and 78 patients who were positive for HBsAg but had serum HBV DNA levels less than 2,000 IU/mL were assigned to the validation cohort.
All patients received PR therapy for 24 or 48 weeks according to the reimbursement policy of the National Health Insurance program in Taiwan. Pegylated IFN-α-2a (180 μg) or weight-based pegylated IFN-α-2b (1.5 μg/kg) was prescribed. For HCV genotype-1b patients, the daily doses of ribavirin were 1,000 and 1,200 mg for patients with body weights <75 and ≥75 kg, respectively. For patients with CHC genotype non-1b, the daily ribavirin dose was 800 mg. SVR was defined as sustained undetectable serum HCV RNA determined through a polymerase chain reaction (PCR) study from the end of therapy to the end of a 24-week follow-up period.
Patients with HCC diagnosed before therapy, human immunodeficiency virus coinfection, toxic hepatitis, autoimmune hepatitis, primary biliary cirrhosis, or Wilson's disease were excluded. This study was approved by the Medical Ethics Committee of Chang Gung Memorial Hospital (Institutional Review Board approval number: 201600519B0) and was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki).
Laboratory test and assessment of cirrhosis
A third-generation enzyme immunoassay kit (AxSYM® HCV Version 3.0; Abbott Laboratories, Abbott Park) was used for the anti-HCV test. A real-time PCR assay (COBAS® AmpliPrep Instrument and COBAS TaqMan® 48; Hoffmann-La Roche Ltd., Basel, Switzerland), with a detection limit of 15 IU/mL, was performed to quantify the serum HCV RNA. HCV genotyping was analyzed through a linear probe assay (VERSANT™ HCV Genotype Assay [LiPA]; Bayer AG, Leverkusen, Germany).
Liver biopsy samples were obtained from 387 patients with patient approval. Liver cirrhosis diagnosis was made by biopsy specimen with an Ishak modified histology activity index score ≥5, transient elastography (FibroScan; Echosens, Paris, France) according to the manufacturer's instructions, or FIB-4 > 3.25 (Sterling and others 2006) plus ultrasonography using the previously described cirrhosis scoring system (Lin and others 1993) with 80% sensitivity and 92.8% specificity.
Follow-up and HCC surveillance
After therapy, patients were observed from the end of the 24-week follow-up period to the date of HCC diagnosis, last-visit, or death. Liver ultrasonography and laboratory studies were routinely arranged every 3 or 6 months depending on patient cirrhosis status. If a routine study indicated HCC, further survey was arranged for confirmation. A diagnosis of HCC was confirmed on the basis of a histological assessment of a needle biopsy sample, surgically resected specimens, 2 image studies such as dynamic liver computed tomography or magnetic resonance imaging with typical arterial enhancement, or 1 image study plus an increased serum AFP level of more than 400 ng/mL (Bruix and Sherman 2005).
Statistical analysis
Continuous variables were expressed as mean ± standard deviation and tested for normal distribution using the Kolmogorov–Smirnov test. Normally distributed data were analyzed using the Student's t-test, other data using the Mann–Whitney U test, and categorical variables using the chi-square test, respectively. Clinical predictors associated with the risk of HCC development were identified using Cox proportional hazards regression model. Calibration was formed using the Hosmer–Lemeshow goodness-of-fit test to compare the number of observed and predicted events in risk groups for the entire range of HCC probabilities.
The study cohort was used to build the risk score model, and the validation cohort was used to test the model. Discrimination was analyzed using the area under receiver operating characteristic (AUROC) curve. A nonparametric approach was used to compare AUROC curves. AUROC curve analyses were also used to calculate cutoff values, sensitivity, specificity, and overall accuracy. Finally, cutoff points were calculated by acquiring the best Youden index (sensitivity + specificity −1). Cumulative incidence of HCC risk was analyzed using the Kaplan−Meier method and compared using the log-rank test. All statistical tests were 2 tailed, with P values <0.05 considered statistically significant. Data were analyzed using SPSS 12.0 software for Windows (SPSS, Inc., Chicago, IL).
Results
Patient characteristics
Baseline clinical and laboratory data of patients with and without HCC in both cohorts are presented in Table 1. The study cohort included 665 PR-treated patients with CHC, in which SVR was achieved at a rate of 67.5%. The median follow-up surveillance period was 5.4 years (range: 0.7–13.1 years). During the follow-up period, 65 (9.8%) patients in the study cohort developed post-treatment HCC. The annual incidence of post-treatment HCC development was 1.7 per 100 person-years (Table 2). The mean age of the patients at initiation of therapy was 54.0 ± 12.1 years, and 337 (50.7%) patients were men.
Baseline Demographic and Clinical Characteristics of Patients With Chronic Hepatitis C With and Without Hepatocellular Carcinoma
AFP, α-fetoprotein; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CHC, chronic hepatitis C; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; PegIFN, pegylated interferon; SD, standard deviation; SVR, sustained virological response.
Incidence Rate of Hepatocellular Carcinoma
CI, confidence interval.
Patients with post-treatment HCC who received antiviral therapy were significantly older; had higher body mass index, pretreatment serum aspartate aminotransferase, bilirubin, and AFP levels; and had lower pretreatment serum albumin levels and platelet counts. Among the patients that developed HCC, a high percentage of patients exhibited baseline cirrhosis and a low percentage of patients achieved SVR. The mean pretreatment alanine aminotransferase and HCV RNA levels and percentages of male patients and patients with HCV genotype 1b were similar in the patients with and without post-treatment HCC. Of the 600 patients without post-treatment HCC, 8 patients died of nonliver-related disease. During follow-up surveillance, 102 patients were censored for unknown reasons, and 66% of the patients were less than 60 years old.
Predictors of post-treatment HCC development
Several baseline clinical factors were identified through univariate Cox regression analysis as being significantly associated with post-treatment HCC development (Table 3): treatment age ≥60 years (hazard ratio [HR]: 3.39, 95% confidence interval [CI] = 2.06–5.59), pretreatment albumin (HR: 0.19, 95% CI = 0.11–0.35, P < 0.001), aspartate aminotransferase (HR: 1.0, 95% CI = 1.0–1.01), bilirubin ≥1.1 mg/dL (HR: 3.08, 95% CI = 1.74–5.45), platelet counts (HR: 0.98, 95% CI = 0.98–0.99), AFP ≥7.9 ng/mL (HR: 5.88, 95% CI = 3.12–11.08), non-SVR (HR: 3.54, 95% CI = 2.14–5.86), cirrhosis (HR: 9.86, 95% CI = 5.53–17.86), and fatty liver (HR: 0.25, 95% CI = 0.13–0.49). The significant factors were then entered into stepwise multiple regression analysis.
Analysis of Hepatocellular Carcinoma Predictors Using Univariate and Multivariate Cox Regression Models
HR, hazard ratio.
Multivariate Cox regression analysis results indicated that the following factors were significant predictors of post-treatment HCC development: treatment age ≥60 years (HR: 2.04, 95% CI = 1.3–3.7), pretreatment bilirubin ≥1.1 mg/dL (HR: 1.99, 95% CI = 1.08–3.67), AFP ≥7.9 ng/mL (HR: 2.44, 95% CI = 1.16–5.32), non-SVR (HR: 1.91, 95% CI = 1.05–3.45), and cirrhosis at baseline (HR: 4.45, 95% CI = 2.07–9.73).
Creation and validation of new scoring method for post-treatment HCC prediction
The 5 independent categorical predictors identified in the multivariate regression model were used to create a new scoring system for post-treatment HCC prediction according to the regression coefficient contribution of the predictors. We assigned 0 points for patients with a treatment age <60 years and 1 point for those ≥60 years; 0 points for pretreatment bilirubin <1.1 ng/mL and 1 point for bilirubin ≥1.1 ng/mL; for pretreatment AFP, 0 points for <7.9 ng/mL and 1 point for ≥7.9 ng/mL; 0 points for SVR and 1 point for non-SVR; and 0 points for no cirrhosis at baseline and 2 points for cirrhosis. The new score was the point sum of the 5 variables and ranged from 0 to 6.
The AUROC analysis yielded a new score of 0.884 with a cutoff point of 2.5 (P < 0.001; Fig. 1). Fifty-six and 444 patients with and without HCC, respectively, were identified correctly by the cutoff point value. The sensitivity, specificity, and overall accuracy of the cutoff point for detecting post-treatment HCC were 86.2%, 74.0%, and 75.2%, respectively. The positive and negative predictive values were 26.4% and 98.0%, respectively. Cumulative HCC incidence was significantly different (P < 0.001) for patients with HCC with new scores ≤2 (low risk) and new scores ≥3 (high risk; Fig. 2A). The 5- and 10-year cumulative incidence of post-treatment HCC development was 0.9% and 6.9%, respectively, in patients with low risk scores and 19.4% and 41.0%, respectively, in patients with high risk scores.
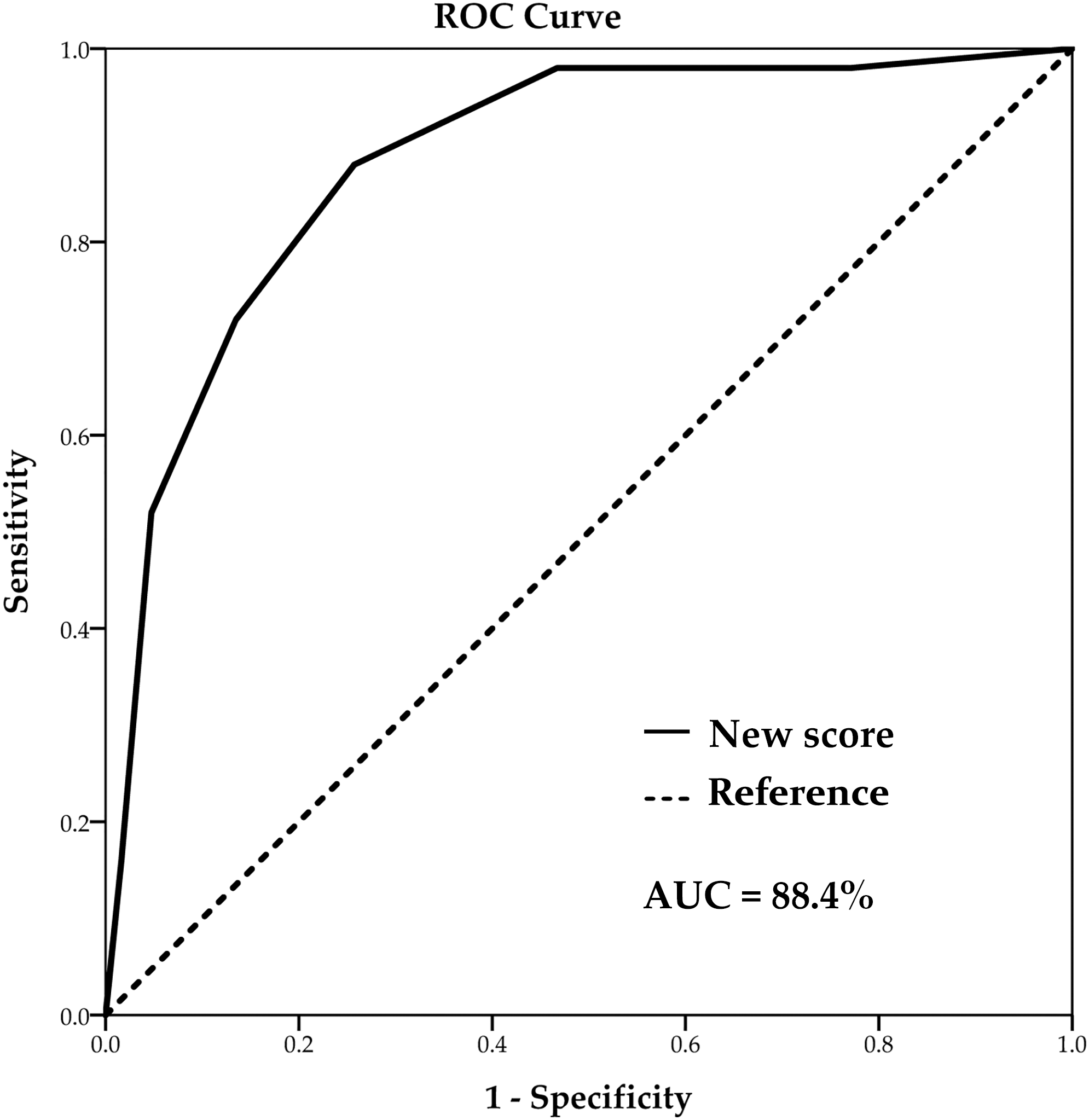
AUROC curve of the new scoring method for predicting the occurrence of HCC. A risk score higher than or equal to 2.5 had an AUROC of 0.884 ± 0.023 and predicted post-treatment HCC development with a sensitivity of 0.862 and specificity of 0.74. AUC, area under the curve; AUROC, area under receiver operating characteristic; HCC, hepatocellular carcinoma.
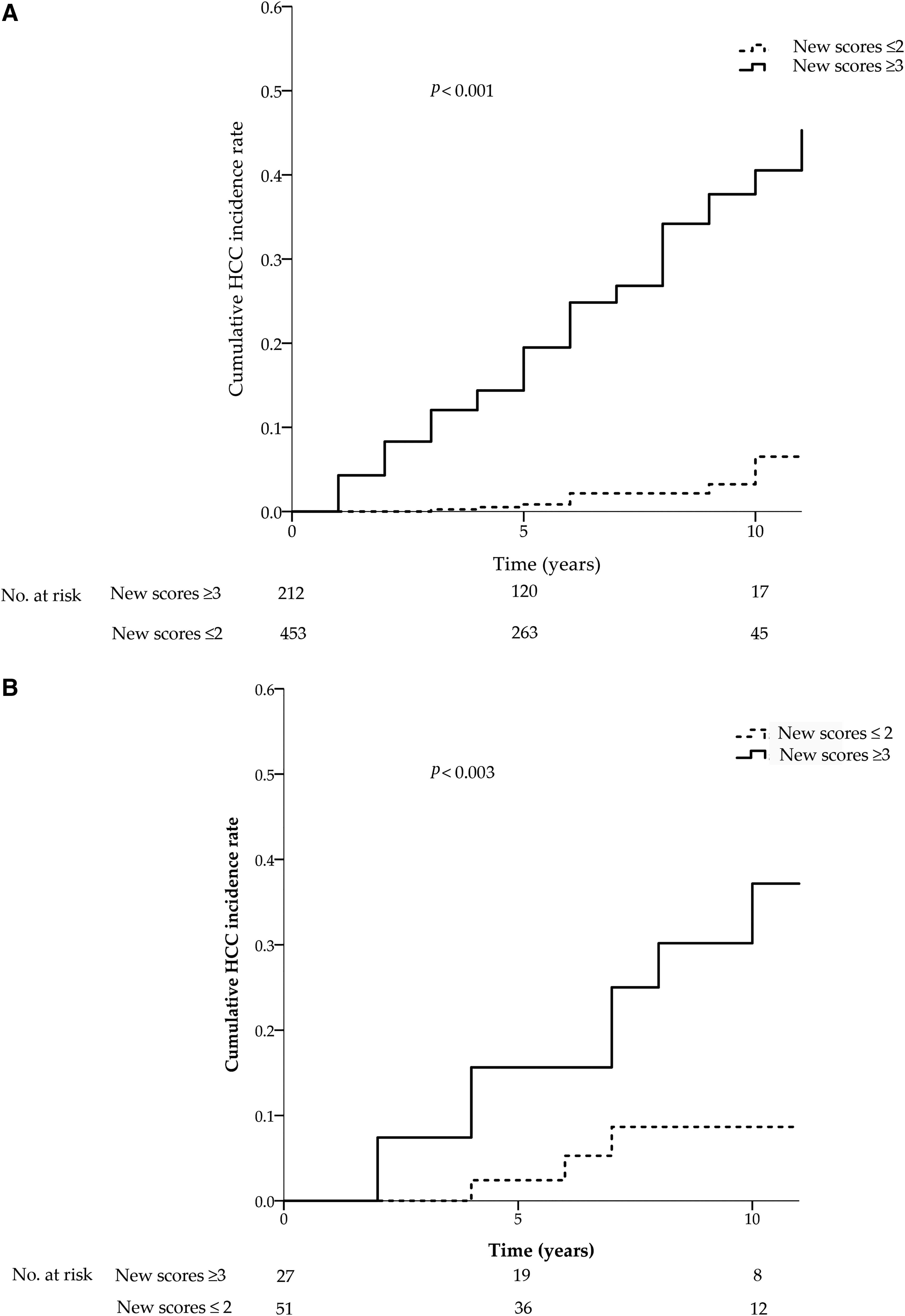
Cumulative incidence of HCC of the
In the validation cohort, 13 of 78 (16.7%) patients developed HCC during the follow-up period. Using the cutoff point of 2.5, 10 and 48 patients with and without HCC were properly identified. The sensitivity, specificity, positive predictive value, and negative predictive value were 76.9%, 73.8%, 37.0%, and 94.1%, respectively. The discrimination of cumulative HCC incidence was significantly different for the high and low risk score patients (P = 0.003; Fig. 2B). The 5- and 10-year cumulative incidence of post-treatment HCC was 2.5% and 8.3%, respectively, in patients with low risk scores and 15.5% and 36.2%, respectively, in patients with high risk scores.
Among the 449 patients who achieved SVR after PR therapy, 98 (21.8%) patients had new scores ≥3, and 351 (78.2%) patients had new scores ≤2. During the follow-up period, 24 patients developed post-treatment HCC, with 18 patients having new scores ≥3 and the remaining 6 patients having new scores ≤2. The incidence rates of HCC per 100 person-years were significantly higher in SVR patients with high risk scores (3.31, 95% CI = 2.02–5.13), compared to SVR patients with low risk scores (0.29, 95% CI = 0.12–0.61), P < 0.001 (Table 2).
The Kaplan–Meier curve analysis showed that the cumulative HCC incidence was also significantly higher in the patients with SVR and high risk scores than the patients with SVR and low risk scores (P < 0.001; Fig. 3A). Among the sustained responders, the 5- and 10-year cumulative incidence of post-treatment HCC development was 1.2% and 4.2%, respectively, in patients with low risk scores and 16.7% and 30.4%, respectively, in patients with high risk scores.
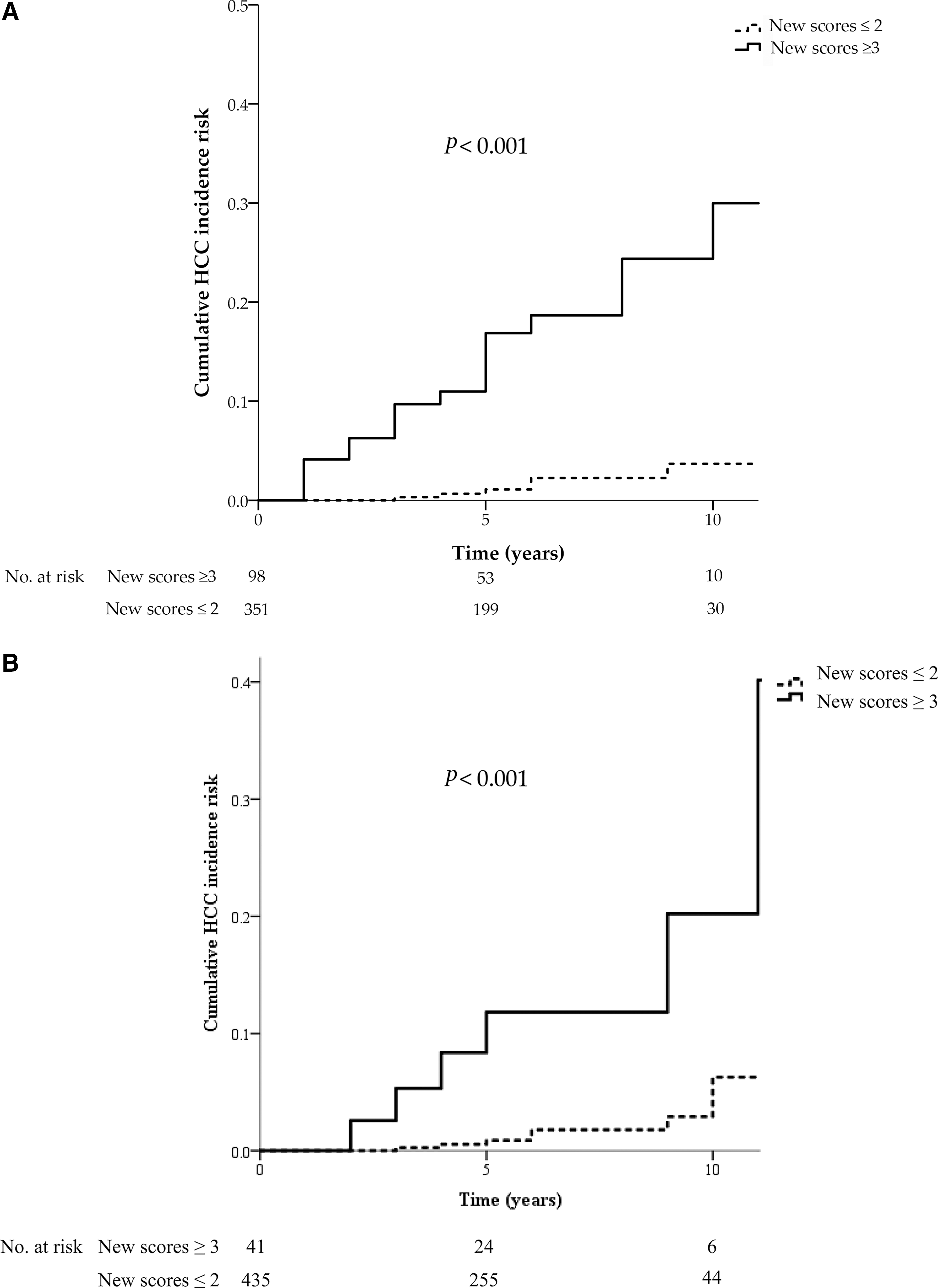
Cumulative incidence rate of HCC of CHC patients
Finally, among the 476 patients without baseline cirrhosis, 41 (8.6%) patients had new scores ≥3, and 435 (91.4%) patients had new scores ≤2. Fourteen patients developed HCC during post-treatment surveillance, with 6 patients having new scores ≥3 and the other 8 patients having new scores ≤2. The incidence rates of HCC per 100 person-years were significantly higher in noncirrhotic patients with high risk scores (2.46, 95% CI = 1.0–5.13), compared to noncirrhotic patients with low risk scores (0.31, 95% CI = 0.14–0.59), P < 0.001.
The Kaplan–Meier curve analysis showed that the cumulative HCC incidence was also significantly higher in the noncirrhotic patients with high risk scores than those with low risk scores (P < 0.001; Fig. 3B). The 5- and 10-year cumulative incidence of HCC development after PR therapy was 0.9% and 6.6%, respectively, in the noncirrhotic patients with low risk scores and 11.9% and 21.7%, respectively, in the noncirrhotic patients with high risk scores.
Discussion
This study developed a simple new scoring method using commonly available clinical parameters to predict the risk of post-treatment HCC in patients previously with CHC and without HCC after PR therapy. Chang and others (2013) also developed a scoring system to predict HCC in patients with CHC after an IFN-based therapy using 7 different factors, including age, sex, platelet count, AFP, fibrosis stage, HCV genotype, and SVR. However, the AUROC of the scoring system was 0.794, which was lower than our AUROC of 0.884. In addition, our new method includes only 5 clinical factors and is simpler to use in a clinical setting.
With a new score ≥3, patients have significantly higher risk for post-treatment HCC than patients with lower scores. The cumulative incidence of HCC at 10 years was 41.0%. By contrast, 6.9% of the patients with a new score ≤2 developed HCC at 10 years after therapy. Surveillance schedules for patients with CHC who have received antiviral therapy should be arranged according to whether their score reveals high or low risk.
Aging had been associated with a high risk of HCC (Bruno and others 2007a; Asahina and others 2010; Chang and others 2012; Alavi and others 2018). Asahina and others (2010) demonstrated that the risk for HCC development after an IFN therapy was age dependent. The HCC risk depended on the age at liver biopsy and increased significantly (>15 fold) after 65 years. Bruno and others (2007a) proved that a higher risk for HCC development manifested at age 60 or higher. This study also determined that an age of 60 years or higher is a predictor for post-treatment HCC, with an AUROC of 0.661 (P < 0.001).
Previous studies have shown that mild elevation of serum bilirubin levels is significantly associated with HCC occurrence (Degos and others 2000; Fattovich and others 2004). Moreover, we identified that serum bilirubin greater than 1.1 mg/dL could predict post-treatment HCC, with an AUROC of 0.648 (P = 0.001).
Baseline liver cirrhosis was reported to be a significant risk factor for post-treatment HCC occurrence in patients with CHC treated with an IFN-based therapy or DAAs (Conti and others 2016; Nagaoki and others 2016). Our study also demonstrated that pretreatment cirrhosis strongly predicted HCC occurrence after PR therapy. However, the sensitivity and specificity levels of pretreatment cirrhosis used to predict post-treatment HCC were 76.9% and 78.3%, respectively, with an AUROC of 0.77 (P < 0.001). The AUROCs of these single predictors were lower compared with the new scoring method with a cutoff point of 2.5.
In this study, 14 (2.9%) of 476 patients without baseline cirrhosis developed post-treatment HCC. According to the new scoring method, 9.4% of the noncirrhotic CHC patients had high risk scores. The noncirrhotic patients with high risk scores had significantly higher risk for post-treatment HCC development than those with low risk scores. It represented that SVR patients without cirrhosis with age over 60 years, serum bilirubin greater than 1.1 mg/dL, and AFP greater than 7.9 ng/mL should be intensively scheduled for post-treatment HCC surveillance.
Studies have demonstrated that an elevated level of serum AFP significantly predicts HCC development; therefore, it has commonly been used for HCC surveillance (Ikeda and others 1993; Tsukuma and others 1993). However, an elevated AFP level may only represent increased proliferative activity of hepatocyte during hepatic inflammation and regeneration in patients with acute liver injury, chronic hepatitis, and advanced CHC without evidence of HCC (Bloomer and others 1975; Taketa 1990; Chu and others 2001; Hu and others 2004; Di Bisceglie and others 2005). In addition, the sensitivity level of AFP for HCC detection was also low, with a serum cutoff point of 20 ng/mL (Paul and others 2007).
Asahina and others (2013) indicated that post-treatment serum AFP level >6 ng/mL predicted post-treatment HCC after an IFN-based therapy with an AUROC of 0.816. In our study, we showed that pretreatment AFP ≥7.9 ng/mL predicted post-treatment HCC development with an AUROC of 0.761 (P < 0.001). Both AUROCs were lower compared with the new scoring method developed in this study to predict post-treatment HCC.
SVR has reduced the HCC incidence in patients with CHC after an IFN-based therapy (Bruno and others 2007b; Kanogawa and others 2015; Shirabe and others 2015; Tada and others 2016). Our study attained comparable results. The sensitivity and specificity levels of non-SVR for post-treatment HCC prediction were 70.8% and 63.1%, respectively, with an AUROC of 0.67 (P < 0.001)—lower than the new scoring method. Therefore, a new score ≥3 provides a stronger parameter for post-treatment HCC prediction.
Although few patients fail antiviral therapy in the era of DAAs, the risk of post-treatment HCC occurrence is not entirely eliminated in these patients after viral eradication. In this study, 24 of 449 patients with SVR developed post-treatment HCC. According to our new scoring method, 21.8% of the SVR patients possessed high risk scores. The SVR patients with high risk scores had a significantly higher post-treatment HCC risk than those with low risk scores and represented a subset of the cirrhotic patients with age ≥60 years, AFP ≥7.9 ng/mL, or bilirubin ≥1.1 mg/dL, as well as patients without cirrhosis with all 3 criteria; therefore, these patients should be closely monitored for HCC occurrence.
The HCV genotype 1b was reportedly associated with an increased risk of HCC in patients who failed therapy or remained untreated (Bruno and others 2007a). However, in our study no significantly higher HCC risk was evident in patients with the HCV genotype 1b compared with a non-1b genotype after PR therapy. Likewise, although studies have demonstrated that male patients possessed a greater risk for HCC, we detected no significant differences in HCC risk between sexes (Khan and others 2000; Fattovich and others 2004; Asahina and others 2010).
Nonetheless, studies have suggested that the HCC risk is reduced when the anticarcinogenic effects of IFNs enable cell cycle arrest and apoptosis of cancer cells (Maeda and others 2014). However, our study ascertained that a longer duration of pegylated IFN therapy was not associated with a reduced risk of HCC. Furthermore, Chang and others (2015) demonstrated that IL-28B rs12979860 non-CC genotype was a predictor for HCC. The possible role of IL-28B in current patients is being analyzed.
In conclusion, we developed a new scoring method with good discriminatory ability for post-treatment HCC prediction in this study. With DAAs, most patients experience successful eradication of HCV infections after antiviral therapy. However, in the new scoring system, the score values exceeded a benchmark level of 3 in SVR patients with cirrhosis and age over 60 years, pretreatment AFP ≥7.9 ng/mL, or bilirubin ≥1.1 ng/mL and in SVR patients without cirrhosis and with all 3 criteria. These patients exhibit a high risk for post-treatment HCC and warrant intensive surveillance after successful viral eradication.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by the Chang Gung Memorial Hospital Research Grant CGRPG2F0071.