
Abstract
The coronavirus disease 2019 (COVID-19) pandemic has affected the entire world, and has a variety of clinical presentations. The aim of this study is to determine the relationships of fecal cytokines and markers with the symptoms and prognosis of children with COVID-19 infection, and to identify noninvasive markers during follow-up. In a cohort of 40 COVID-19-positive children and 40 healthy controls, fecal cytokines and markers were examined in stool samples. A binary logistic model was used to assess the potential of cytokines as risk factors for hospitalization. Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. A P-value <0.05 was accepted as statistically significant. Levels of fecal lysozyme, myeloperoxidase, hemoglobin, and interleukin-5 (IL-5) (P < 0.05) were significantly higher among the patients than controls. In a logistic regression analysis, fecal IL-2 (OR = 3.83; 95% CI: 1.44–15.92), IL-4 (OR = 2.96; 95% CI: 1.09–12.93), IL-5 (OR = 4.56; 95% CI: 1.18–27.88), IL-10 (OR = 2.71 95% CI: 1.19–7.94), interferon-gamma (IFN-γ) (OR = 4.03; 95% CI: 1.44–15.73), IFN-α (OR = 3.02; 95% CI: 1.08–11.65), calcium-binding protein B S100 (S100 B) (OR = 4.78; 95% CI: 1.31–27.82), neutrophil elastase (NE) 2 (OR = 4.07; 95% CI: 1.17–19.69), and matrix metalloproteinase 1 (MMP-1) (OR = 3.67; 95% CI: 1.1–18.82) levels were significantly higher in hospitalized patients with COVID-19 infection than outpatients. We demonstrated that various fecal cytokines and markers were increased in patients who had COVID-19. Fecal IL-2, IL-4, IL-5, IL-10, IFN-γ, IFN-α, S100 B, NE, and MMP-1 levels were significantly elevated in hospitalized patients. We suggest that the fecal and serum levels of cytokines could be used to predict the prognosis of COVID-19 disease, although more studies are needed to confirm this.
Introduction
Severe acute respiratory syndrome coronavirus 2
In children, the clinical manifestations of the disease range from mild respiratory tract infection to severe lung injury, multiple organ failure, and death caused by hyperinflammation and cytokine storm syndrome (Lamers et al, 2020; Neurath, 2020). Diarrhea, vomiting, and abdominal pain are also common gastrointestinal (GI) symptoms that may occur in isolation or together with respiratory symptoms (Tian et al, 2020).
The most important defense mechanism against viral infection is natural immunity. Antiviral cytokines produced by lymphocytes and epithelial cells are induced, and their levels elevated, in various viral infections.
Measuring levels of fecal cytokines and markers is a sensitive and noninvasive method for monitoring intestinal immune responses during inflammatory disease and enteric infection. In particular, the fecal levels of interleukin-2 (IL-2), interferon-gamma (IFN-γ), IL-6, IL-8, and IL-1β are increased in acute bacterial and viral gastroenteritis and ulcerative colitis (Brittion et al, 2021). Fecal IL-23 was elevated in adult patients with severe COVID-19 disease (Britton et al, 2021).
On the contrary, various studies have shown that COVID-19 infection negatively affects the microbiota (Yeoh et al, 2021; Zuo et al, 2020). While there is a dramatic decrease in gut bacteria known as immunomodulatory potential such as Faecalibacterium prausnitzii, Roseburia, and Lachnospiraceae of patients with COVID-19 infection, it has been shown that there is a significant increase in gut bacteria that cause proinflammation such as Clostridium hathewayi, Actinomyces viscosus, and Bacteroides nordii (Zuo et al, 2020).
The study of Yeoh et al. (Yeoh et al, 2021) proposed that the severity of COVID-19 infection was associated with the increasing dysbiosis index. In the same study, there was a correlation between increased dysbiosis and high levels of proinflammatory cytokines and inflammatory markers. The alteration of gut microbiota also influences the permeability of the gut barrier (Konturek, 2021). As a result, it was stated that intestinal dysbiosis may support the cytokine storm (Yeoh et al, 2021).
Therefore, the aim of this study was to determine the relationships of fecal cytokines and markers with COVID-19 symptoms and prognosis in children, and to identify noninvasive markers during follow-up.
Materials and Methods
Patient recruitment and clinical data collection
This cross-sectional study included 40 pediatric patients who had been diagnosed with SARS-CoV-2; RT-PCR was used for diagnosis. The study was performed at Istanbul University-Cerrahpasa, Cerrahpasa Faculty of Medicine, Department of Pediatric Gastroenterology, Hepatology, and Nutrition, in Istanbul, Turkey, from November 1, 2020, to February 1, 2021.
Stool samples were collected twice from the study group. The first samples were collected at the time of diagnosis (within 3 days) and the second samples 3 weeks after diagnosis. These samples were stored at −80°C until the study was carried out. Patients who provided their first stool samples after the third day and those who could not provide second samples were excluded from the study.
The demographic and clinical features of the cases were recorded. Patients were grouped according to whether they received outpatient or hospital care.
Patients who had no complaints but were shown to be positive for COVID-19 by PCR after coming into contact with a family member with COVID-19 were classified as asymptomatic.
Patients who could be followed at home, had no evidence of pneumonia on chest X-ray (CXR), or had peripheral oxygen saturation (SpO2) of at least 94% were considered to be outpatients. Patients who had pneumonia findings on CXR, SpO2 below 94%, a requirement for respiratory or vasopressor support, creatinine clearance <30 mL/min, alanine amino transferase >5-fold the baseline, or end organ damage, and who were followed in the hospital, were classified as hospitalized patients (Dong et al, 2020).
The control group included 40 healthy children; stool samples from these children were kept at −80°C under suitable conditions until the study was carried out. The control group patients were aged 0–18 years, and had no history of infection or evidence thereof in physical examinations, as well as no history of contact with individuals with COVID-19 or travel in the previous 15 days, and negative oropharyngeal/nasopharyngeal SARS-CoV-2 RT-PCR tests.
Children in the patient and control groups who agreed to participate, and whose parents signed the informed consent forms, were included in the study. IL-2, IL-4, IL-5, IL-10, tumor necrosis factor-alpha (TNF-α), IFN-α, IFN-γ), calprotectin, lactoferrin, calcium-binding protein S100 (S100 B), pyruvate kinase, lysozyme, neutrophil elastase (NE) 2, neopterin, matrix metalloproteinase-1 (MMP-1), hemoglobin, and myeloperoxidase levels were measured in the first and second stool samples of the study group patients and controls. These data were then compared between the 2 groups. In addition, clinical findings of the patients in the severe disease group were obtained after 3 months.
Fecal sample collection and processing
Fecal samples were collected into sterile containers (Precision™ Stool Collector; Covidien, Dublin, Ireland) and frozen at −80°C for measurement of cytokines. The samples were thawed on ice. Approximately 1 g of each fecal specimen was added into an extraction buffer tube (containing protease inhibitor) and shaken to make the mixture homogeneous. The contents were centrifuged at 12,000x g for 20 min at 4°C, and the supernatants were then collected for measurement of fecal cytokines, calprotectin, and other markers.
Measurement of fecal cytokines, calprotectin, and other markers
IL-2, IL-4, IL-5, IL-10, TNF-α, IFN-α, IFN-γ, calprotectin, lactoferrin, CBPS100, pyruvate kinase, lysozyme, NE 2, neopterin, MMP-1, and hemoglobin were measured with Elabscience (Wuhan, China) enzyme-linked immunoassay (ELISA) kits, and myeloperoxidase was measured with a BT Lab Systems' (St. Louis, MO) ELISA kit. Dilution was performed according to the manufacturer's instructions.
Statistics
The data obtained from the patient and control groups were analyzed using SPSS software (version 26.0; SPSS, Inc., Chicago, IL). The Kolmogorov-Smirnov test was used to examine the normality of the data. Numerical data are summarized as mean ± standard deviation or median (minimum–maximum) depending on the distribution. Frequencies and percentages were calculated for categorical data. Student's t-test or the Mann–Whitney U test was used for comparison of patients and healthy controls. One-way analysis of variance (ANOVA) followed by Dunnett's multiple comparison test, or the Kruskal-Wallis test followed by Dunn's multiple comparison test, were used to compare the study and control groups.
First and second samples were compared using the paired Student's t-test or Wilcoxon signed rank test. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated using univariate binary logistic regression models to assess the potential of cytokines as risk factors for hospitalization. The predictors were natural log-transformed for the regression models, to prevent the regression coefficients being close to zero. Due to multicollinearity and strong correlations between cytokines, a multiple logistic regression model could not be fitted. A P-value <0.05 was accepted as statistically significant.
Results
Twenty (50%) of the patients were male, and 20 (50%) were female. The mean age of the 40 patients was 8.52 ± 5.77 years, and the mean ages of the boys and girls were 8.85 ± 5.65 and 8.20 ± 6.03 years, respectively. Among the children in the control group, 18 (45%) were male and 22 (55%) were female. Their mean age was 7.45 ± 4.66 years, and the mean ages of the boys and girls were 7.68 ± 5.12 and 7.24 ± 5.58 years, respectively. There was no significant difference in gender or age between the study and control groups (P > 0.05).
In the study group, 11 (27.5%) patients had no symptoms, while 15 (37.5%) had coughing, 21 (52.5%) had a fever, 8 (20%) experienced abdominal pain, 5 (12.5%) had vomiting, 7 (17.5%) had diarrhea, and 1 had lower GI bleeding. The patients' medical history and clinical symptoms are shown in Fig. 1.

Underlying disease and symptoms of study population.
No significant differences were found between the fecal cytokines and markers between the first and second stool samples (P > 0.05) (Fig. 2). The first fecal samples of the patients and controls were also compared. The study group had significantly higher levels of IL-5, lysozyme, myeloperoxidase, and hemoglobin (P = 0.02, P < 0.001, P = 0.006, and P < 0.001, respectively). However, the levels of TNF alpha, IFN gamma, lactoferrin, NE 2, and CBPS100 were significantly lower in the study group (P = 0.002, P < 0.001, P = 0.006, P < 0.001, and P = 0.008, respectively) (Table 1).
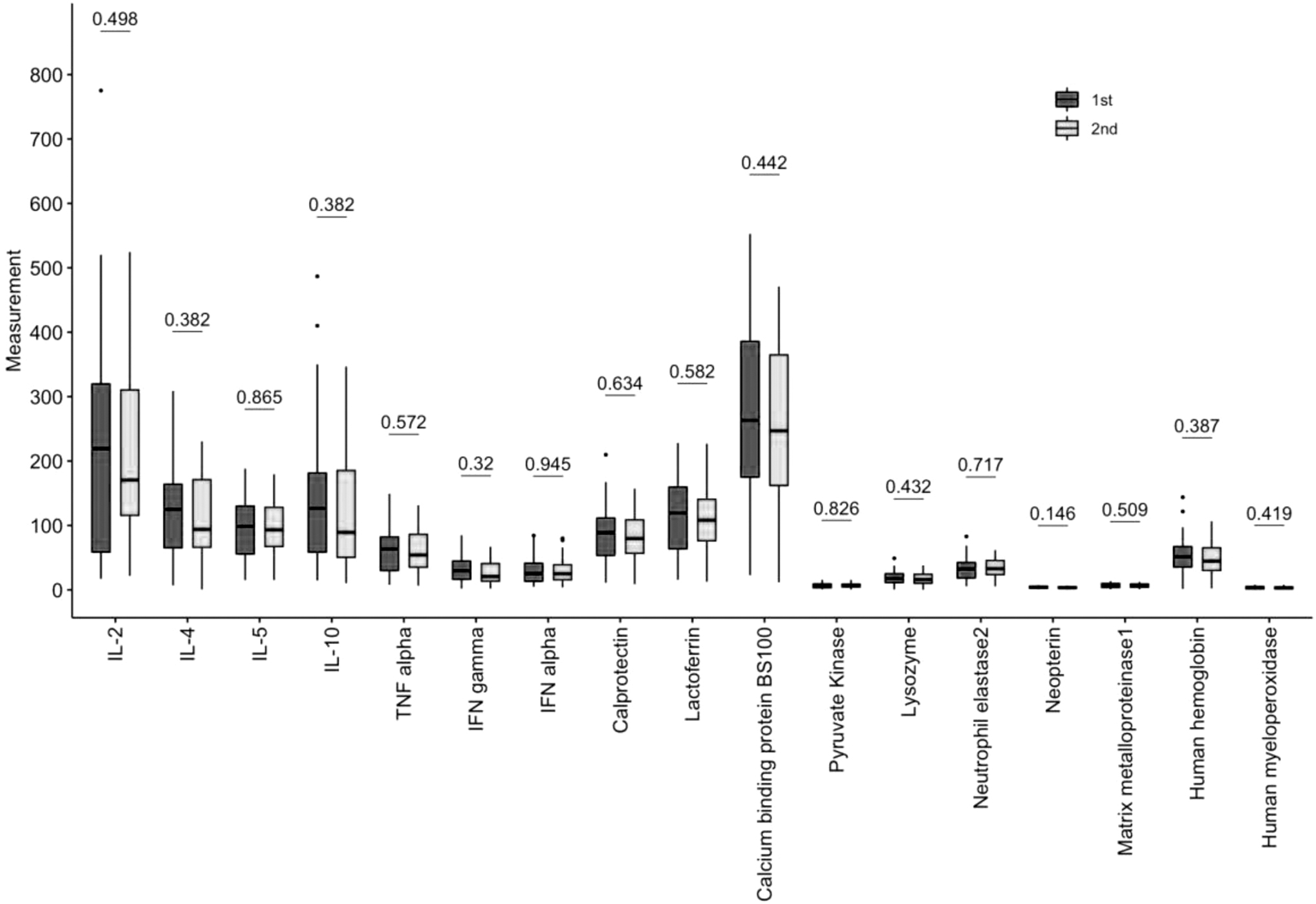
Boxplots for 1st and 2nd samples of cytokines of patients. P values were shown on top of boxplots. Boxes represent the 25th–75th percentile of each variable. The horizontal line in each box represents the median. The whiskers represent the local maximum and local minimum values. Values that are >1.5 times the interquartile range from either end of the box are considered outliers and denoted with a small dot (1st samples taken in the first 3 days of patients diagnosed with COVID-19 infection, 2th samples of the same patients 3 weeks later). COVID-19, coronavirus disease 2019; IFN, interferon; IL, interleukin; TNF, tumor necrosis factor.
Comparison of Fecal Cytokines and Markers with Samples of Patient and Healthy Controls
Statistically significant results are mentioned in bold.
1st samples taken in the first 3 days of patients diagnosed with COVID-19 infection.
IFN, interferon; IL, interleukin; S100 B, calcium binding protein B S100; SD, standard deviation; TNF, tumor necrosis factor.
The fecal cytokines and markers of the children in the study group were analyzed according to the presence of symptoms (Table 2); these markers were also compared between the hospitalized and outpatient patients with COVID-19. The fecal IL-2, IL-4, IL-5, IL-10, TNF alpha, IFN gamma, IFN alpha, lactoferrin, S100 B, pyruvate kinase, lysozyme, NE 2, neopterin, MMP-1, hemoglobin, and myeloperoxidase levels were significantly higher among hospitalized patients (Table 3). The results of the assessment of cytokines as potential predictors of clinical prognosis are shown in Table 4. In the logistic regression analysis, IL-2 (OR = 3.83; 95% CI: 1.44–15.92), IL-4 (OR = 2.96; 95% CI: 1.09–12.93), IL-5 (OR = 4.56; 95% CI: 1.18–27.88), IL-10 (OR = 2.71; 95% CI: 1.19–7.94), IFN-γ (OR = 4.03; 95% CI: 1.44–15.73), IFN-α (OR = 3.02; 95% CI: 1.08–11.65), S100 B (OR = 4.78; 95% CI: 1.31–27.82), NE 2 (OR = 4.07; 95% CI: 1.17–19.69), and MMP-1 (OR = 3.67; 95% CI: 1.1–18.82) levels were significantly higher in hospitalized patients with COVID-19 infection than outpatients (Table 4).
Comparison of Symptoms and Fecal Cytokines and Marker
Statistically significant results are mentioned in bold.
The given P-values are given by comparing the symptoms with the control group.
GI, gastrointestinal.
Relationship of Fecal Cytokines and Markers with Disease Severity
Statistically significant results are mentioned in bold.
The P-values given are given by comparing the outpatient and hospitalized groups of patients.
Univariate Logistic Regression of Cytokines as Potential Risk Factors on Hospitalization
Statistically significant results are mentioned in bold.
Log transformed values of predictors were used in the models.
95% CI, confidence interval of OR; OR, odds ratio from univariate logistic regression model where the output is hospitalization.
Discussion
Accumulating data on the COVID-19 pandemic have revealed that GI symptoms are very common in infected patients (Pan et al, 2020). SARS-CoV-2 can actively infect and proliferate in the GI tract, especially the ACE2 receptor-rich part of the lower digestive system (Wong et al, 2020). In a study, 28.3% of pediatric patients had GI symptoms, 22% had diarrhea, 9.4% had vomiting, and 6.3% had abdominal pain. Moreover, the presence of GI symptoms was associated with a severe phenotype (Giacomet et al, 2020). In our study, 27.5% of the 40 pediatric patients were asymptomatic, while 37.5% presented with cough, 52.5% with fever, 20% with abdominal pain, 12.5% with vomiting, and 17.5% with diarrhea. One patient presented with lower GI bleeding.
In a retrospective study of 2,141 pediatric patients (median age = 7 years) who had COVID-19, 43.1% had mild disease, 41.0% had moderate disease, 2.5% had severe disease, and 0.6% had critical disease (Dong et al, 2020). In our study, mild disease was observed in 67.5% of the patients, while the 23.5% who were followed up in the hospital had moderate-to-severe disease.
Many cytokines are elevated in the serum of most COVID-19 patients (Rothan and Byrareddy, 2020). Various fecal cytokines contribute to the integrity and function of the GI system (Bamias et al, 2015). A previous study of adult patients with COVID-19 found that their fecal IL-8 levels were significantly increased, while the IL-10 levels were lower than those of uninfected individuals (Britton et al, 2021). Similar to a study by Britton et al (Britton et al, 2021), fecal IL-10 levels were low in our patients who presented with cough.
Fecal calprotectin is a cytosolic protein with immunomodulatory, antimicrobial, and antiproliferative effects. Effenberger et al (2020) found high fecal calprotectin levels in COVID-19 patients; they stated that an inflammatory response was triggered in the intestines. In our study, increased calprotectin was observed only in patients who had vomiting. The lack of elevation of these markers in other patients presenting with GI symptoms may be related to the small number of such patients.
Several other studies have reported a relationship between fecal neopterin, which is an important marker of intestinal inflammation, and COVID-19 infection (Grabherr et al, 2021). In our study, no group differences were found in neopterin levels.
CBPS100 is secreted from monocytes, macrophages, and inflammatory cytokines in a state of inflammation, and especially in those with infection. Fecal CBPS100 is decreased in inflammatory bowel diseases (Di Liddo et al, 2020). In our study, a decrease in CBPS100 was particularly evident in febrile and COVID-infected patients. This is another indication that COVID-19 infection affects the intestinal immune system.
Fecal lysozyme, myeloperoxidase, and hemoglobin are useful markers of intestinal inflammation (Hansberry et al, 2017; Mooiweer et al, 2014; Veer et al, 1998). In our study, the levels of lysozyme, myeloperoxidase, and hemoglobin were significantly higher in patients with COVID-19 than healthy controls. These findings are another indication that COVID-19 infection significantly affects the intestinal immune system. The lack of significant differences in fecal cytokines and markers among the patients' samples suggests that the GI immune response did not decrease over a period of 3 weeks. In particular, increases in IL-2, IL-4, IL-5, IL-10, IFN-γ, IFN-α, S100 B, NE 2, and MMP-1 predict hospitalization in COVID-infected children.
Britton et al (2021) in the study, higher fecal SARS-CoV2 mRNA was detected in stool samples of patients who died from COVID-19 infection compared to those who did not. This situation suggested that it induces an irregular immune response through the intestines and causes mortality (Britton et al, 2021). In our study, we were evaluated fecal cytokines and markers. We found high levels of IL-2, IL-4, IL-5, IL-10, IFN-γ, IFN-α, S100 B, NE, and MMP-1 in hospitalized patients' fecal samples. However, we could not have chance to study Sars-CoV2 mRNA in the stools of the study groups. It was the limitation of our study.
The limitations of our study included the lack of simultaneous measurement of fecal cytokines and serum cytokines, and the small number of patients included. As a result, we were not able to evaluate the correlation of fecal cytokine levels with the systemic cytokine responses. Also, the presence of COVID-19 could not be investigated in fecal swabs by PCR.
Conclusions
COVID-19 infection is associated with changes in fecal cytokine and marker levels in children. The levels of fecal cytokines and markers vary according to the presence of symptoms. Hemoglobin, myeloperoxidase, and lysozyme were generally high in the children with symptomatic COVID-19 infection in this study. It is not clear why COVID-19 is mild in some patients and severe in others. In particular, increases in IL-2, IL-4, IL-5, IL-10, IFN-γ, IFN-α, S100 B, NE 2, and MMP-1 are major risk factors for hospitalization in COVID-infected children. We showed that the gut is an immunologically active organ in COVID-19 infection. Larger studies of fecal and serum cytokines are needed to improve the management of the dysregulated cytokine response seen in COVID-19 infection.
The English in this document has been checked by at least 2 professional editors, both native speakers of English. For a certificate, please see:
Footnotes
Acknowledgment
The authors thank Istanbul-Cerrahpasa University Scientific Research Projects.
Authors' Contributions
A.D.T., G.U., G.M., and M.K. contributed to the design and implementation of the research; A.D.T. and E.A. to the analysis of the results and to the writing of the article. A.D.T., P.Ö., A.D.P., M.K., K.M., A.A.K., H.Ç., Ö.F.B., and F.Ç.Ç. conceived the original and supervised the project.
Consent to Participate
Written informed consent to participate in the study was obtained from the patients' guardian.
Ethical Approval
The study was approved by the Institutional Ethics Committee.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Istanbul-Cerrahpasa University Scientific Research Projects TSG-2020-34992.