
Abstract
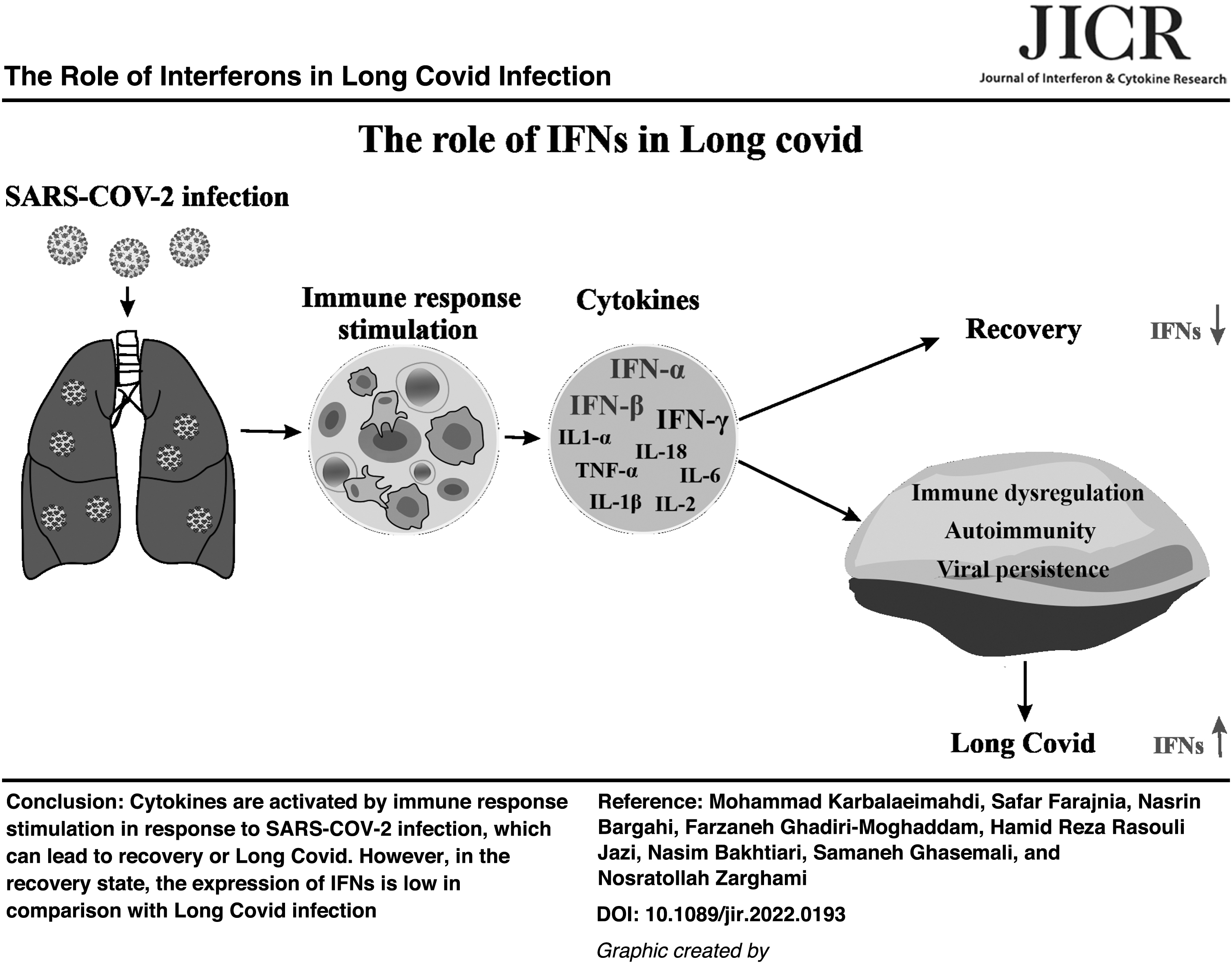
Although the new generation of vaccines and anti-COVID-19 treatment regimens facilitated the management of acute COVID-19 infections, concerns about post-COVID-19 syndrome or Long Covid are rising. This issue can increase the incidence and morbidity of diseases such as diabetes, and cardiovascular, and lung infections, especially among patients suffering from neurodegenerative disease, cardiac arrhythmias, and ischemia. There are numerous risk factors that cause COVID-19 patients to experience post-COVID-19 syndrome. Three potential causes attributed to this disorder include immune dysregulation, viral persistence, and autoimmunity. Interferons (IFNs) are crucial in all aspects of post-COVID-19 syndrome etiology. In this review, we discuss the critical and double-edged role of IFNs in post-COVID-19 syndrome and how innovative biomedical approaches that target IFNs can reduce the occurrence of Long Covid infection.
Introduction
Postinfectious disorders beyond COVID-19
At the beginning of the coronavirus outbreak, research mainly focused on early-stage symptoms of COVID-19 and its effects on mortality. However, over time, the importance of studying the long-term effects of this disease became more apparent. Long Covid, also known as post-COVID, post-COVID condition (PCC), postacute sequelae SARS-CoV-2 infection (PASC), chronic COVID syndrome, and acute COVID-2, refers to the long-term effects of COVID-19 (Nittas et al, 2022). According to the World Health Organization, it is a condition that usually occurs 3 months after COVID-19 infection with symptoms, lasts for no <2 months, and other causes cannot explain (World Health Organization, 2021). The U.S. Centers for Disease Control and Prevention (CDC) believes that PCC identification would be at least 4 weeks after the infection (Centers for Disease Control and Prevention, 2022).
The National Institute for Health and Care Excellence of United Kingdom distinguishes between a post-COVID-19 syndrome lasting longer than 12 weeks and an ongoing symptomatic COVID-19 duration of 4–12 weeks (National Institute for Health and Care Excellence, 2021). The phrase “Long Covid” is often employed to define signs and indications that occur or develop following an acute COVID-19. It covers both the post-COVID-19 syndrome (12 weeks or longer) and ongoing symptomatic COVID-19 (from 4 to 12 weeks). The extent of this condition is unclear and can lead to numerous health problems in affected patients, including psychological and physical symptoms that interfere with daily activities. Higher Age, high index of body mass, and female sex may increase the probability (Sudre et al, 2021). Long after the acute phase of COVID-19, a significant number of individuals report persistent symptoms.
According to the Office for National Statistics of United Kingdom (ONS), as of May 1, 2022, ∼2.0 million persons (3.1% of the total population) in the United Kingdom were suffering from self-reported Long Covid (Office for National Statistics, 2020). ONS estimates that about 1/5th of respondents who test positive for COVID-19 show symptoms for 5 weeks or longer, and about 1/10th of respondents who test positive for COVID-19 show symptoms over 12 weeks or longer (Office for National Statistics, 2022). It has been reported that 4 months after initial COVID-19 symptoms, 70% of those at low risk of COVID-19 death with persistent indications experienced damage in some organs (Dennis et al, 2021).
Common signs and symptoms of Long Covid
People with Long Covid experience various symptoms affecting multiple organs, including the cardiovascular system, respiratory system, kidneys, liver, pancreas, spleen, skin, neurological system, and digestive system (Bourmistrova et al, 2022; Dennis et al, 2021; Genovese et al, 2021; Liao et al, 2022; Nalbandian et al, 2021; Nguyen and Tosti, 2022). It is also linked to a higher risk of developing new health conditions such as incident diabetes in men, neurological problems, and autoimmune diseases (Acosta-Ampudia et al, 2022; Bourmistrova et al, 2022; Rojas et al, 2022; Wander et al, 2022). Also, people with Long Covid may have an elevated risk of developing cerebrovascular disorders like cardiac arrhythmias, ischemic and nonischemic heart disease, pericarditis, myocarditis, heart failure, and thromboembolic disease (Xie et al, 2022).
Some of the prevalent reported symptoms with Long Covid are fatigue, headache, upper respiratory symptoms (dyspnea, sore throat, persistent cough, and altered sense of smell or taste), gastroenterological symptoms (diarrhea, nausea, acid reflux, stomach pain, and loss of appetite), chest pain or tightness, cognitive and psychological complaints (post-traumatic stress disorder, brain fog, insomnia, depression, concentration impairment, memory issues, and anxiety), palpitations, dizziness, tingling, joint pain, tinnitus, ear pain, nausea, persistent fever, dermatologic complaints (rashes and hair loss), and a decline in quality of life (Aiyegbusi et al, 2021; Nalbandian et al, 2021; Premraj et al, 2022; Weng et al, 2021).
Possible etiology of Long Covid
Several studies have investigated how severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections can lead to Long Covid infection. The 3 most important causes suggested are immune dysregulations, viral persistence, and autoimmunity. These are biological factors that commonly contribute to long-term symptoms due to viral infections. On the other hand, individual patients may develop Long Covid through different biological factors such as organ damage, clotting/coagulation issues, and host-microbiome/virome interactions, and reservoirs of SARS-CoV-2 may persist in particular tissues, or neurotrophic pathogens can be reactivated (Proal and VanElzakker, 2021). However, a precise reason behind PCS is yet to be proven.
Despite the above causes, gender is one of the risk factors that showed a noticeable association with the Long Covid syndrome. Women are more likely than men to develop Long Covid symptoms (Bai et al, 2022). The reasons why the female gender is more at risk of Long Covid might be more immune response and autoimmunity, which is common in middle-age women. Men have different adaptive and innate immune responses than women, and probably hormonal mediators play a key role in these variations (Ciarambino et al, 2021). Higher age has been identified as another risk factor.
A study has shown that the number of people older than 70 years, who reported symptoms lasting 4 weeks or longer, has been more than those 18–49 years of age (Sudre et al, 2021). Autoantibodies neutralizing type I interferon (IFN) sharply increase with age, and evidence has shown that this is prevalent in COVID patients older than 70 years (Bastard et al, 2021).
Immune dysregulations in post-COVID disorders
Dysfunctional innate and adaptive immune mechanisms can cause uncontrolled immune responses that have been called immune dysregulation disorders, which in patients with COVID can be characterized by an alteration of innate and adaptive immune cells or cytokines. In addition, some of these changes are able to sustain in convalescent individuals for a prolonged period after infection and can cause postinfectious syndromes similar to SARS-CoV-1 and Ebola (Clark et al, 2015; Ngai et al, 2010). A study has shown that the population of CD8+ and CD4+ T cells, which express PD-1, and T regulatory cells were decreased in PACs, and on the contrary, the number of B cells and the CD14+, CD16+, and CCR5+ monocytic subset was increased considerably compared to healthy controls (Patterson et al, 2021).
Furthermore, Wen et al (2020) by use of the single-cell RNA sequencing technique have indicated that the ratio of CD4+ and CD8+ T cells decreased remarkably in recovered individuals' peripheral blood mononuclear cells, whereas plasma B cells and CD14+ monocytes with high inflammatory gene expression significantly increased. Another study has reported that, while the level of NKG2A in CD8+ T cells and natural killer (NK) cells increased in SARS-CoV-2-infected patients, it returned to baseline in convalescence (Zheng et al, 2020). Also, some studies have identified the existence of SARS-CoV-2–specific T cells in convalescent patients (Grifoni et al, 2020; Ni et al, 2020).
The cytokine interleukin (IL)-1β is one of the key mediators of inflammatory responses, activated by infection, and consequently can activate other proinflammatory cytokines, such as IL-6 (Nieto-Torres et al, 2014). IL-6 and IL-1β make a contribution in the cytokine storm and play a key role in inflammatory mechanisms (Conti et al, 2020; Zhou et al, 2020). IFN-γ (type II IFN) is a cytokine produced by a large number of neutrophil granulocytes, macrophages, lymphocytes, dendritic cells, and monocytes, and participates in inflammatory processes, signal transduction, and antiviral immunity. Also, it can act as a proinflammatory or anti-inflammatory cytokine (Lees, 2015).
Cytokines, by regulating inflammation, control both adaptive and innate immune systems, and influence the immune responses. Therefore, dysregulation of cytokine expression might be involved in Long Covid symptoms. The elevated levels of IL-1β, IL-6, IFN-γ, and TNF-α (tumor necrosis factor-alpha) have been detected in blood and plasma samples of people who recovered from COVID-19. On the contrary, CCL4 and GM-CSF were at remarkably lower degrees in comparison with healthy controls (Andrade et al, 2021; Files et al, 2021; Ong et al, 2021; Patterson et al, 2021).
Viral persistence
Viral persistence is equivalent to evasion of the host's immune system or failure to eradicate the virus from the infected host. More to the point, viruses are able to adjust the expression of each host gene and consequently their genome to acquire a residence in a nonlytic state inside the cells. So viruses can gain special strategies of replication (Oldstone, 2006). In most cases, the types of diseases that persisting viruses cause are often novel and unpredictable. A theory has been proposed that persistent virus would possibly stimulate each direct dendritic cell activation and cell damage, possibly ending in autoimmunity.
However, from a virologist's view, persistent infection and autoimmunity are considered 2 entirely different mechanisms, which might be a result of SARS-CoV-2 (Jacobs, 2021). Like all microorganisms, some methods are applied by SARS-CoV-2 to escape and deactivate the host immune reaction (Li et al, 2020c). Taefehshokr et al (2020) showed that these contain the potential to duplicate inside double-membrane vesicles that host microorganism pattern recognition receptors (PRRs) are unable to discover. The transfer of viral RNA genome from the envelope into the cytoplasm takes place after SARS-CoV-2 enters the cells, initiating the process of translation.
When RNA replicates, formation of new viral particles occurs, through the incorporation of fragments of the host cell membrane in the new viral envelope (Li et al, 2020c; Taefehshokr et al, 2020). Superantigens (Sags), are microbial products first discovered from examination of the overstimulation of T cells by Staphylococcal Enterotoxin B (Brown and Bhardwaj, 2021). It has shown that Sags have a substantial effect on the host's T cells and play a central role in SARS-CoV-2 infections (Darif et al, 2021). They are able to provoke a large amount of T cell population, setting off a huge immune response. Also, the stimulation power of Sags is much more compared to regular antigens as up to 10% of T cells respond, while common antigens might typically trigger simply 0.001%–0.01% of T cells (Dar et al, 2016; Guedez et al, 1997).
The mechanism of action of Sags is to bind to the variable region of the T cell receptor (TCR) and MHC class II molecules on the antigen-presenting cells, which results in the stimulating of several T cell lineages and production of IL-2 and different inflammatory cytokines (Fraser, 2011; Wieczorek et al, 2017). Therefore, Sags are considered a significant factor in the progress of autoimmune diseases by crossing the MHC class II molecule of B cells with the TCR on T cells (Marrack and Kappler, 1990; Rokni et al, 2020).
Besides serving as pathogen-associated molecular patterns, virus particles can promote a substantial innate primary immune response, which might be owing to its Sags following recognition by Toll-like receptor 7 (TLR7). Bartoletti et al (2021) found that the mortality rate in critically ill COVID-19 patients is decreased by corticosteroids as well as suggested a necessity for immune suppression. In many patients, Sags response is normally downregulated and consequently, the Sags-induced immune stimulations are all, but effective in creating immune responses (Miyashita et al, 1995). The virus can replicate inside body, particularly where the response of the immune system is moderately fragile due to the negative immunological feedback loop (Hassett et al, 2020; Nabavi, 2020).
One common approach to limit virus replication is using partial activation of the IFN reaction, which is an incredibly potent antiviral reaction that has co-developed among viruses and hosts for many years and is a planned response playing a pivotal part in the regulation of a number of viral infections. Regulating this innate immunity has a role in viral persistence (Lanford et al, 2011; Schultz et al, 2015); on the other hand, Long Covid is an immunologic response to the persistence of SARS-CoV-2 (Buonsenso et al, 2022).
Autoimmunity
There have been many factors that may cause the initiation or intensification of autoimmune diseases such as bacterial infections, viral fungal, and genetic predisposition. Furthermore, such agents have affected vulnerable people to autoimmunity at 3 levels: the specific antigen and its presentation, the target tissue, and the general reactivity of the immune system (Campbell, 2014; Khan and Wang, 2019). Several pathogenic viruses are believed to trigger and initiate autoimmune diseases, including Hepatitis A and C virus, Rubella virus, HTLV-1, Cytomegalovirus, Herpes virus-6, Parvovirus B19, and Epstein-Barr-virus, and Coronavirus (Ehrenfeld et al, 2020; Smatti et al, 2019).
It has been proposed that the shared pathogenetic mechanisms and clinical-radiological conditions among COVID-19 and the hyperinflammatory illnesses could advocate that SARS-CoV-2 is able to promote a rapid autoimmune or autoinflammatory dysregulation, leading to the severe opening pneumonia, in genetically prone people (Caso et al, 2020; Tan et al, 2021). Inherited disorders of type I IFN immunity and auto-antibodies, which neutralize type I IFNs, caused lethal COVID-19 lung inflammation by meddling with type I IFN immunity in blood plasmacytoid dendritic cells and tissue-resident respiratory epithelial cells (Escobedo et al, 2021; Ricci et al, 2021; van der Wijst et al, 2021; Zhang et al, 2022), and the diffusion of the virus during the first few days of illness is promoted by both of these elements. Moreover, ∼15% of acute COVID-19 patients had auto-antibodies to IFN-α, IFN-ω, and IFN-β in their blood samples.
In addition, the defensive power of type I IFN-α2, IFN-β, and IFN-ω against SARS-CoV-2 is hindered by such auto-antibodies in a culture dish. Also, these autoantibodies have no longer been observed both in infected individuals who have been symptomless or had gentle phenotypes or in healthy people. Simultaneously, such studies establish a method by that individuals at the highest risk of severe COVID-19 are identified (Bastard et al, 2020; Beccuti et al, 2020). Nevertheless, other types of autoimmunity related to SARS-CoV-2 infection are X-linked recessive TLR7 and plasmacytoid dendritic cell deficiency (Onodi et al, 2021; Zhang et al, 2007).
Interferons
The types of IFNs
As a family of cytokines, IFNs have a significant part in the host's adaptive and innate immune responses in vertebrates. Known human IFNs are classified into types I, II, and III based on the use of their receptor (Akamatsu et al, 2021). Type I IFNs including 13 IFN-αs, IFN-β, IFN-ɛ, IFN-κ, and IFN-ω, can be produced by many cell types (Severa et al, 2020). IFN type II (IFN-γ) is largely produced by CD4+ and CD8+ T cells and NK and NK T cells, which are involved in adaptive and innate immune systems (Schoenborn and Wilson, 2007). A great amount of type III IFNs consisting of IFN-λ1, IFN-λ2, and IFN-λ3 are produced by epithelial cells of hepatocytes and type 2 myeloid dendritic cells (Grajales-Reyes and Colonna, 2020; Syedbasha and Egli, 2017).
The expression of type I and II IFN receptors takes place on approximately every nucleated cell, while the expression of IFN type III receptors occurs on epithelial, neutrophil, and dendritic cells (Galani et al, 2017). As a responding mechanism to viral infection, distinct IFNs are secreted by the detection of viral nucleic acid in the cytoplasm through intracellular PRRs. IFNs are affected by inducing ∼2,000 products of IFN-stimulated genes (ISGs), and their expression is predominantly controlled through the Janus kinase ( JAK)/signal transducer and activator of transcription (STAT) pathway (Fig. 1) (Onomoto et al, 2021; Schoggins, 2019).
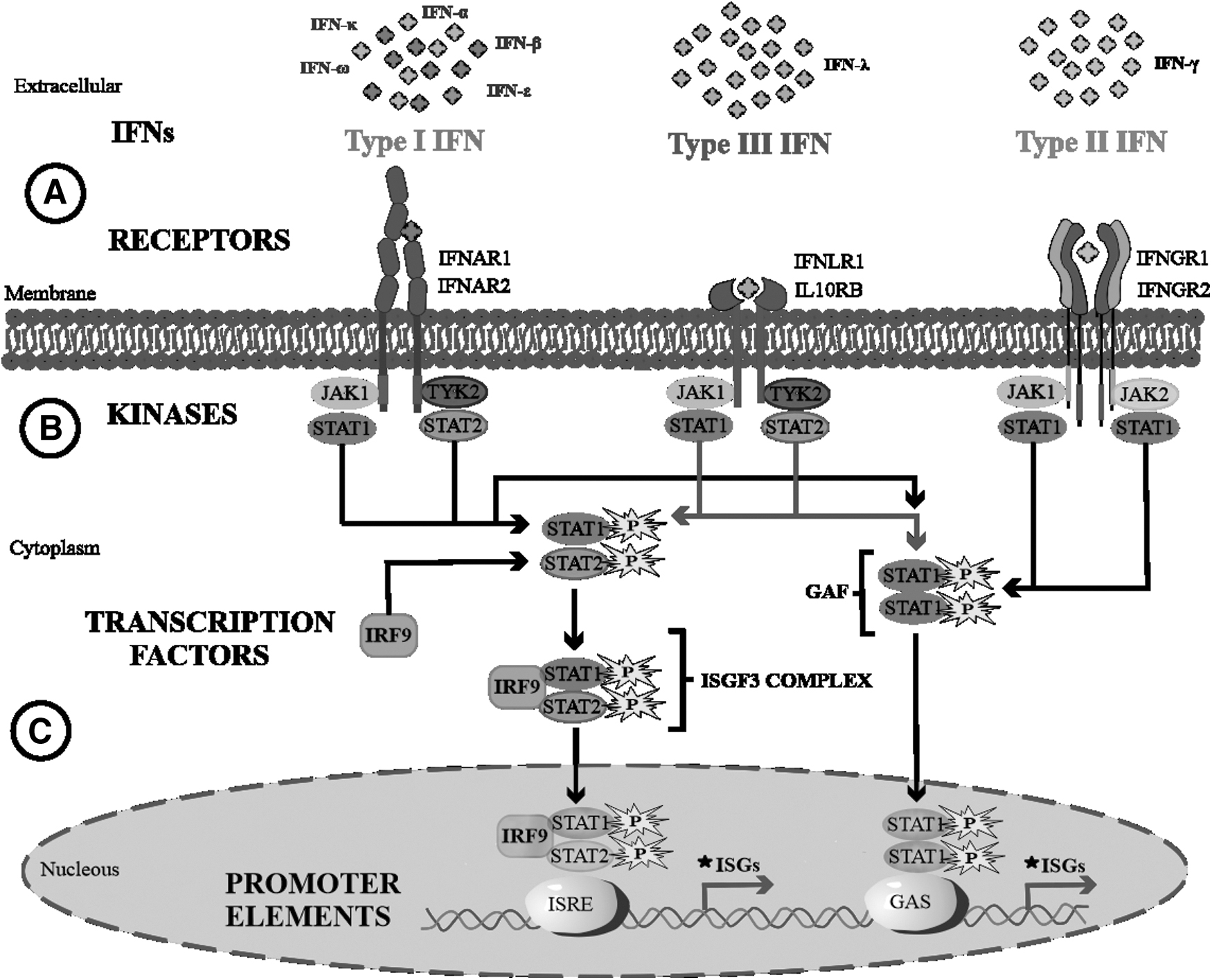
The signaling pathway of IFNs from extracellular to nucleus.
Long Covid lasts longer than 12 weeks. Type I and III IFN levels, also IFN-γ, highly increase in individuals after resolution of active SARS-CoV-2 infection at month 4 after infection. It is shown that an increased expression of type I IFN (IFN-β) and type III IFN (IFN-λ1) is consistently high at 8 months after initial mild-moderate infection in the Long Covid group compared to asymptomatic controls (recovered patients). Due to the IFN-γ high level produced by CD8+ T cells at 8 months after infection, it has recently been considered a predictor of postacute COVID-syndrome (Phetsouphanh et al, 2022).
In another study, the production of IFN-γ has been studied in CD4+, Treg, and CD8+ T cells, and the results showed an increase in the production of IFN-γ in Treg cells in severe convalescent patients at 3 months after the infection. This result was not observed for mild-moderate patients and healthy individuals. However, 6 months after the infection, IFN-γ production was significantly decreased in both CD4+ and Treg cells, especially in severe Long Covid patients (Wiech et al, 2022). Colarusso et al (2021) found that IFN-β is significantly lower in severe Long Covid compared to moderate Long Covid patients.
The role of IFNs in COVID-19 (both protective and deleterious effects)
The SARS-CoV-2 virus' cytopathic effects lead to the death of lung alveolar epithelial cells. Differentiation and proliferation of adjacent progenitor epithelial cells recover the lung (Kikkert, 2020). Type I IFNs are considered more proinflammatory in comparison to type III IFNs, even though both type I and III IFNs are regarded as significant mediators of the innate immune responses (Galani et al, 2017). Increased IFN-λ stimulates apoptosis and p53 gene expression, which results in impaired repair of damaged lung epithelial cells and increased morbidity of COVID-19 disease (Fig. 2A–E) (Hadjadj et al, 2020; Major et al, 2020). It was shown that in patients with severe COVID-19, the production, signaling, and activity of type I IFNs are impaired, which appears to be associated with inherent errors in the signaling cascade or the production of autoantibodies, particularly to IFN-α or IFN-ω.
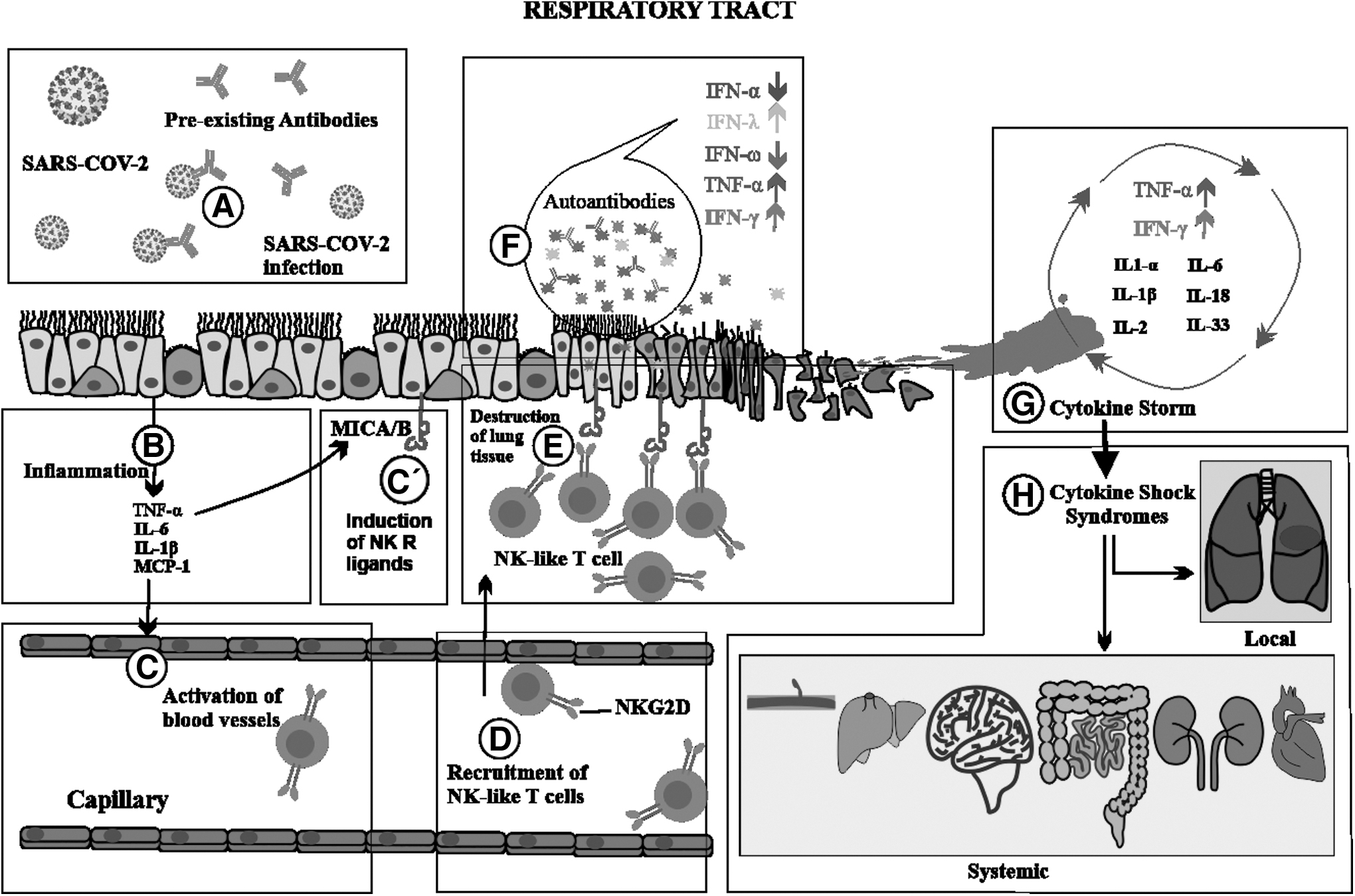
Human RT infection by SARS-CoV-2. RT infection by the virus may be inhibited by pre-existing neutralizing antibodies resulting from the previous infection with seasonal coronaviruses
Interestingly, the presence of these autoantibodies was relatively higher in elderly and patients who were males and had severe COVID-19 (Ackermann et al, 2020; Beck and Aksentijevich, 2020; Zhang et al, 2020a). Also, cohort longitudinal analysis shows higher IFN-α2 amounts in female patients compared to their male counterparts (Takahashi et al, 2020). In viral infections, type II IFN or IFN-γ helps to differentiate CD8+ T cells into cytotoxic T lymphocytes (CTLs). CTLs with the production of effector molecules and cytokines confine the replication of virus and destroy cells that are infected.
Also, IFN-γ increases CD4+ and CD8+ memory cells (Karki et al, 2021; Whitmire et al, 2007). Recent studies show that a high amount of IFN-γ is produced in moderate to severe COVID-19 patients (Sadanandam et al, 2020). From among the increased 10 different cytokines in such patients, only the combination of IFN-α and IFN-γ induces the PANoptosis process as an innate immune inflammatory-programmed cell death pathway. Interestingly, these cytokines in combination with other inflammatory cytokines or alone cannot promote this process (Sadanandam et al, 2020). Recent studies show that in addition to the important role of the combination of IFN-γ and IFN-α in lethal cytokine shock, it is similarly related to the recovery-like stage of COVID-19 patients (Fig. 2F–H) (Ziegler et al, 2020).
The signaling pathway of IFNs in Long Covid
The JAK-STAT pathway is activated by binding the ligand to type I, II, and III IFN receptors. After the activation of receptors by ligand binding, kinases associated with these receptors are mediated by IFN signaling. The produced type I IFNs by the host as the first defense mechanism, by binding to complex IFN-α/-β receptors (IFNAR), induce different downstream ISG expressions. Upon phosphorylation of the STAT1/STAT2 by Jak1 and tyrosine kinase 2 (Tyk2), the phosphorylated STAT1/STAT2 heterodimers along with IRF9 (interferon regulatory factor 9) form an ISGF3 complex, which, after entering to the nucleus, stimulates the transcription of genes that possess promoters called ISRE (interferon-stimulated responsive element) (Cao et al, 2019; Fish and Platanias, 2014; Schneider et al, 2014).
Type III IFNs bind to heterodimers IFNLR1/IL-10RB (interleukin-10 receptor B). Activated ISGF3 resulting from IFN-II action, stimulates the transcription of ISGs with the ISRE promoters. Both type I and type III IFNs along with promoting the formation of STAT1/STAT1 homodimers. Phosphorylated STAT1 homodimers as IFN-γ-activated factor (GAF) by going to the nucleus and binding to the Gamma interferon activation site (GAS) (IFN-γ-activated site) elements, which exist in the promoter of some ISGs, stimulate the transcription of genes with the GAS promoters.
The receptor of type II IFN (IFN-γ) is composed of IFNGR1 and IFNGR2 subunits. The binding of IFN-γ to its heterodimeric receptor activates JAK1/2 associated with the receptor that induces the formation of GAF resulting in stimulating transcription of genes with GAS elements (Akamatsu et al, 2021; Platanias, 2005). It is demonstrated that the Envelope protein (E) of the SARS-CoV-2 virus triggers the transcription of ISGs, unlike creating a permissible environment for the virus replication, while Nucleocapsid (N) and Membrane (M) proteins inhibit the IFN-Is signaling pathway (Li et al, 2020b), and nonstructural protein (NSP1) blocks IFN-α stimulation by inhibiting STAT1 phosphorylation (Xia et al, 2020).
It has been shown that diverse ISGs, including STAT2, MX2, and IRF7, are upregulated during COVID-19 infection, which are able to suppress viral replication (Israelow et al, 2020). Several studies have indicated that insufficient production of type I IFNs or mutations in the IRF7 and TLR3 genes leads to more vulnerability to COVID-19 infection and illness severity (Li et al 2020a; van der Made et al, 2020). Fallerini et al demonstrated that TLR7 missense variants negatively affect TLR7 downstream signaling and IFN-associated expression of genes (Fallerini et al, 2021). Experiments show that homozygosity of the interferon-induced trans-membrane protein 3 (IFITM3) gene rs12252 C allele is associated with disease severity in COVID-19 patients (Zhang et al, 2020b).
Furthermore, a significant correlation has been observed between severity of the illness and the existence of variants in genes associated with inflammatory responses such as TYK2. High expression of TYK2 and low expression of IFNAR2 are linked with life-threatening COVID-19 (Pairo-Castineira et al, 2021).
Bastard et al (2020) found IgG auto-Abs against IFN-α, IFN-ω, or both in some of the patients with a severe infection that had a role in neutralizing IFNs in these patients. In addition, their research showed that patients in whom auto-Abs against IFN-α2 were present possessed auto-Abs against 13 IFN-α subtypes, although some also had neutralizing auto-Abs against IFN-β. Interestingly, auto-Abs against IFN-Is are not a result of infection and pre-exist to infection (Bastard et al, 2020).
Another study revealed an increased presence of auto-Abs against IFN-Is in the COVID-19 patient's group compared to the control group and there is a positive correlation between the number of these auto-Abs and the severity of the disease (Wang et al, 2021). Furthermore, in inflammatory conditions, other microbiomes and viromes could also be involved in the production of autoantibodies and cause a wide variety of auto-Abs reactivity. Such complicated situation could describe a considerable percentage of clinical variations identified in Long Covid patients (Ortona and Malorni, 2022).
Methods of diagnosing and treating Long Covid
Although the serious medical effects of Long Covid are increasing, there are still no definitive diagnostic criteria (
In fact, these symptoms are sometimes caused by an undiagnosed health condition or an underlying disease caused by COVID-19 (Centers for Disease Control and Prevention, 2022; Lopez-Leon et al, 2021). Hence, it is necessary to confirm the initial infection and then rule out other diseases with similar symptoms such as rheumatoid arthritis or lupus, and as the differential diagnosis is continued, the Long Covid is diagnosed. The type of treatment is usually determined based on individual symptoms and includes antiviral drugs and modulation of IFNs, immunotherapies such as plasma exchange, and steroids (Michaud, 2021).
The diagnostic methods used by clinicians are X-ray, ultrasound, computed tomography, or magnetic resonance imaging to recognize alterations, including inflammation or scarring in the lungs or heart. Laboratory testing may be helpful for Long Covid's diagnosis (The New York Times, 2022). Lung performance tests are the primary test to determine lung function, volume, and performance. Another widely used test is the blood test for measuring heart rate, blood pressure, oxygen saturation, thyroid hormones, and inflammatory markers. Polymerase chain reaction is not a decisive tool to diagnosing Long Covid.
Neutrophils are one of the early signs of SARS-CoV-2 infection (Taefehshokr et al, 2020). Finally, based on experiences, serological tests to measure cytokines and IFNs are more accurate and helpful in diagnosing Long Covid infection, because type 1 and type 3 IFNs are often produced in the early stages of a viral infection and cause inflammation by activating immune cells called T cells (Stanifer et al, 2020).
The role of IFNs in the diagnosis and treatment of Long Covid
Researchers have considered IFN-α as an effective treatment for Long Covid syndrome (Zhang et al, 2020a) because the innate immune system endows the production of IFN-α as the first defense line against viruses (Fung and Liu, 2019; Zhang et al, 2020a). Patients with severe COVID-19 show IFN insufficiency, which can potentially lead to immune escape from the virus (Blanco-Melo et al, 2020). A recent study showed that patients experienced a serious clinical condition in the absence of IFN-α (Schoggins, 2019; Trouillet-Assant et al, 2020). The Chinese National Health Commission guidelines suggested recombinant aerosol IFN-α for treatment of SARS-CoV-2, because IFN-α prevents the virus replication, in vitro (Mantlo et al, 2020).
Therefore, it seems that the early administration of IFNs can prevent the rapid spread of the virus and subsequent cytokine storms (Davidson et al, 2016; Taefehshokr et al, 2020). However, due to its immune-regulating role, IFN-α can cause side effects such as severe inflammatory response, tissue damage, and pathogenicity (Zhang et al, 2020a). Nevertheless, the problem is that long-term COVID patients have an overactive innate immunity with a deficiency of B and T cells, which manifests itself as a high expression of type I and III IFN that remains elevated continuously for 8 months after infection (Davidson et al, 2016). Studies have shown that administration of IFNs before a severe viral infection and the onset of the inflammatory phase of the disease can have a protective effect.
Nevertheless, IFN treatment after the onset of inflammation and exacerbation of the disease can lead to long-term immunopathology (Channappanavar et al, 2019). Therefore, it has been necessary to pay attention to the appropriate administration time for the optimal performance of IFNs. Further analysis of the clinical efficacy of IFN for COVID-19 patients with varying degrees of severity and selecting the appropriate timing and its optimal regimes could result in safe and more effective treatment for COVID-19 (Zanoni, 2021).
Increase of IFNs following inflammation can result in serious illness and injury, prolong the disease, and make treatment more challenging, so the treatment of COVID-19 disease includes reducing the inflammatory response caused by IFN in various organs (Akamatsu et al, 2021; Yang et al, 2021). Thereby, measurement of IFN level and analysis of its subtypes during SARS-CoV-2 infection can provide more accurate treatment for viral infection, as well as immune response damage (Yang and Shen, 2020).
IFNs might serve as drug candidates for enhancing antiviral effects, while minimizing immunopathology when those subtypes are identified or combined with other antiviral drugs. It has been tested clinically in patients with long COVID-19, in combination with lopinavir/ritonavir (LPV/r). In contrast to those receiving oral LPV/r, patients receiving intravenous injection of IFN-α2b, in combination with LPV/r, experience shorter hospital stays and higher viral clearance rates (Sodeifian et al, 2022). In addition, administering IFN-α2b with arbidol decreased the duration of infection and inflammatory cytokine IL-6 levels in the upper respiratory tract (Zhou et al, 2020a). Furthermore, Cuban clinical studies have confirmed the efficacy of IFN-α2b against COVID-19 (Pereda et al, 2020). Similarly, patients with severe Middle East respiratory syndrome-related coronavirus infection treated with a combination of IFN-α2a and ribavirin experienced a significantly improved survival rate of 14 days (Shalhoub et al, 2015).
This study's findings show that IFN-I treatment is an effective treatment for COVID-19. Although delayed IFN-I treatment was unable to effectively inhibit virus replication, it was associated with an increase in proinflammatory cytokine expression and neutrophil infiltration in the lungs, resulting in fatal pneumonia. Therefore, IFNs for COVID-21 must be used with a balance between antiviral and immunological effects (104). An Adam Mickiewicz University study confirms these findings that limiting signaling cascades set off by inflammatory cytokines and IFNs is key to preventing systemic inflammation. Thus, targeting STAT family members can be suggested as a new treatment strategy in patients with severe COVID-19 (Yang et al, 2021).
Other antiviral drugs include (eg, favipiravir, remdesivir, LPV/r, and ribavirin), polyclonal or monoclonal antibodies against SARS-CoV-2 (eg, casirivimab/imdevimab, bamlanivimab/etesevimab), plasma during convalescence and immune modulating factors (eg, IFNs, corticosteroids, tocilizumab, and baricitinib) Recommended for treatment (Tsang et al, 2021). Angiotensin-converting enzyme inhibitors or angiotensin II type I receptor blockers are recommended for patients with COVID-19 (Jean et al, 2020; Vallianou et al, 2021). Also, the serum level of creatine kinase and lactate dehydrogenase could portent a positive reaction to COVID-19 treatment (Yuan et al, 2020).
The results of a randomized study showed patients who received a combination of lupinavir and IFN-β1a/ritonavir/ritonavir uratazanavir/with hydroxychloroquine in the primary stage of disease received faster treatment (Ader et al, 2021). Therefore, research is now directed toward immunomodulatory agents other than antiviral drugs. With the combined use of IFNs, the optimal timing, and route of its use, a safe and effective antiviral treatment for COVID-19 can be created (Sodeifian et al, 2022).
Conclusion
In conclusion, in this review, we discussed the double-edged role of IFNs in Long Covid infection. Three potential causes attributed to this syndrome are viral persistence, autoimmunity, and immune dysregulation. The signaling pathway of type I IFNs is impaired owing to inherent errors in the signaling cascade and autoantibodies that neutralize IFN-α and IFN-ω causing lethal COVID-19, especially in elderly people.
Declaration
All authors are supported by institutions engaged in education or medical research.
Footnotes
Authors' Contributions
M.K., S.F., and F.G.-H. conceived and designed the study and collected the data. S.G. and N.B. prepared figures. H.R.R.J., N.Z., and N.B. participated in editing and revising the initial drafts of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a grant from the Biotechnology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran (Grant No. 64815).