
Abstract
Interleukin-17 (IL-17) and tumor necrosis factor (TNF) regulate tissue remodeling through matrix metalloproteinases (MMPs). It is not yet clear whether these cytokines have a functional hierarchy in psoriasis. Serum levels of TNF (1,403 versus 1,058 pg/mL), IL-17 (1,528 versus 820 pg/mL), MMP-1 (1,999 versus 1,039 pg/mL), and MMP-9 (1,950 versus 1,561 pg/mL) were higher in psoriasis subjects (n = 60) than in control subjects (n = 60). Tissue inhibitor of MMPs (TIMP-1; 1,374 versus 1,218 pg/mL) was lower in psoriasis subjects. Serum IL-17 was correlated with MMP-2 (rs = 0.40) and TIMP-1 (rs = −0.26) levels. Unstimulated production of MMP-1, MMP-2, and MMP-9 by monocytes was higher in psoriasis subjects, whereas TIMP-1 production was lower. TNF stimulation increased all MMPs, whereas TIMP-1 production was unchanged. IL-17 stimulation increased all MMPs, whereas TIMP-1 production was decreased in psoriasis subjects. MMP-9 production was higher in monocytes stimulated with IL-17 compared with TNF. TIMP-1 production was decreased more by IL-17 than by TNF, but only in psoriasis cells. MMP-1/TIMP-1, MMP-2/TIMP-1, and MMP-9/TIMP-1 ratios were higher after IL-17 stimulation (compared with TNF stimulation) in psoriasis subjects; this occurred in controls only for the MMP-2/TIMP-1 ratio. IL-17 has a greater ability than TNF to dysregulate the MMPs/TIMP-1 balance, supporting IL-17 blockade as first-line treatment in cutaneous psoriasis.
Introduction
Psoriasis is a multisystem inflammatory disease that mainly affects the skin (and joints) with epidermal thickening, parakeratosis, and leukocyte infiltration. Beyond genetic susceptibility and environmental factors, immune dysregulation is a major contributing factor to the disease (Alexander and Nestle, 2017). The pathophysiology of psoriasis includes an intricate network of cells that, through cytokines and other soluble mediators, initiate and maintain an infiltration of the epidermis by immune cells, such as macrophages and neutrophils. Innate immune cells produce key cytokines, particularly tumor necrosis factor (TNF) and interleukin (IL)-6, which activate myeloid dendritic cells (mDCs).
Activated mDCs present antigens and secrete mediators, including IL-23, leading to the differentiation of T helper (Th) 17 cells. Th17 cells secrete IL-17 and IL-22 that activate keratinocytes and induce the overproduction of proinflammatory cytokines and chemokines (Alexander and Nestle, 2017). These mediators feed back into the inflammatory circuit and shape the inflammatory infiltrate. Keratinocytes and infiltrating leukocytes produce matrix metalloproteases (MMPs) that degrade and remodel extracellular matrix proteins and glycoproteins. The MMPs are also involved in cell differentiation, angiogenesis, cell proliferation and migration, apoptosis, and wound healing. Through these functions, MMPs are end-effector molecules of the tissue damage seen in psoriasis (Amezcua-Guerra et al, 2018).
Inflammatory circuits established during disease activity represent a pathogenic challenge and a therapeutic opportunity for anticytokine drugs. The advent of targeted therapies in the last quarter century has given us quite effective drugs. Since biologic therapies interact with a cytokine (such as TNF, IL-17, or IL-23) in a specific manner, these drugs have revolutionized the ability to treat psoriasis compared with more widespread immunosuppression with conventional immunosuppressant drugs such as methotrexate (Brownstone et al, 2021).
However, a flawed characterization of the role of major cytokines in psoriasis and the scarcity of head-to-head clinical trials comparing different anticytokine therapies have prevented clinical consensus on the sequence in which biological therapies should be started or switched. The main guidelines on the systemic treatment of psoriasis continue to place anticytokine drugs at the same hierarchical level, regardless of whether they are directed against TNF or IL-17 (or other molecular targets, such as IL-12 and IL-23) (Nast et al, 2020; Smith et al, 2020; Menter et al, 2019).
Therefore, we consider it important to clarify whether cytokines are hierarchically involved in the pathophysiology of psoriasis, to eventually transfer this knowledge to medical practice. To shed light on this topic, we performed in vitro stimulation with TNF or IL-17 on monocytes from psoriasis patients to assess their MMPs production, assuming a differentiated response for each.
Patients and Methods
Study participants
This study was conducted on outpatients with plaque psoriasis from a single dermatology clinic. Patients with arthritis or any concurrent autoimmune disorder and those receiving steroids or biologics were excluded. Pregnant patients and those with active infection, recent trauma or surgery, or neoplasia also were excluded. Clinical data were obtained at the time of blood sampling, including an assessment of disease activity using the Psoriasis Area and Severity Index. Nonpsoriatic individuals of the same age and gender were included as a reference.
The protocol was approved by our institutional review board (Comité de Ética del Instituto Nacional de Cardiología Ignacio Chávez; protocol number 18-1048). The study was performed following the 2013 Declaration of Helsinki. Patients consent to participate, authorizing the use of clinical data and blood samples for research purposes.
Laboratory procedures
Four milliliters of fasting venous blood was obtained in tubes containing a clot activator and serum gel separator. Blood was allowed to clot and centrifuge (600g, for 15 min at 4°C), and sera were collected and stored in aliquots at −75°C until use. Five milliliters of venous blood was additionally collected in tubes containing ethylenediaminetetraacetic acid; mononuclear cells were obtained using density gradient centrifugation with Histopaque-1077 (Sigma-Aldrich, St. Louis, MO), and CD14+ monocytes were isolated using the Magnisort CD14 Positive Selection Kit (Life Technologies, Carlsbad, CA).
A total of 5 × 105 CD14+ monocytes per well were cultured in RPMI-1640 medium supplemented with 10% of fetal calf serum (GIBCO, Grand Island, NY) +25 mM HEPES buffer +
Levels of MMP-1, MMP2, MMP-9, and tissue inhibitor of MMP-1 (TIMP-1) were measured in supernatants, whereas the levels of TNF, IL-17, MMPs, and TIMP-1 were measured in serum samples. For ELISAs (R&D Systems, Minneapolis, MN), serum samples were diluted 1:2, whereas supernatants were diluted 1:5. Measurements were performed in duplicate and the mean value was used for calculations.
Statistical analysis
Data distribution was evaluated using the D'Agostino-Pearson test. Consequently, categorical data are expressed as percentages and compared using Fisher's exact test. Continuous variables are expressed as medians with interquartile range and compared using the Mann–Whitney test (2 independent samples), the Wilcoxon signed-rank test (2 matched samples), or the Kruskal–Wallis test with Dunn's post-test (for multiple comparisons). Correlations were evaluated using the Spearman's rho (rs ) coefficient.
A P < 0.05 value was set for significance, and analyses were 2 tailed. Statistical analysis was performed using the SPSS v15.0 (SPSS Inc., Chicago, IL) and the GraphPad Prism v6.07 (GraphPad Inc., La Jolla, CA) software.
Results
One hundred and twenty individuals were enrolled in the study: 60 patients with psoriasis (48% women, median age 53 years) and 60 control subjects (55% women, median age 52 years). Table 1 summarizes the clinical data of the participants. Patients with psoriasis had a higher frequency of overweight, diabetes, and hypertension than controls.
Clinical and Laboratory Data of Study Participants
Data are presented as median (interquartile range) unless otherwise specified. Significant P values are in bold.
ACEi, angiotensin-converting enzyme inhibitors; ARBs, angiotensin receptor blocker; BMI, body mass index; HMG-CoA-R, hydroxymethylglutaryl-coenzyme A reductase; hs-CRP, high-sensitivity C-reactive protein; IL-17, interleukin-17; LDL-C, low-density lipoprotein cholesterol; MMP, matrix metalloprotease; NSAIDs, nonsteroidal anti-inflammatory drugs; PASI, psoriasis area severity index; TIMP-1, tissue inhibitor of MMP-1; TNF, tumor necrosis factor.
Serum from psoriasis patients was characterized by higher TNF (1,403, 584–1,486 pg/mL versus 1,058, 488–1,385 pg/mL; P = 0.005) and IL-17 (1,528, 1,193–2,291 pg/mL versus 820, 581–1,529 pg/mL; P < 0.001) than controls. MMP-1 (1,999, 1,102–3,413 pg/mL versus 1,039, 392–2,380 pg/mL; P = 0.004) and MMP-9 (1,950, 1,493–2,653 pg/mL versus 1,561, 1,280–2,094 pg/mL; P = 0.004) levels were also higher in psoriasis, but MMP-2 (743, 525–883 pg/mL versus 744, 644–835 pg/mL; P = 0.879) levels were not.
Serum TIMP-1 (1,218, 1,058–1,406 pg/mL versus 1,374, 1,076–1,853 pg/mL; P = 0.012) levels were lower in psoriasis patients than in controls. In psoriasis, serum IL-17 levels were directly correlated with MMP-2 (rs = 0.40) and inversely with TIMP-1 (rs = −0.26), whereas TNF did not show significant correlations (Fig. 1).
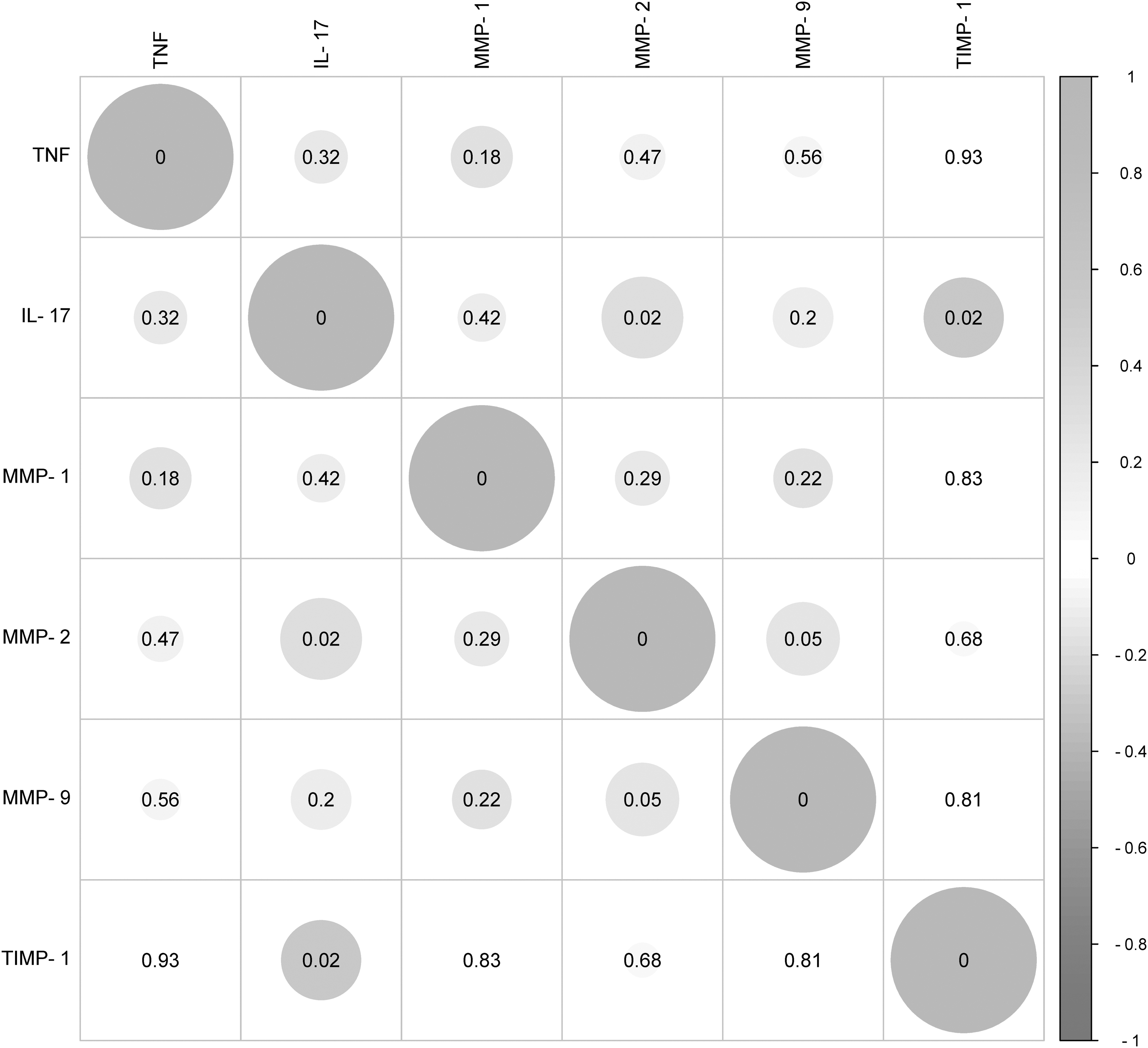
Correlation matrix between the serum levels of cytokines (TNF and IL-17) and those of MMPs and TIMP-1. The circles represent the intensity (size) and the direction (green, direct; red, inverse) of the association between variables. P values are presented inside each circle. IL-17, interleukin-17; MMP, matrix metalloprotease; TIMP-1, tissue inhibitor of MMP-1; TNF, tumor necrosis factor.
Basal production of MMP-1, MMP-2, and MMP-9 was higher in monocytes from patients with psoriasis compared with controls; TIMP-1 production, however, was lower (Fig. 2). TNF stimulation induced significant increases in the production of all MMPs, both in monocytes from psoriasis patients and controls; meanwhile, TIMP-1 levels in supernatants were unchanged. Similarly, IL-17 stimulation was associated with increased production of all MMPs in monocytes from psoriasis patients and controls. Nevertheless, IL-17 decreased TIMP-1 production in monocytes from psoriasis patients but not in control cells.

Levels of MMP-1
Regarding the MMPs/TIMP-1 ratios (Fig. 3), all were higher in cells from psoriasis patients than in controls at baseline. After stimulation with TNF, MMP-1/TIMP-1, MMP-2/TIMP-1, and MMP-9/TIMP-1 ratios increased in control cells, whereas this was true only for MMP-1/TIMP-1 and MMP-9/TIMP-1 ratios in psoriatic cells. IL-17 stimulation produced significant increases in the MMP-1/TIMP-1 and MMP-9/TIMP-1 ratios in patients and controls, whereas the MMP-2/TIMP-1 proportion increased only in cells from psoriasis patients.
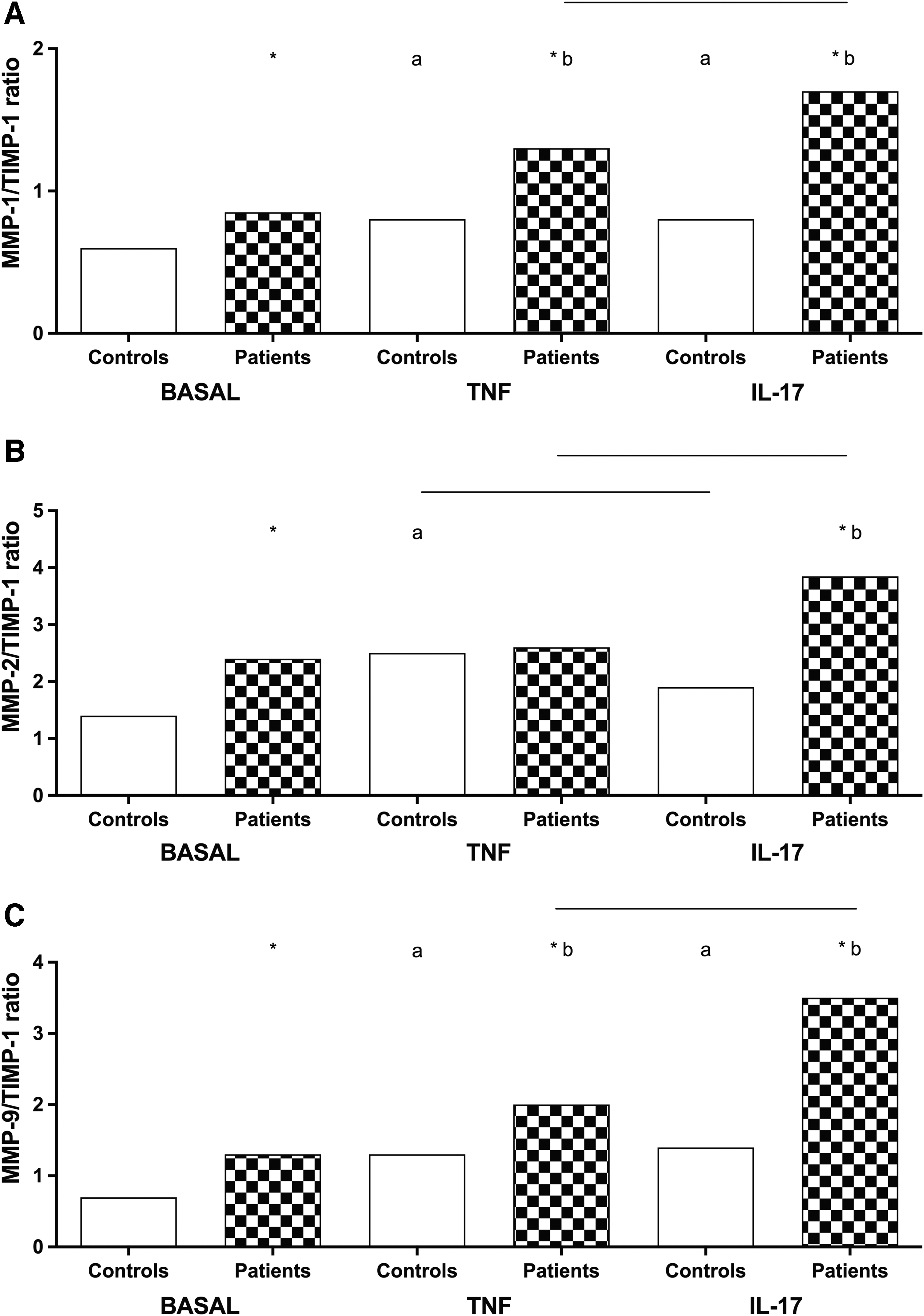
MMP-1/TIMP-1
In a final set of analyses, we compared MMP production depending on the cytokine used for stimulation (Figs. 2 and 3). The production of MMP-9 was significantly higher in monocytes stimulated with IL-17 than stimulated with TNF, both in cells from psoriasis patients and in controls. Meanwhile, TIMP-1 production decreased more with IL-17 than with TNF, but only in cells from psoriasis patients. There were no differences for MMP-1 or MMP-2. This differentiated response caused the ratios of MMP-1/TIMP-1, MMP-2/TIMP-1, and MMP-9/TIMP-1 in cell supernatant from psoriasis patients to be much higher after IL-17 stimulation than after TNF stimulation. In contrast, this phenomenon occurred in monocytes from control subjects only for the MMP-2/TIMP-1 ratio.
Discussion
This study investigated whether there is a hierarchical response of 2 prototypical cytokines in psoriasis. In this study, we found that IL-17 has a greater effect on dysregulating the production of MMPs and its tissue inhibitor, suggesting that IL-17 is a more relevant cytokine than TNF in guiding extracellular matrix degradation in cutaneous psoriasis.
Our finding of a hierarchical IL-17 response is supported by a recent meta-analysis on prognostic biomarkers of psoriasis progression. Indeed, LCE3D, IL23R, IL23A, NFKBIL1 loci, HLA-C*06:02 (genomic approach), IL-17, IgG aHDL, GlycA, I-FABP, and kallikrein 8 (proteomic approach) were identified as psoriasis markers. IL-17 and IL-23 molecules, which correspond to a Th17 phenotype, are the dominant cytokines that confer risk and severity for cutaneous psoriasis (Ramessur et al, 2022). Furthermore, the production of the principal MMP inducer (CD147 or basigin) by activated monocytes is a process dependent on Th17 cytokines instead of those of the Th1 phenotype (interferon-γ or TNF) (Amezcua-Guerra et al, 2020).
The IL-17 family comprises IL-17A, IL-17B, IL-17C, IL-17D, IL-17E, and IL-17F. They are mainly produced by Th17 cells in response to IL-23. IL-17A and IL17F are the most pathogenic in psoriasis. IL-17 receptors (IL-17R) are widely expressed in epithelial cells. Upon recognition of its ligand, IL-17R recruits ACT1, which binds to TNF receptor 6. Downstream signaling involves the mitogen-activated protein kinase and nuclear factor-κB pathways. IL-17 acts with IL-22 to induce the secretion of cytokines (such as TNF, IL-6, and IL-1β) and chemokines (including CXCL8, CCL, and CXCL1) by keratinocytes, epithelial cells, fibroblasts, macrophages, and other cells.
These proinflammatory mediators recruit additional Th17 cells and effector neutrophils, increasing local inflammation that ultimately results in the characteristic erythematous lesions of psoriasis. Th17 cells are not the only source of IL-17 in psoriasis. Other innate cell subsets produce this key cytokine and could thus be therapeutic targets for IL-17 blockade (Bugaut and Aractingi, 2021; Martin et al, 2013).
Early clinical trials revealed the therapeutic effect of TNF blockade with etanercept, a TNF receptor (p75): Fc fusion protein, in patients with plaque psoriasis (Papp et al, 2005; Leonardi et al, 2003). Subsequently, IL-17 blockade with secukinumab, an anti-IL-17 monoclonal antibody, was shown to have a superior therapeutic effect over etanercept in plaque psoriasis (Langley et al, 2014), although secukinumab failed to demonstrate overall superiority over adalimumab, an anti-TNF monoclonal antibody, in patients with active psoriatic arthritis having concomitant plaque psoriasis (McInnes et al, 2020).
However, secukinumab demonstrated consistently higher responses than adalimumab on all skin endpoints in these patients (Gottlieb et al, 2021). Ixekizumab, another monoclonal antibody that neutralizes IL-17, has been superior to etanercept in severe psoriasis (Griffiths et al, 2015).
Emerging evidence from laboratory and clinical trials supports that the IL-17 pathway is crucial in the pathogenesis of psoriasis, although this knowledge has not yet been fully translated into clinical practice (Ramessur et al, 2022; Bugaut and Aractingi, 2021; Amezcua-Guerra et al, 2020; Martin et al, 2013). Treatment guidelines from leading dermatological academic bodies still consider therapeutic IL-17 blockade to be on the same level as the use of TNF inhibitors to treat patients with moderate-to-severe disease and inadequate response to conventional systemic drugs (Menter et al, 2019; Nast et al, 2020; Smith et al, 2020). Our results highlight the need for head-to-head clinical trials that facilitate the transition of knowledge from the bench to the bedside.
In conclusion, IL-17 has a greater capacity than TNF to induce dysregulation of the balance between MMPs and their tissue inhibitor. This hierarchical supremacy supports the blockade of IL-17 as the first line of treatment in cutaneous psoriasis over TNF inhibitors.
Footnotes
Acknowledgment
Portions of this article are available as a Preprint repository in Research Square (
Authors' Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by M.F.O.-S., A.E.G.-P., and M.E.V.-M. Laboratory procedures were performed by R.S. Statistical analysis was performed by R.S. and L.M.A.-G. The first draft of the article was written by L.M.A.-G. and all authors commented on previous versions of the article. All authors read and approved the final article.
Data Availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
No specific funding was received from any bodies in the public, commercial, or not-for-profit sectors to carry out the work described in this article.