
Abstract
COVID-19, caused by the SARS-CoV-2 virus, has caused a global health crisis, necessitating a deeper understanding of its pathophysiology. In this study, we explored the immune and hematological dynamics in COVID-19 patients to gain insights into disease severity and prognosis. Our findings revealed distinct cytokine profiles in moderate and severe cases. IL12A was significantly upregulated in peripheral blood mononuclear cells from moderate cases, suggesting a potential role in initiating an effective immune response. Conversely, severe cases exhibited downregulation of key pro-inflammatory cytokines (IL23A, TNFalpha, IL1B, and IFNG) alongside an upregulation of the immunosuppressive IL10, indicative of a dysregulated immune environment. Serum analysis showed elevated IL6 and IL10 levels in both moderate and severe cases, emphasizing their potential as markers for disease severity. Notably, no significant differences in serum cytokines were found between recovery and lethal cases. In lethal cases of COVID-19, elevated D-dimer, urea, and creatinine correlated with IL6 and IL10. This study contributes valuable information to the ongoing efforts to understand and manage the dysregulated immune responses underlying COVID-19 pathology.
Introduction
COVID-19, resulting from infection with the SARS-CoV-2 virus, leads to a broad spectrum of symptoms and varying levels of severity. While most individuals have mild to moderate symptoms, others may develop severe conditions requiring hospital care. Compared with seasonal influenza, COVID-19 exhibits a higher mortality rate, showing that a greater percentage of infected individuals succumb to the virus. Furthermore, SARS-CoV-2 has been associated with the development of neurological and neuropsychiatric disorders. People who are older or have preexisting conditions such as heart disease, diabetes, chronic respiratory diseases, kidney disease, obesity, high blood pressure, or cancer are at a significantly increased risk of severe outcomes from COVID-19. (Basile et al., 2022; Beyrouti et al., 2020; Cavalli et al., 2020a; Ehrenfeld et al., 2020; Fogarty et al., 2020; Frontera et al., 2020; Rubino et al., 2020; Sheraton et al., 2020; Tancheva et al., 2020). There is also an extended, subchronic phase known as Neuro-COVID, characterized by symptoms ranging from loss of smell and taste to more severe conditions like encephalitis, strokes, and polyneuropathy (Latorre, 2022).
The varied symptoms associate to SARS-CoV-2 infection are known to originate from a dysregulated immune-inflammatory response, potentially leading to a condition referred to as a “cytokine storm (Cavalli et al., 2020b; Dharra et al., 2023; Du et al., 2023; Maison et al., 2023; Martonik et al., 2023; Taylor, 2022; Xu et al., 2023).
Understanding the immune and hematological aspects of COVID-19 is crucial for addressing effectively the pandemic (Basile et al., 2022; Dharra et al., 2023; Montazersaheb et al., 2022; Taylor, 2022; Ye et al., 2020).
As the pandemic evolves, it is vital to investigate the biological effects of SARS-CoV-2 infection in order to improve diagnosis, treatment, and prognosis strategies. This study aims to identify specific cytokine profiles across different levels of disease severity, offering potential therapeutic targets. By understanding the cytokine dysregulation occurring in COVID-19, we can design treatments that effectively modulate the immune response of the patients. Additionally, exploring early intervention strategies could transform clinical management, helping to prevent the escalation from moderate to severe conditions. In a time of new variants and widespread vaccination campaigns, insights from such studies not only deepen our understanding of the pandemic but also prepare us for future viral challenges. The evolving nature of infectious diseases underscores the ongoing need for thorough research, pivotal in shaping public health and clinical decisions.
Materials and Methods
Transcriptomic analysis
The transcriptomic data of peripheral blood mononuclear cells (PBMCs) from COVID-19 patients and healthy individuals were sourced from the GSE152418 dataset, available on the Gene Expression Omnibus database at https://www.ncbi.nlm.nih.gov/gds. This dataset includes profiles from 17 healthy individuals, 4 moderately symptomatic COVID-19 patients, 12 severely symptomatic COVID-19 patients (including 4 in ICU), and 1 recovering patient (excluded from this analysis). Data generation was performed using Illumina NovaSeq 6000 system, and analysis was conducted with the GREIN tool, accessible at https://shiny.ilincs.org/grein (Mahi et al., 2019).
Patients
Recruited patients
The study involved 60 individuals confirmed to have COVID-19 via RT-PCR testing for SARS-CoV-2. These patients were treated in the COVID-19 units of the Military Medical Academy in Sofia, comprising 34 males and 26 females with an average age of 61.38 ± 14.53. They stayed in the hospital for an average of 14.19 ± 5.88 days. The control group included 20 healthy blood donors matched by age and gender. The study protocols were approved by the Local Institutional Ethics Committee, and consent was obtained from all participants.
Clinical data
COVID-19 severity was categorized into mild, moderate, and severe cases. Mild cases had symptoms like mild upper respiratory infections, headache, and fever, maintaining oxygen saturation of ≥95%. Moderate cases involved symptoms such as pneumonia without severe manifestations, fever ≥38°C, and oxygen saturation ≤95% on room air. Severe cases involved significant respiratory distress (≥30 breaths per minute), oxygen saturation <90% at rest, PaO2 to FiO2 ratio ≤300, and extensive lung infiltrates. Critical cases required mechanical ventilation and ICU care. Data including demographic, clinical, lab results, and radiographical findings were collected within the first 24 h of hospital admission. Evaluations included counts of WBC, lymphocytes, platelets, basophils, eosinophils, and hemoglobin; CD3+, CD8+, CD4+, CD19+, and CD16+CD56+ lymphocyte counts; and levels of ALAT, ASAT, LDH, urea, creatinine, ferritin, CRP, PT, aPTT, TT, fibrinogen, and D-dimer. Initial lung assessments were conducted via chest radiography or CT scans.
Evaluation of cytokines in COVID-19
Venous blood samples from COVID-19 patients and healthy controls were collected into sterile tubes and stored at −80°C. Th1, Th2, and Th17 cytokine levels were measured using LEGEND-plex™ Human Th1/Th2 and Th17 Panel multi-Analyte Flow Assay Kits (BioLegend, San Diego, CA, USA), following the manufacturer’s instructions. Analysis was performed on a BD LSR II flow cytometer (BD Biosciences, Mountain View, CA).
Statistical analysis
Results are presented as mean ± SD. Data from flow cytometry were analyzed using FlowJo software. Normality was tested using the Kolmogorov–Smirnov, D’Agostino & Pearson Omnibus, and Shapiro–Wilk tests. Depending on these results, the Mann–Whitney or Kruskal–Wallis tests were applied, followed by Dunn’s post hoc test for significant differences. Spearman’s non-parametric test was used for correlation analyses. A significance level of P < 0.05 was set for all tests, with analyses performed using GraphPad Prism 9.
Results
Transcriptomic study
We made use of the whole-genome transcriptomic dataset GSE152418, generated on PBMCs from COVID-19 patients with different disease severity and healthy donors. As shown in Figure 1A–B, the transcriptomic analysis of PBMCs in COVID-19 patients revealed distinctive patterns associated with disease severity. Notably, IL12A exhibited significant upregulation in moderate cases, suggesting its potential role in orchestrating an effective immune response during this stage. Conversely, severe cases displayed a notable downregulation of pro-inflammatory cytokines, including IL23A, TNF, IL1B, and IFNG, accompanied by an upregulation of the immunosuppressive IL10.
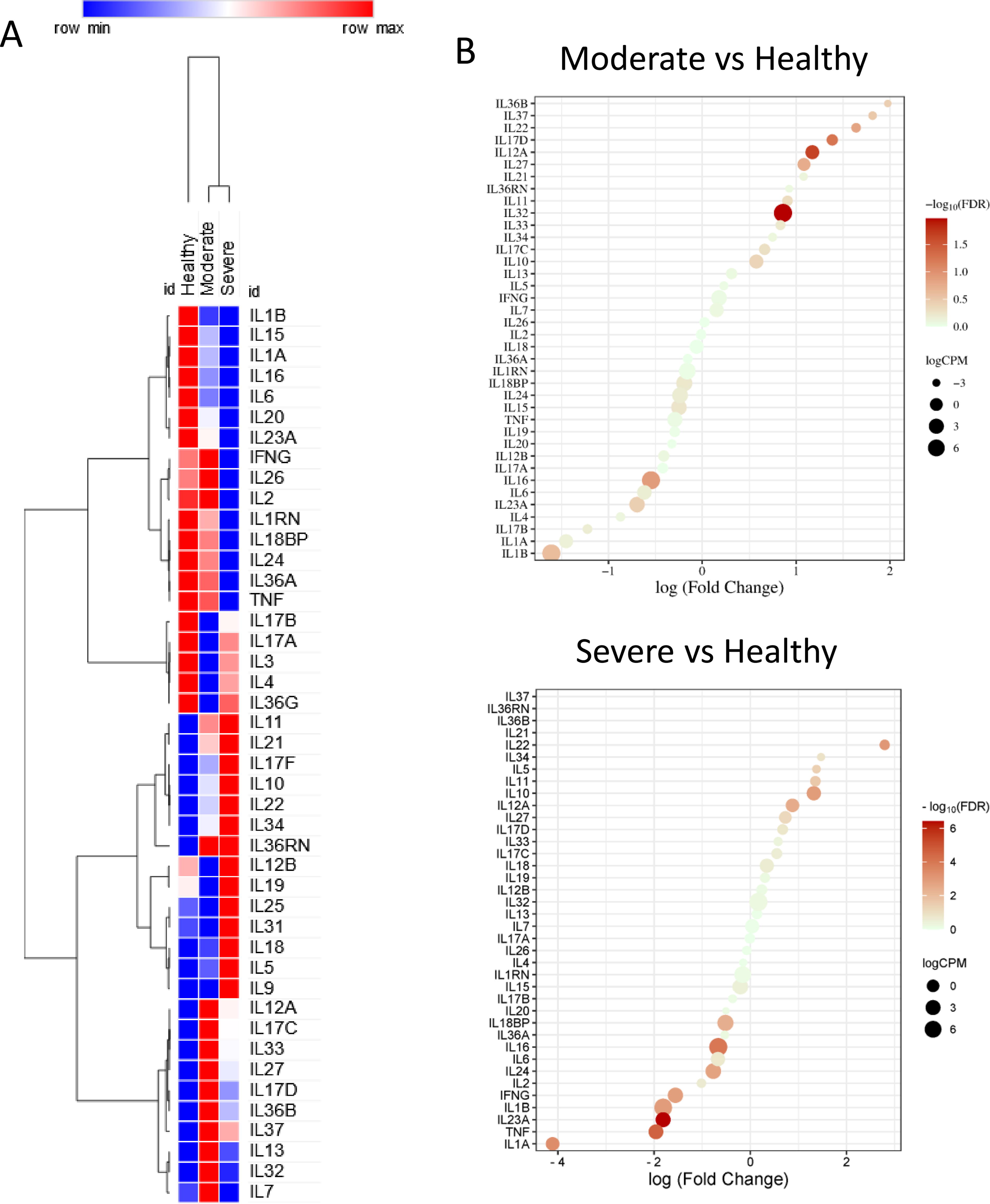
Transcriptomic analysis of PBMCs from COVID-19 patients, using the GSE152418 dataset.
Patients
COVID-19 patients’ distribution
The sera from 60 patients diagnosed with COVID-19 were separated into the 3 groups (20 patients each) based of the severity of disease: mild, moderate and severe. The mild disease group included 14 men and 6 women. The mean age was 55.6 ± 15.6. The moderate disease group was composed of 10 men and 10 women, with mean age 62.7 ± 12.2. The severe COVID-19 group included 10 men and 10 women, with a mean age of 65.9 ± 14.7. Among them, 2/10 men and 6/10 women died of COVID-19.
Cytokine levels in COVID-19 patients
We investigated the levels of cytokines in the sera and the blood parameters of COVID-19 patients and healthy donors by ELISA (Fig. 2). A significant increase in the levels of IL6 and IL10 was observed in both moderate and severe cases as compared with the control subjects (Fig. 2A). A trend of increase for Th1 levels was observed in all the COVID-19 cases, but no statistical significance was reached (Fig. 2B). Hematological parameters reflected distinct profiles in moderate and severe cases compared with mild cases, with a significant decrease in hematocrit (HCT), lymphocyte count, and an increase in granulocytes (Fig. 2C).

Evaluation of cytokines and blood parameters in COVID-19 patients and healthy donors.
Analysis of cytokines and blood parameters in recovered cases and lethal cases from severe COVID-19 patients
We next aimed to investigate whether there were differences in serum cytokine levels and blood parameters between recovered cases and lethal cases of severe COVID-19 patients. The results showed no significant differences in the cytokines’ levels between the recovered and lethal cases of COVID-19 (Fig. 3A). Accordingly, no differences were observed for Th1, Th2 and Th17 levels (Fig. 3B). On the other hand, significantly lower levels of HGB and HCT were found in lethal cases as compared to recovery cases (Fig. 4A), along with a significant increase in D-dimer, urea and creatinine (Fig. 4B). These latter parameters significantly correlated to IL-6 and IL-10 (Fig. 4C).
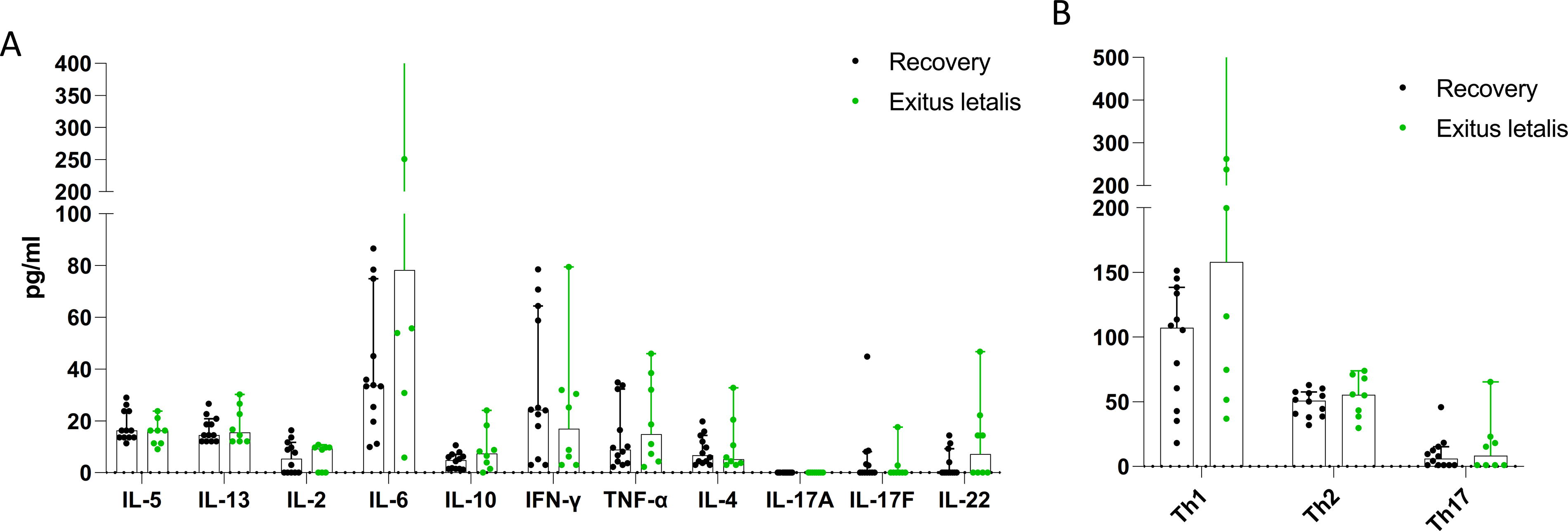
Evaluation of cytokines in severe COVID-19 cases.
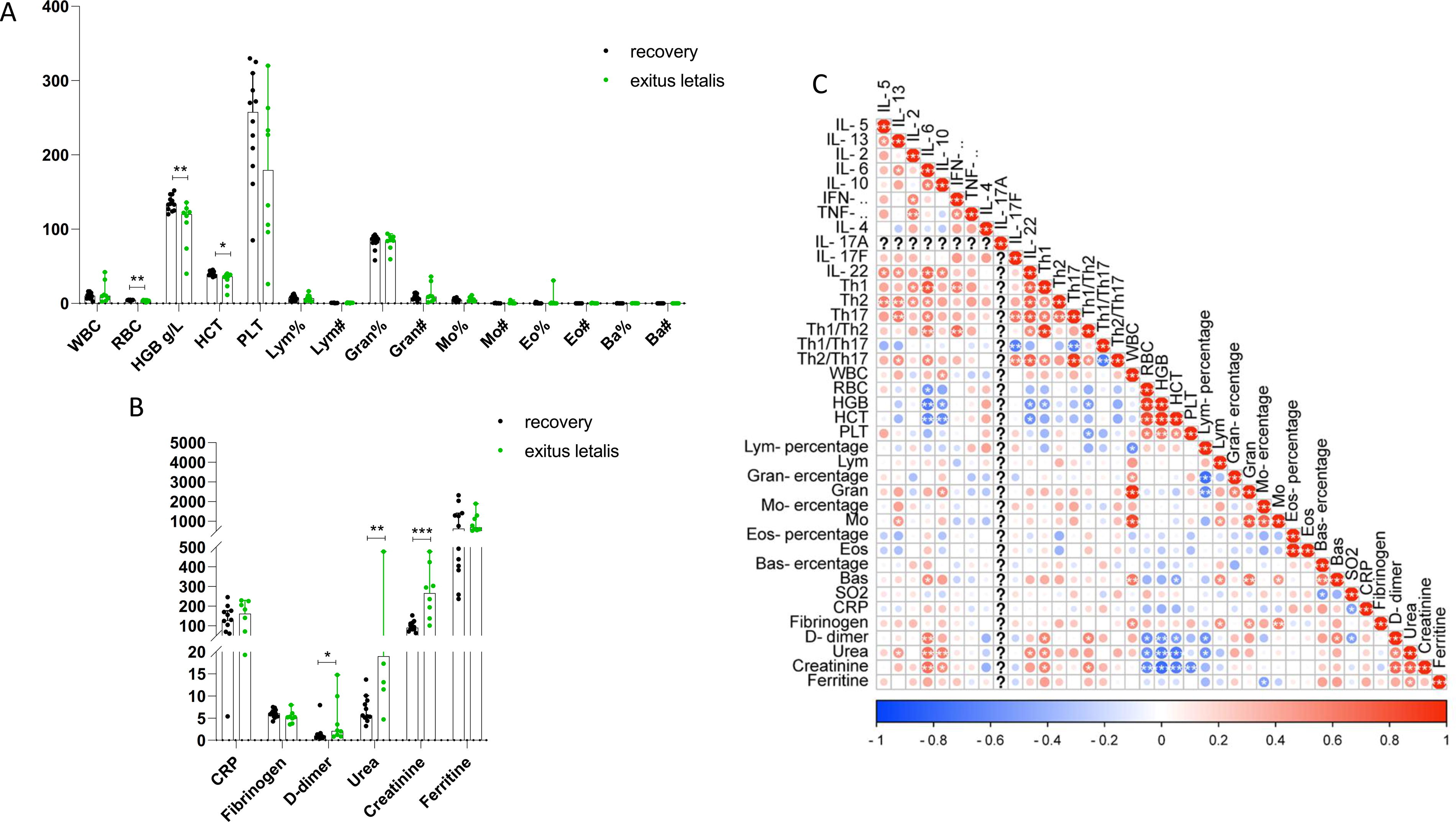
Evaluation of blood parameters in recovery and lethal cases of COVID-19.
Analysis of lymphocyte populations in COVID-19 patients
We investigated the lymphocyte populations in COVID-19 patients to monitor the differences among the groups (Fig. 5). A significant decrease was found in the percentage of CD3+, CD3+CD8+, CD3+CD4+, and CD16+CD56+ cells comparing the mild versus severe COVID-19 patients (Fig. 5A). On the other hand, the percentage of CD3+, CD3+CD4+, and CD19+ cells was significantly decreased in severe cases with recovery compared to lethal cases (Fig. 5B).
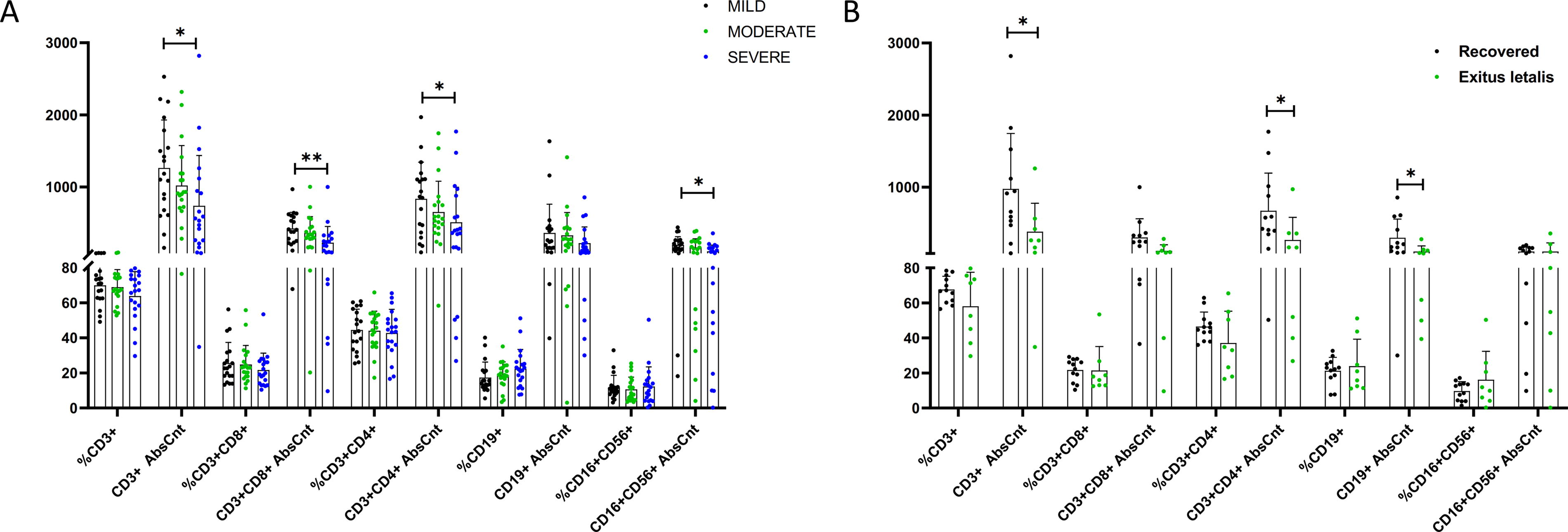
Evaluation of different lymphocyte populations in COVID-19 patients with mild, moderate, and severe disease
Discussion
The findings of this study contribute significantly to our understanding of the intricate immune and hematological dynamics in COVID-19 patients with varying disease severities (Arunachalam et al., 2020; Conti et al., 2020; Xu et al., 2023). The observed upregulation of IL12A in moderate cases suggests a potential role in orchestrating an effective immune response during this phase of the disease. IL12A, known for its involvement in the activation of T cells and natural killer cells, may play a crucial role in mounting an initial defense against the virus, possibly influencing the trajectory of the disease. This upregulation aligns with previous studies implicating the importance of a robust immune response in combating SARS-CoV-2 (Martonik et al., 2023; Zhou et al., 2020).
Conversely, the significant downregulation of IL23A, TNFA, IL1B, and IFNG mRNA levels in severe cases underscores a dysregulated immune environment characterized by a diminished pro-inflammatory response. This muted cytokine profile in severe cases may contribute to the excessive viral replication and impaired clearance observed in critically ill patients. The upregulation of the immunosuppressive cytokine IL10 in severe cases further supports the notion of an immune evasion strategy employed by the virus, potentially hindering effective antiviral immune responses and contributing to the progression of severe disease.
The serum cytokine profile revealed a striking increase in IL-6 and IL-10 levels in both moderate and severe cases, implicating their potential as reliable markers for disease severity. IL-6, a well-known marker of inflammation, has been previously associated with cytokine storm and adverse outcomes in COVID-19 (Aziz et al., 2020; Conti et al., 2020). The concurrent increase in IL10 adds a layer of complexity, suggesting a potential interplay between pro-inflammatory and anti-inflammatory signals.
Interestingly, no significant differences in serum cytokine levels were identified between recovery and lethal cases, challenging the notion that cytokine dysregulation alone dictates disease outcomes. This finding suggests that factors beyond cytokine levels, such as host factors, viral load, and the overall immune competence of the individual, may play pivotal roles in determining the clinical course of the disease. The lack of discernible differences in serum cytokines between recovery and lethal cases underscores the complexity of COVID-19 pathophysiology and the need for a multifaceted approach to understanding disease progression.
Hematological alterations in moderate and severe cases compared to mild cases provide additional insights into the systemic impact of SARS-CoV-2 infection. The decrease in HCT and lymphocyte count, coupled with an increase in granulocytes, aligns with the observed cytokine dysregulation and suggests a systemic inflammatory response. These hematological changes may contribute to the clinical manifestations of moderate and severe COVID-19, including respiratory distress and other organ complications.
In lethal cases, the lower levels of HGB and HCT, along with elevated D-dimer, urea, and creatinine, paint a picture of widespread organ dysfunction. The correlation of these parameters with IL6 and IL10 indicates a potential link between cytokine dysregulation and organ damage. The elevation of D-dimer suggests a prothrombotic state, consistent with reports of coagulopathy in severe COVID-19 cases. The association with urea and creatinine levels further implies renal involvement, highlighting the multi-organ impact of the disease in lethal cases.
While the study provides valuable insights, several questions and avenues for further research emerge. First and foremost, the molecular mechanisms underlying the observed cytokine dysregulation need to be elucidated. Understanding how SARS-CoV-2 manipulates the host immune response and triggers specific cytokine patterns is essential for developing targeted therapies. Additionally, the study’s focus on moderate and severe cases prompts consideration of early intervention strategies. Exploring whether interventions aimed at modulating the identified cytokine imbalances in the early stages of infection can alter disease outcomes would be a logical next step.
Furthermore, the lack of differences in serum cytokines between recovery and lethal cases warrants investigation into alternative markers or factors that may contribute to disease prognosis. Host genetic factors, viral genomic variations, and the presence of comorbidities could influence the disease course independently of cytokine levels and merit thorough exploration. Integrating comprehensive clinical data, including demographics, comorbidities, and treatment regimens, would enhance our ability to discern the multifactorial determinants of COVID-19 outcomes.
In conclusion, this study enhances our understanding of the complex interplay between the immune system, hematological parameters, and clinical outcomes in COVID-19 patients. The identified cytokine signatures, both at the transcriptomic and serum levels, provide potential targets for therapeutic interventions and prognostic assessments. However, the multifaceted nature of COVID-19 pathophysiology requires a holistic approach, considering host factors, viral characteristics, and treatment strategies. As the global scientific community continues to unravel the intricacies of SARS-CoV-2 infection, studies like this contribute crucial pieces to the puzzle, guiding the development of more effective diagnostic tools and targeted therapeutic interventions for individuals across the spectrum of COVID-19 severity.
Footnotes
Authors’ Contributions
A.I.T., F.N. and P.F.: Conceptualization. N.R.R., M.C.P. and P.F.: Data curation N.R.R. and N.M.: Formal analysis S.L.B., Y.V.D., N.M., and E, V.E.-F.: Investigation. S.L.B., Y.V.D., E.V.E.-F., F.N. and P.F.: Methodology. F.N.: Project administration A.I.T. and F.N.: Supervision J.F.M.-V.: Validation P.F.: Visualization N.R.R., S.L.B., and N.M.: Writing—original draft. A.I.T., J.F.M.-V., M.C.P., P.C., F.N., and P.F.: Writing—review and editing.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the Bulgarian Academy of Sciences.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon reasonable request to the Corresponding Author.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
The work was supported by the European Fund for regional development through Operational Program Science and Education for Smart Growth 2014–2020, Grant BG05M2OP001-1.002-0001-C04 “Fundamental Translational and Clinical Investigations on Infections and Immunity”, Bulgaria.