
Abstract
Membranous nephropathy (MN) is an autoimmune disease that is caused by the production of autoantibody against glomerular podocyte antigens by immune cells due to the lack of self-tolerance mechanisms. Similar to many autoimmune diseases, the pathogenesis of MN is still vague and many experiments are being conducted to detect the antigens and genetic reasons for MN illness. Recently, new antigens, such as exotosin 1/exotosin 2, neural EGF-like-1, semaphorin 3B, and protocadherin 7 have been identified in MN patients who did not have presence of antiphospholipase A2 receptor antigen. What is more, cytokines, which are molecules that regulate immune responses, have been found to have harmful effects in various autoimmune diseases, including multiple sclerosis, rheumatoid arthritis, systemic lupus erythematosus, and MN. The role of cytokines and treatment strategies in MN patients is discussed in this article. As the understanding of the disease improves, targeted therapies that focus on specific antigens or cytokines may be developed to effectively manage MN.
Introduction
Membranous nephropathy (MN), a prevalent and developing glomerular condition, is responsible for about one-quarter of cases of adult nephrotic syndrome. More than 75% of instances of idiopathic MN (IMN), sometimes referred to as MN, have an unknown cause (Zhao et al., 2022). Currently, MN is divided into two categories: primary, which is frequently brought on by the presence of antiphospholipase A2 receptor (PLA2R) autoantibodies, and secondary, which is brought on by malignancy, infection, medicine, or autoimmune disease. The distinct renal pathological features of MN consist of the enlargement of capillary walls within the glomeruli and the presence of immune complexes in the membrane located on the side (Tomas et al., 2014). In other words, the IgG deposition of complement components on the glomeruli capillary wall characterizes MN. MN is thought to be an autoimmune disease that mostly affects the kidneys. Few details are known concerning immunological dysregulation in MN, despite the fact that the majority of autoimmune illnesses are linked to a pro-inflammatory Th17-immune response. An autoimmune reaction that results in renal damage is the primary factor in the development and progression of the disease. This happens when immune complexes are created as a result of autoantibodies in the blood binding to particular antigens on podocytes. Then, under the glomerular epithelium, these complexes accumulate, harming and impairing the podocytes. As a result, the filtration barrier deteriorates, which causes a large amino acid loss in the urine.
The identification of autoantigens such as PLA2R1, which is responsible for about 70%–80% of primary MN (pMN) cases and THSD7A has expanded our knowledge of the disease, now commonly known as pMN. Currently, four new antigens have been identified in pMN including exotosin 1 (EXT1)–and exotosin 2 (EXT2)–associated MN, neural EGF-like-1 (NELL-1)-associated MN, semaphorin 3B (SEMA3B)-associated MN, and protocadherin 7 (PCDH7)-associated MN. The shift in perspective of pMN, from focusing on the study of tissue structure to examining the underlying physiological processes and from using general treatments to specifically targeting the generation of antibodies, became possible due to the identification of anti-PLA2R and anti-THSD7A autoantibodies (Zhao et al., 2022). Scientists are constantly discovering new autoantigens associated with pMN, suggesting that the disease is likely caused by a similar mechanism involving various autoantigens. The ability of human IgG4 antibodies against the human PLA2R1 or THSD7A to cause MN is currently unknown. Regarding the complement system, the plasma levels of C3a, C5a, C4d, Bb, and C5b-9 in MN patients were found to be significantly higher than those in healthy controls, although none of these indicators was associated with treatment response or renal prognosis in these patients (Zhang et al., 2019b). There was no difference in plasma complement protein levels between individuals with PLA2R1-positive MN and those with PLA2R1-antibody-negative MN.
About immunological dysregulation in MN, very little is known. Th1 cells often respond to intracellular infections by secreting Interferon (IFN)-γ, whereas Th2 cells are stimulated by parasites or allergens and release Interleukin (IL)-4 and IL-5. A pro-inflammatory immune system known as the Th17-immune response is linked to autoimmune disorders (Tomas et al., 2014). To differentiate, Th17 cells need particular cytokines, such as transforming growth factor-b (TGF-b) in combination with IL-6 or IL-21 (Zhao et al., 2021). IL-17A, IL-17F, IL-21, and IL-22 are among the cytokines secreted by Th17 cells that attract and activate neutrophils and macrophages to fight external pathogens or facilitate the onset of autoimmune disorders (Kimura and Kishimoto, 2011). The use of immunosuppressive medications like rituximab has been justified by the identification of pMN as an antibody-mediated autoimmune illness. As summarized in Table 1, rituximab has been proven safe and effective as the initial treatment for pMN, with remission achieved in 60%–80% of patients. The change in the T- and B-cell population in circulation has drawn interest in this setting. The proliferation and development of autoreactive B cells are facilitated by an aberrant rise in T follicular helper (TFH) cells and B cells are helped to finish somatic hypermutation in the germinal center, which urges the differentiation of B cells into plasma cells that generate IgG4 antibodies. This review will primarily focus on the immunopathogenesis of MN and the crucial role of cytokines in the underlying pathological processes, in order to gain a better understanding of the inflammation and immune-related mechanisms involved.
Clinical Trials of Rituximab in Membranous Nephropathy
Antigens in MN
The main challenge in diagnosing MN lies in differentiating between IMN and secondary MN, especially when considering MN associated with malignancy in patients. In this section, our objective is to provide a summary of the antigens involved in the development of MN, categorized into two groups: pMN and secondary MN.
Antigens in primary MN
Notably, in addition to PLA2R and THSD7A linked to MN, there is a growing consensus that MN is merely a recurrence of glomerular injury and that the MN associated with EXT1/EXT2, NELL-1, SEMA3B, and PCDH7 are distinct diseases with a similar harm characteristic of membranous. MN is classified as PLA2R-positive or PLA2R-negative MN depending on whether the kidney biopsy samples stained positively or negatively for PLA2R. Only a few specialist laboratories carry out THSD7A staining because THSD7A is incredibly uncommon. The seriousness of the disease is correlated with the detection of anti-PLA2R antibodies in patients with pMN. Several research approved the higher rate of proteinuria and nephritic-range proteinuria in MN patients with an aPLA2R-Ab+ than those with aPLA2R-Ab negative MN (Li et al., 2016). Although <50% of either main or secondary MN biopsy specimens are PLA2R negative, no additional antigens were found after 2014. Specific antigen-associated MN most likely represents unique diseases, each with a special clinical history, pathological results, and medical response. In recent research (Radice et al., 2018), three-quarters of IMN and ∼30% of patients with secondary MN (seven sufferers with malignancy) were positive for anti-PLA2R antibodies. The association between changes in aPLA2R titer and the activity of IMN is significant. It has been observed that a more rapid decline in aPLA2R titer is linked to shorter remission periods. In patients with IMN, immunological remission often precedes clinical remission. As the aPLA2R titer decreases over a few months, there is a notable reduction in proteinuria, leading to clinical remission. This suggests that monitoring the aPLA2R titer can serve as an informative marker for disease progression and treatment response in patients with IMN. According to a study, it was found that patients with low levels of anti-PLA2R exhibited the highest rates of spontaneous remission. On the other hand, patients with high levels of anti-PLA2R were more likely to experience persistent proteinuria and/or require immunosuppressive therapy (Timmermans et al., 2015). However, it is important to acknowledge that around 30% of patients with IMN exhibit negative aPLA2R, presenting a challenge in assessing their disease status and predicting outcomes without corresponding indicators. A noteworthy finding in the context of IMN is that the baseline levels of IL-35 have the potential to predict the duration of remission in patients, even in cases where aPLA2R is negative. In a study conducted by Zhang and the team (Zhang et al., 2019a), notable differences between patients with MN and cancer and those with IMN were revealed. Specifically, the rates of glomerular PLA2R and IgG4 depositions, as well as circulating anti-PLA2R antibodies, were significantly lower in MN patients with cancer. Additionally, MN patients with cancer exhibited distinct clinical characteristics, such as higher serum creatinine levels and lower estimated glomerular filtration rate (eGFR).
MN patients with anti-THSD7A showed end-stage kidney disorder, had undergone transplantation, and had an MN recurrence in the graft at an early stage. The allograft also showed evidence of THSD7A staining, pointing to the harmful function of anti-THSD7A antibodies (Tomas et al., 2016). Reviewing the literature reveals an intriguing finding that suggests a stronger association between THSD7A antigens and their corresponding antibodies with neoplastic conditions, compared to the weaker association observed between PLA2R antigen and anti-PLA2R antibodies; furthermore, studies have linked secondary MN, which is associated with anti-THSD7A, to proliferative disorders such as colorectal tumor and gallbladder tumor (Smarz-Widelska et al., 2022). However, according to multiple studies, the reported occurrence of THSD7A staining in kidney tissue with pMN ranged from 1.6% to 9.1% (Zhang et al., 2018). The case report detailed an intriguing instance of a patient with non-small cell lung cancer who developed MN subsequent to treatment with tislelizumab, a Programmed Cell Death-1 (PD-1) inhibitor (Chen et al., 2021). Notably, this patient exhibited a positive test result for THSD7A antibodies, a rare occurrence that has been shown to have a significant impact on the development of secondary MN. Leeaphorn et al. conducted the inaugural systematic review and meta-analysis on cancer prevalence among patients with MN, establishing a strong correlation with a prevalence rate of 10% (Leeaphorn et al., 2014).
Antigen in secondary membranous nephropathy
Typically, the presence of PLA2R in MN indicates pMN, whereas PLA2R negativity suggests secondary MN, although this occurs in a small proportion of patients, as most studies indicate that the majority of secondary MN cases are PLA2R-negative. For example, among the cases in a study, 6 out of 19 were diagnosed with Hepatitis B Virus (HBV)-associated MN (HBV-MN), of which 4 showed positive PLA2R on biopsy and 3 out of 4 cases tested had detectable circulating anti-PLA2R antibodies, indicating pMN. While the coexistence of viral infection may be coincidental, the possibility of viral infection potentially triggering the production of anti-PLA2R antibodies cannot be disregarded (Nikolopoulou et al., 2021). However, in the laser capture-coupled mass spectrometry cohort of PLA2R-negative MN, EXT1/EXT2 were the most prevalent specific proteins; these proteins are also found in secondary (autoimmune) MN (Sethi et al., 2019). Members of the exostosin glycosyltransferase family, EXT1 and EXT2, use chain elongation to contribute to the production of the heparan sulfate backbone. The other most frequent MN antigen found in the mass spectrometry was the NELL-1 protein, which was discovered after EXT1/EXT2 (Sethi et al., 2020a). SEMA3B was the third new antigen and it was both uncommon and distinct (Sethi et al., 2020b). The fourth most frequent novel protein in the MS/MS cohort of PLA2R-negative MN, is PCDH7, another novel antigen that was recently detected in patients with MN (Sethi et al., 2021). It is evident that more research and tests are required to identify the proteins or antigens that cause MN pathogens and learn more about the illness. The serum antibodies to PCDH7-associated MN, SEMA3B, and NELL-1 were found in a study by Sethi and colleagues. However, there was no report of finding anti-EXT1/EXT2 antibodies due to the probable target of antibodies to epitopes of EXT proteins that are truncated in serum and do not exist in the recombinant EXT proteins (Sethi, 2021). SEMA3B is mainly found in children under 2 years old and in young adults. In children, kidney biopsy samples often show IgG staining along the tubular basement membrane but these deposits do not test positive for SEMA3B. At present, putative antigens are the appropriate term to use for anti-EXT1/EXT2 antibodies. Neural cell adhesion molecule 1 (NCAM-1) has been identified as an antigen for membranous lupus nephritis (MLN) and pMN, in similar approaches of correlation between EXT1 and EXT2 with lupus nephritis. Patients with NCAM-1-associated MLN tend to be younger, mostly female, and have a history of lupus, which sets them apart from typical patients with MN. Nearly 7% and 2% of the MLN and pMN cases were linked to NCAM-1, respectively. However, more research is necessary to determine the clinical effects of anti-NCAM-1 antibodies. The neural cell adhesion protein which has been linked to proliferative lupus nephritis, is expressed at high levels in the central nervous system (Gu et al., 2021).
TGF beta receptor 3 (TGFBR3)-associated MN, similar to exostosin 1/2- and NCAM-1-associated MN, is prevalent in patients with MLN. TGFBR3 was concentrated in glomeruli and exhibited coimmunoprecipitation with IgG. Positive staining for TGFBR3 in glomerular immune deposits indicates a distinct form of MN that is enriched in MLN, prompting investigation for underlying autoimmune conditions. Mass spectrometric analysis revealed TGFBR3 as a unique type of MN, concentrated in glomeruli and valuable as IgG immune complexes from kidney biopsy tissue. Colocalization of TGFBR3 with IgG in glomerular immune deposits was observed. However, further research is needed to determine whether TGFBR3-associated MN is associated with other systemic lupus erythematosus (SLE) manifestations or has prognostic implications (Caza et al., 2023, 2021; Miller and Caza, 2023). Patients diagnosed with TGFBR3-associated MN typically have a background of autoimmune disease, with SLE being the most common diagnosis in 82% of cases during renal biopsy. Approximately 29.4% of these patients also exhibit a coexisting proliferative component. This condition primarily affects women around the age of 40. TGFBR3-associated MN shares clinical and histopathological similarities with MN forms associated with NCAM1 and EXT1/2 (Rossi et al., 2022).
Genetic in Membranous Nephropathy
There’s growing evidence that MN has a major hereditary component. MN shares a strong association with class II antigens of the human leukocyte antigen (HLA) system, which are encoded by particular alleles of the HLA-D locus on chromosome 6, much like the majority of autoimmune disorders. The majority of antigen-presenting cells, including B cells, monocytes, macrophages, dendritic cells, and Langerhans cells, carry HLA class II molecules, which control immune responses (Stanescu et al., 2011). They are linked to autoimmune disorders because they serve to introduce peptide antigens to the immune system. A genome-wide association study of three European cohorts, involving 556 white patients, demonstrated a substantial link between adult pMN and risk alleles in HLA-DQA1 (chromosome 6) and PLA2R1 (chromosome 2) (Stanescu et al., 2011). The risk of acquiring MN was shown to be strongly correlated with risk alleles of PLA2R1 and HLA-DQA1, as demonstrated in a large Chinese cohort comprising 1,112 patients with pMN and 1,020 healthy individuals39. Individuals who carried both risk alleles were >11 times more likely to develop MN. PLA2R antibodies were also linked with the presence of risk alleles.
Different HLA class II alleles associated with an elevated risk of MN were found in two studies using Chinese cohorts, indicating that HLA correlations may differ throughout ethnic groups (Cui et al., 2017; Le et al., 2017). In particular, DQA1*0501 in Europeans, DRB1*0301 in both races and DRB1*1501 in East Asians are substantial risk alleles. The strongest non-HLA signal that was found to be linked was the PLA2R1 gene. While DRB1*1501 is a high-risk allele for MN, DRB1*1502, which is merely one amino acid different, is not. On the other hand, DRB1*1502 indicates a decreased eGFR and an increased risk of renal failure when detected in conjunction with other HLA risk alleles. No genetic predisposition information is known for secondary MN or other antigens (Xie et al., 2020). Interaction between PLA2R1 and specific HLA alleles increases genetic susceptibility to MN (Table 2). After restriction, endonuclease fragment length polymorphisms, variable repeat sequences, and microsatellite polymorphisms, single nucleotide polymorphisms (SNPs) are the third generation of genetic markers, arising from single nucleotide differences in the DNA sequence. SNPs in the HLA-DQA1 region have a substantial effect on PMN in many racial groups. As a result, studies on PLA2R gene polymorphisms have been carried out in numerous nations.
Genetic Factors in MN
Cytokines in MN
To provide further clarity on the role of cytokines in the pathogenesis of MN, our objective is to categorize it into two sections: cytokines in pMN based on anti-PLA2R, and cytokines in MN without anti-PLA2R. It is important to note that the available data for both sections, particularly the second group, are significantly limited and should not be overlooked. As mentioned earlier, secondary MN is associated with viral infections or malignancies. Consequently, the cytokine profiles may vary between different diseases, underscoring the need to address the dearth of studies in this specific area.
Cytokines in pMN
A soluble form of the IL-6R can be found in the blood of patients with pMN. Despite the majority of soluble cytokine and growth factor receptors, the sIL-6R can activate gp130 on cells (trans-signaling pathway) that do not express the membrane-bound IL-6R by binding to it and activating it, thereby initiating signaling (Scheller and Rose-John, 2006). It is possible that the importance of IL-6 in pMN has been grossly overestimated. IL-6 (Fig. 1) has been identified as a promising target for therapeutic intervention in multiple autoimmune diseases. A recombinant monoclonal antibody called tocilizumab, which has murine variable and human IgG1 domain binds to IL-6 receptors that are both membrane-bound and soluble, inhibiting the signal transduction that IL-6 causes and has demonstrated effective medicinal results in cases of MN caused by Castleman’s illness (Zhao et al., 2022). The dual role it plays in B-cell activation, expansion, and differentiation helps to explain this conundrum. Additionally, IL-10 causes the growth of mesangial cells and impairs glomerular function. Impaired cell-mediated immunity in IMN is likely related to the up or down-regulation of IL10 and IL2, respectively (Sinuani et al., 2013). Higher circulating IL-35 levels (which is an IL-12 family member), in patients predicted clinical remission in MN (Roccatello et al., 2016) which may be related to enhanced Treg cells. Serum IL-35 levels increase post-treatment, and baseline levels in patients with available serum antibodies against anti-PLA2R predict the time course of the response, making IL-35 an overall biomarker (Zhang et al., 2022). In other words, indicators commonly used in IMN patients, such as aPLA2R, primarily focus on those with positive aPLA2R, leaving a challenge in assessing disease status and predicting outcomes for the nearly 30% of IMN patients with negative aPLA2R. However, the baseline levels of IL-35 have shown promise in predicting the remission time of patients, even in cases where aPLA2R is negative (Zhang et al., 2022). These findings suggest that IL-35 could serve as a valuable biomarker in assessing disease prognosis and predicting the duration of remission in IMN patients, regardless of aPLA2R status. By incorporating IL-35 measurements into clinical assessments, healthcare professionals may be able to better monitor and manage the disease progression of IMN patients with negative aPLA2R, leading to more personalized treatment strategies and improved patient outcomes.
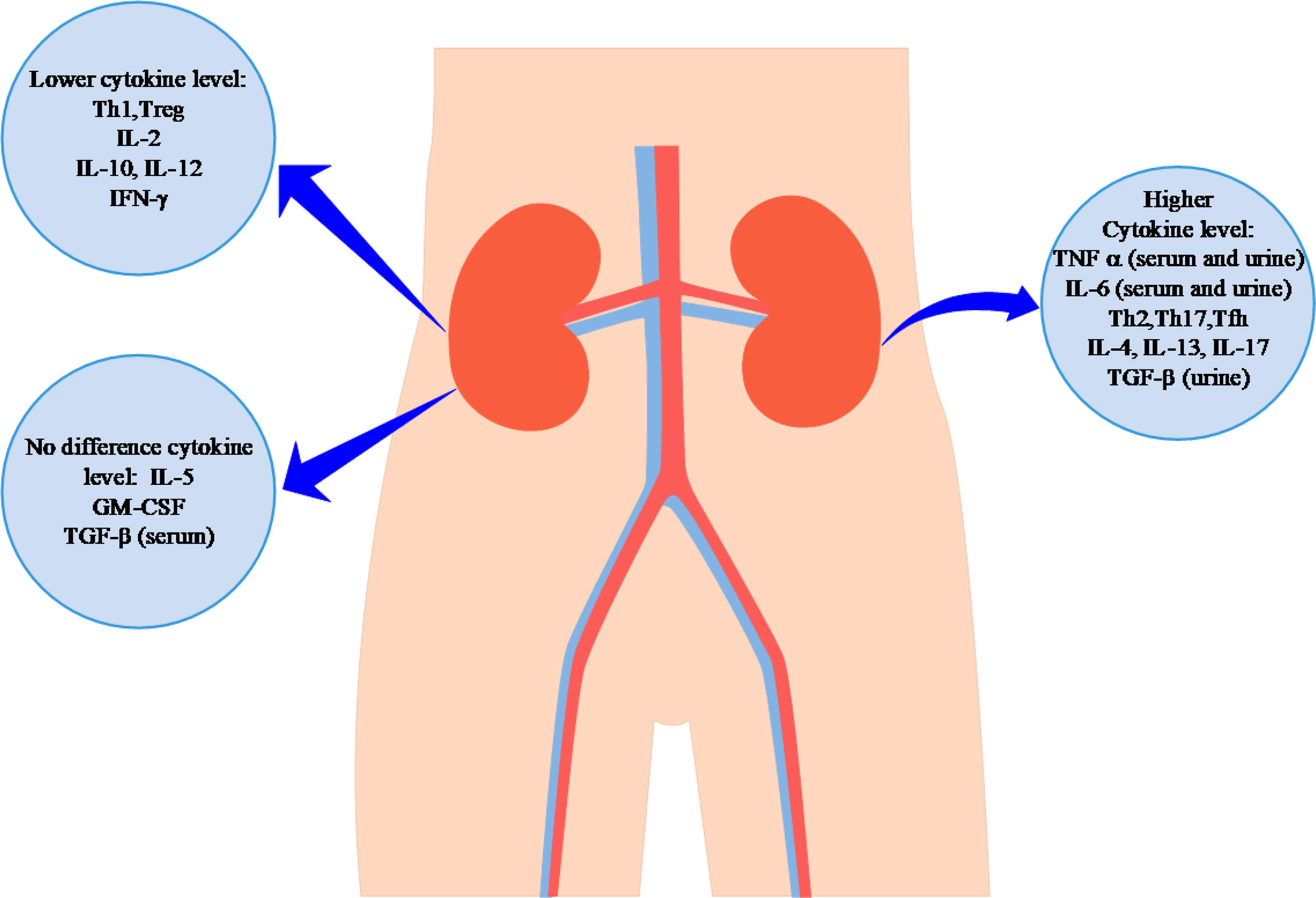
The level of cytokines in MN. TNF-α and IL-6 are higher in both serum and urine of patients with MN. Regarding serum, the expression levels of IL-4/IL-13 and IL-17 are higher and considered the most significant cytokines in MN pathogenesis. In addition, Th2, Th17, and TFH are higher in patients with MN than normal individuals. In contrast, the levels of IL-2, IL-10, IL-12, and IFN-γ are evaluated lower. Th1 and Treg cells which are considered immune response regulation, are lower in autoimmune diseases. Also, some studies report contradictory results of cytokines levels in MN, such as IL-5, Granulocyte-macrophage colony-stimulating factor, and TGF-β in serum. MN, membranous nephropathy; TGF-β, transforming growth factor-β; TNF-α, tumor necrosis factor-α; IFN-γ, interferon-γ.
A recent study found that TFH cells, naive B cells, and plasma cells significantly increased in number in IMN patients, raising the possibility that the frequency of these cells may be correlated with the advancement of histopathological manifestations (Zhang et al., 2017). When compared to healthy controls, IMN patients had significantly higher serum levels of IL-2, IL-4, IL-10, IL-17A, and IFN-γ. Evidently, Th1 cells play a key role in the inflammation response through two main cytokines; IL-2 and IFN-γ. Compared to healthy individuals, two research detected the peripheral blood mononuclear cells and lymphocytes in MN, and significantly fewer IL-2+ CD4+ cells production after stimulation (Hinoshita et al., 1990; Hirayama et al., 2002). There was no indication of a connection between the concentration of IL21 in the serum and the development of IMN but there was a direct correlation between the intracellular IL-21 of TFH cells (CD4CXCR5IL21+) and IMN (Shi et al., 2016). The reasonable explanation for the aforementioned finding is that CD4+ T cells and NKT cells, in addition to TFH, were probably involved in the production of IL-21 in serum. B lymphocyte and regulatory T-cell percentages have been shown to be considerably greater and lower in IMN cases than in the control group, respectively.
The interaction between BAFF (or BLyS) and a proliferation-inducing ligand (APRIL) to connect to particular receptors on naive or memory B cells is crucial for B cell survival. The detrimental effects of BAFF and APRIL on antibody-mediated autoimmune diseases are principally observed in their support for the survival of long-lived plasma cells and stimulation of antibody synthesis. In contrast to MN patients without anti-PLA2R, Netti and colleagues found that MN patients with anti-PLA2R first displayed noticeably higher levels of BAFF and APRIL (Netti et al., 2019). These findings were further validated by two studies, which demonstrated that MN patients without anti-PLA2R antibodies also lacked anti-THSD7A antibodies. This shows that, despite immune deposits being present in the glomerular basement membrane, the reduced levels of B cell cytokines in these patients were likely caused by the absence of circulating antibodies (Han et al., 2018; Oniszczuk et al., 2021). However, not only should the absence of research evaluating the relationship between BAFF and APRIL and antibody levels in MN not be disregarded but the results of various treatment strategies are also unknown. Evaluating the effect of monoclonal antibody against BAFF; Belimumab, in patients with MN was conducted and showed full or partial responses among nine patients as well as a completed response within 2 years of treatment and follow-up (Barrett et al., 2020).
TGF- β and IL-6 work together to promote Th17 differentiation, inflammation, and autoimmune disease. IL-17 is mainly produced by Th17 and can encourage the release of chemokines or other mediators. Kidney injury may be mediated by local IL-17, which also fosters the local inflammatory response. Recent research has also revealed the impacts of IL-17 on the immunological microenvironment through the promotion of tertiary lymphoid organs (Luo et al., 2021). Regarding TGF-β, it has been revealed that involvement in tissue damage at an early, promotes tissue fibrosis, and also engages in chemotactic leukocyte infiltration through the Smad signaling approach (Prud’Homme, 2007). TGF-1 levels in the urine of patients with MN are greater, and podocyte synthesis of TGF-1 has been linked to membrane thickening (Kim et al., 1999; Senatorski et al., 1998).
Cytokine in secondary membranous nephropathy
Recent research has provided increasing evidence linking secondary MN to malignancies, viral infections, and drug toxicity. However, the identification of the associated antigens in this type of MN is more feasible compared to pMN, and notably, the role of cytokines and their signaling pathways has been largely overlooked. Data regarding the specific cytokines involved in MN associated with other factors are limited compared to pMN. Important immunological mediators known as cytokines stimulate and polarize the immune response to provide host defense and restore homeostasis. The STAT6/JAK signaling pathway allows IL-4, the characteristic cytokine of T cells, to activate the synthesis of GATA3. In the signaling pathways of TH1 and TH2 cells, respectively, STAT4 and STAT6 are essential proteins. As prospective therapeutic targets for autoimmune disorders, they are also thought to exist. Additionally, some data have demonstrated that the major autoantibody in IMN is the TH2-related IgG4. Additionally, lupus nephritis, membranoproliferative glomerulonephritis, Henoch-Schonlein purpura nephritis, and IgA nephropathy were compared, and it was found that the IMN group had considerably less peripheral TH1/TH2 cells and a greater level of IL-4 and IL-13 cells. In addition, there was a substantial correlation between the amount of TH2 cells and urine proteins, indicating a potential involvement for TH2-derived IL4/IL-13 in podocyte destruction. No correlation between IL-4 and IgG levels was identified, despite the B cells being stimulated by the high amounts of TH2 cytokines to produce the TH2-related IgG subclass (IgG4). Regarding the expression of IL-4 and IL-13 genes in pMN, several studies have approved increasing levels. They are closely linked in terms of structure and function and have been thoroughly investigated in conditions such as inflammation, malignancy, and autoimmune disorders. Similar to IL-21 in patients with MN, which promotes B cell differentiation and improves antibody affinity formation, IL-4, and IL-13 not only can promote the function of B cells to generate antibodies (Zhang et al., 2017) but also can induce deposition of IgG by entering M2a type macrophages to the glomeruli of pMN (Fig. 2). IgG1, 2, and 3 are deposited in the pMN’s M2a region, which may encourage complement activation (Hu et al., 2021). In addition, earlier research found that pMN has higher levels of circulating M2 monocytes, which may be related to the early stages of antibody synthesis (Hou et al., 2018). This unforeseen outcome is substantiated by the IgG concentration dropping after urinary excretion (Masutani et al., 2004). In fact, alterations in IL-4 and IL-13 are not only found in pMN but also in patients affected by autoantibodies. Although the use of IL-4/STAT6 to treat diseases has been investigated (Oh et al., 2010), it may not be appropriate for pMN. IL-4 in pMN is regarded as a potent targeted therapy because of its pivotal role in the generation and class switching of antibodies. The investigation of IL-4 as a therapeutic target must wait until there has been more surveillance.
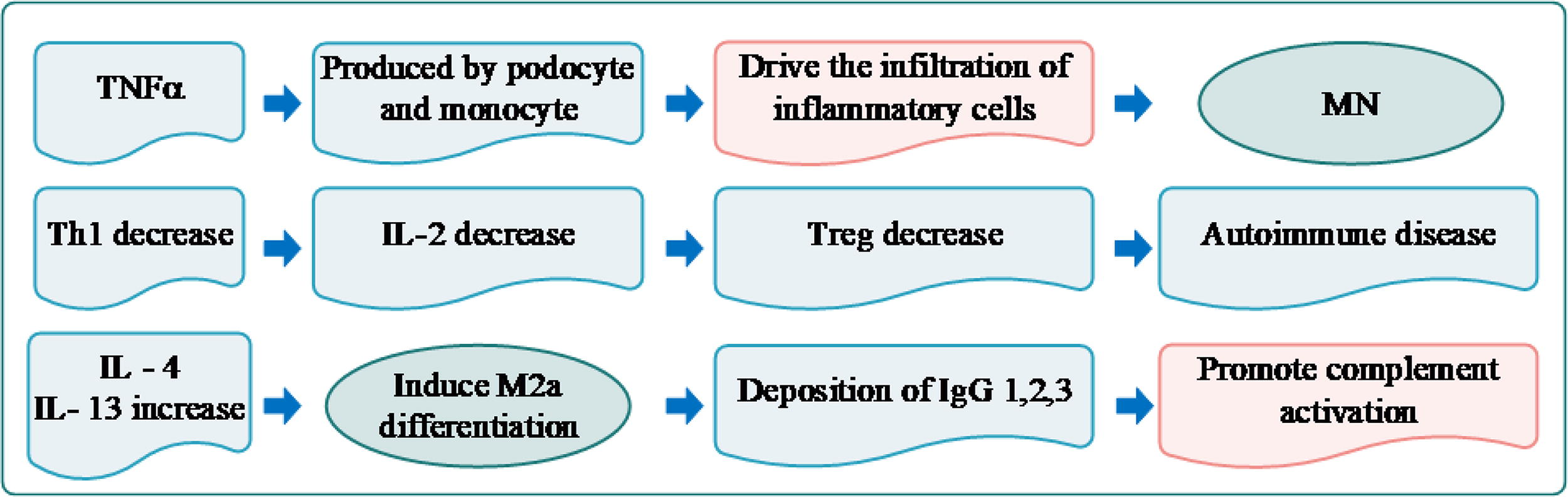
A schematic review of cytokines’ role in MN. Autoimmune diseases, such as MN, show declined release of Th1, consequently, its production, IL-2 which has a key role in the regulation of Treg cells is decreased leading to autoimmune responses. Regarding MN, podocytes and monocytes call the inflammatory cells attention by producing and releasing TNF-α. In addition, the complement system’s response is activated through macrophage differentiation, in particular, M2a after increasing IL-4 and IL-13. TNF-α, tumor necrosis factor-α.
Normal kidney function, which is unexpectedly boosted in IMN, is regulated and maintained in large part by IL10 and IL10-dependent signaling networks (Hirayama et al., 2002). The sources of IL-10 production vary from Th cell subsets, namely Th2, Th17, CD8+T cells, and B cell regulatory subsets (Breg). In rheumatoid arthritis patients the higher level of serum IL-10 is significant due to its ability to induce B cell proliferation and then, autoantibodies generations and inhibit IL-6 function in the acute phase. Br1 cells, a prominent Breg cell in pMN, were reported to be considerably higher compared to healthy individuals and nonimmune mediated patients with chronic renal disease by Chiara Cantarelli et al. (Cantarelli et al., 2020). Because IL-10 has deleterious effects in autoimmune diseases, such as SLE and MN, and can stimulate plasma cells to produce autoantibody, anti-IL-10 is considered a therapeutic application where IL-10 levels are positively connected with the severity of the disease (Motavalli et al., 2019).
Complement System
The complement system, particularly the terminal complement components C5b-9 (membrane-attack complex), plays a crucial role in the pathophysiology of MN (Teisseyre et al., 2023). Elevated urinary excretion of the C5b-9 complex has been observed in MN, and disease progression is associated with ongoing urinary loss. A recent case study by Seikrit et al. highlighted a patient with anti-PLA2R1-associated MN and antibodies against complement factor H, an important regulator of the alternative complement pathway (Seikrit et al., 2018). However, a subsequent study did not support the hypothesis that these antibodies contribute to the hyperactivation of the complement system in MN. In another study, it was found that around 3% of individuals with MN exhibit antibodies that specifically target the C-terminal recognition region of Factor H, impeding its binding to the surface (Zipfel et al., 2019). The lectin pathway is believed to be responsible for complement activation in MN since IgG4 is unable to activate the classical complement pathway but the exact mechanism of this activation remains speculative. In one study, researchers conducted a comprehensive analysis of complement activation pathways in patients with PLA2R1- and THSD7A-associated MN, and we also investigated the significance of such complement activation in a new antigen-specific autoimmune mouse model of MN (Seifert et al., 2023). Their findings revealed the activity of all three complement initiation pathways (alternative, classical, and lectin) in the studied patient cohort, suggesting that complement activation is not limited to a specific pathway in this disease. Interestingly, when examining paraffin-embedded tissue with antigen retrieval, we observed significantly higher rates of C1q positivity in patients with PLA2R1- and THSD7A-associated MN, indicating that C1q may be concealed within immune deposits in MN. However, contrasting results from other studies have challenged the notion that removing complement has an impact on proteinuria, thus raising questions about this pathophysiological concept.
The synthetic monoclonal antibodies Eculizumab, Ravulizumab, and eculizumab have demonstrated effectiveness in inhibiting the activation of the C5 protein, thus reducing cell damage caused by complement activation in the terminal complement pathway. However, the lack of documented clinical trials evaluating the use of these monoclonal antibodies in patients with MN raises concerns about their potential efficacy in treating this condition. Therefore, further research and clinical trials are necessary to determine the effectiveness and safety of these monoclonal antibodies in the management of MN. A valuable article provided a comprehensive review of the complement system’s role in MN and its potential as a therapeutic target (So et al., 2022).
Two trials are currently in progress to assess the effectiveness of two anticomplement medications in treating the condition. The first medication is called iptacopan and it is an extremely strong oral selective inhibitor of factor B, a crucial part of the alternative complement pathway (Caravaca-Fontán et al., 2023). Based on PLA2R antibody titers and proteinuria, this randomized, two-arm, parallel-group research will compare the effectiveness of iptacopan with RTX in participants at high risk of illness progression (NCT04154787). Narsoplimab, a humanized IgG4-λ monoclonal antibody, is the other agent. It works by blocking mannan-binding lectin serine protease 2, or MASP-2, a serine protease that cleaves the complement components C2 and C4. This medication is now being tested in patients with MN and other glomerular diseases in order to determine its safety (NCT02682407).
Membranous Nephropathy Treatment
As a child has MN, they might only need conservative therapy unless they are severely symptomatic. It is worth mentioning that complete remission from MN might take range between months and years because it is a condition that heals more slowly. Prior to starting therapy, patients with high anti-PLA2R antibody levels responded less well to treatment. Concentrations of antibodies against PLA2R are reliable indicators of how well a treatment will work. Patients with achieved remission or resistance to immunosuppressive therapy were detected with anti-THSD7A antibodies (Zaghrini et al., 2019). To date, only two medications have been shown to be effective in preventing end-stage renal disease and death: the alkylating agents cyclophosphamide and chlorambucil. The use of cyclophosphamide or chlorambucil, either alone or in combination with steroids, has demonstrated an increased rate of complete or partial remissions compared to supportive treatment or steroids alone (Perna et al., 2004). While half of MN cases do not react to steroids, Valentini et al. show in a short group of instances that the remaining cases did respond completely or partially (Valentini et al., 2009). Similarly, 11 MN adolescent patients had a steroid sensitivity of 6, a steroid dependence of 2, and a resistance of 3 (Arif et al., 2016). The assessment of using cyclophosphamide and chlorambucil as monotherapy in these patients is limited, indicating a lower effectiveness of this treatment approach. As alternatives for first-line therapies, tacrolimus (TAC) or cyclosporine (a calcineurin inhibitor) were suggested. A study discovered that corticosteroid and cyclophosphamide treatment was more successful at inducing remission than TAC and rituximab sequential treatment. The corticosteroid-cyclophosphamide group also saw remissions more quickly, with a noticeable difference in the number of remissions already at three months. Additionally, the majority of remissions in the corticosteroid-cyclophosphamide group were total, compared to the majority of partial remissions in the TAC-rituximab group (Fernández-Juárez et al., 2021). Meantime, the efficacy of the combination of TAC and corticosteroids was evaluated by Tian et al., which showed that the combination of TAC and corticosteroids was found to be effective in treating patients with MN within the first year, particularly in the initial 6 months. However, due to negative effects on the nephron with a high risk of striking hands, this therapy technique does not have any long-term benefits (Tian et al., 2022). Clinical remission at 24 months in the cyclophosphamide/glucocorticoid group was higher efficacy (84%) than patients who received TAC/rituximab (58%). Both groups experienced similar rates of serious adverse events. The cyclophosphamide/glucocorticoid group also had a significantly higher immunological response, with a greater depletion of anti-PLA2R1 antibodies at three and six months (77% and 92%, respectively) compared to the TAC/rituximab group (45% and 70%, respectively). In a study evaluating the combination of rituximab and cyclosporine compared with monotherapy, elucidated the therapeutic potential and immune response after 2 years (Ponticelli and Moroni, 2019; Waldman et al., 2016). In a multicenter study involving 122 MN patients with stable renal function who received TAC treatment, remission rates were observed to be 60%, 78%, and 84% after 6, 12, and 18 months of treatment, respectively (Caro et al., 2015). The study also found that lower levels of proteinuria at baseline were significantly associated with a higher likelihood of achieving remission, suggesting that TAC monotherapy is an effective and safe treatment option for MN patients with stable renal function. An important observation from a retrospective analysis of clinical data on 182 MN patients treated with TAC and followed up for at least 1 year is the relatively high rate of relapse (Liang et al., 2023). Specifically, out of the total patients, 154 (84.6%) experienced complete or partial remission, while 28 patients (15.4%) did not respond to the treatment.
However, there has been a tendency to start treating MN using more current treatments, such as the B-cell inhibitor drug rituximab. While multiple studies have highlighted the effectiveness of cyclophosphamide in the treatment of MN, particularly when used in combination therapy, a single study has indicated the superiority of rituximab over cyclophosphamide in terms of long-term efficacy (Oliva-Damaso and Bomback, 2021). Concerns about the negative effects of myelotoxicity, the elevated risk of cancer and infection, and the suppression of gonadal function brought on by alkylating drugs are the causes of this shift. The identification of autoantibodies against PLA2R and THSD7A has provided a logical basis for designing treatments to target B cell lineages to inhibit the differentiation into plasma cells, consequently inhibiting antibody production and the complement system’s function (Fig. 2). Additionally, this discovery offers a means to evaluate the effectiveness of treatment. Rituximab, an anti-CD20 monoclonal antibody, is generally considered safe and is successful in resolving proteinuria in approximately two-thirds of adults with MN. Rituximab has been used for primary/IMN in adults in a large number of smaller or observational studies. In the majority of patients receiving rituximab treatment, all investigations have shown a decline in proteinuria and a partial or complete remission of the disease (Safar-Boueri et al., 2021). Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment on an unprecedented scale, in particular hematological malignancies (Meftahpour et al., 2022). Some reports, however, explain the glomerulonephritis brought on by ICIs as immune-related adverse events. Interestingly, ICIs, as immunosuppressive, are considered MN treatment strategies, and further studies are required to evaluate the beneficial and drawbacks impacts of this treatment. It has already been proposed that rituximab inhibits Immune Checkpoint Inhibitor (ICI)-driven T-cell activation that upregulates autoreactive B cells while maintaining T-cell-mediated antitumor immunity (Lin et al., 2020). Rituximab is widely used in the treatment of MN in adults due to its high tolerability and low toxicity. Similarly, it has become the preferred choice over cyclophosphamide as the initial therapy for children with ANCA-associated vasculitis (Jariwala and Laxer, 2018). As a result, rituximab’s pharmacokinetics and safety statistics have been provided for the pediatric population. Rituximab enables partial or complete renal remission, opening the door to additional therapeutic approaches. Meanwhile, one study supported the prospect of targeting immune checkpoints, such as Cytotoxic T-lymphocyte associated protein-4, PD-1, T-cell immunoglobulin and mucin-domain containing-3, and Lymphocyte-activation gene 3, as MN treatment applications whose expression is compromised before treatment (Motavalli et al., 2023). Benyahia et al. showed that three of the six patients who received rituximab treatment experienced partial responses, and three of them fully recovered, strengthening the proof-of-concept for the drug’s continued efficacy even after exposure to ICI (Benyahia et al., 2023). Nivolumab’s antitumor effectiveness as well as maintaining kidney function in patients with malignant pleural mesothelioma and MN were both authorized by Lin and colleagues (Lin et al., 2020). Gauckler and colleagues approved that there is strong evidence in favor of using rituximab as an induction medication because it induces remission in roughly two-thirds of patients without the need for concurrent corticosteroid therapy (Gauckler et al., 2021). In general, Ruggenenti and the team summarized the efficacy of rituximab in MN patients (Ruggenenti et al., 2017). In in vitro, B-cell cytotoxicity with rituximab was far lower than anti-CD-20 mAB (Patz et al., 2011). These results suggest that obinutuzumab and ofatumumab are promising therapy options for MN patients. In the preliminary investigation, Sethi and colleagues administered obinutuzumab to 10 individuals with MN who had mostly not responded to rituximab treatment (Table 3). The results revealed that 90% of the patients experienced either partial or complete remission after receiving two doses of obinutuzumab. At the 6-month mark, 60% of the patients achieved complete or partial remission, which is a higher response rate compared to the 35% in the rituximab monotherapy study in patients with MN (Sethi et al., 2020c).
Therapeutic Applications in the Treatment of MN
Ongoing research is dedicated to identifying new therapeutic targets and investigating immunomodulatory approaches for the treatment of MN associated with anti-PLA2R antibodies. These advancements offer the potential for more individualized and efficient treatment strategies in the future. It is important to note that therapeutic applications for MN should not solely rely on PLA2R. Considering the significant role that the complement system and cytokines can play in the pathogenesis of MN, it is recommended to evaluate therapies involving complement system inhibitors or cytokine inhibitors. By targeting these additional factors, a more comprehensive and tailored approach to treatment can be pursued. However, other treatment strategies, such as plasma exchange, immunoabsorption, mycophenolate mofetil, adrenocorticotropic hormone, and bortezomib have shown promising results in MN sufferers. As mentioned above, the targeting complement system is being evaluated as a novel therapeutic application. Meantime, some drugs such as PL-2 (pegcetacoplan; Apellis Pharmaceuticals), eculizumab (Alexion), which target C5, and LNP023 (Novartis), which inhibits complement factor B are being evaluated in MN and give good results. However, it is urgent to further study and experiment in order to assess its safety as well as related adverse effects due to the lack of high-quality data (Reinhard et al., 2020).
Conclusion
MN as an autoimmune disease is determined by the deposition of IgG and complement components on the glomeruli capillary wall. The glomerular podocytes that express PLA2R, TSH7DA, and EXT1/EXT2 antigens are the ones that are specifically targeted by antibodies made by plasma cells. Autoantibodies against glomerular podocytes antigens and complement system activation are considered MN pathogenesis and, evidently, cytokines pave the way for immunological mechanisms. Therefore, focusing on the role of cytokines and their levels of expression in serum and urine is necessary to understand the pattern of immune response in MN. The prognosis of MN is influenced by a number of variables, including age, gender, comorbidities, treatment response, and disease severity. The more severe the disease, the worse the prognosis generally is. This includes the extent of organ damage or dysfunction and the overall impact on the patient’s health. The presence of other diseases or medical conditions can complicate the primary disease, making treatment more challenging and potentially worsening the prognosis. For example, diabetes or hypertension can affect kidney disease outcomes. How well a patient responds to treatment is a critical factor. Patients who respond positively to treatments typically have a better prognosis. This includes improvements in symptoms and markers of disease. Younger patients generally have better recovery prospects compared to older patients. Age can influence how the body copes with disease and responds to treatment. There can be gender-specific differences in disease progression and response to treatment, which can affect prognosis. Some diseases may affect one gender more severely than the other. In addition, proteinuria level, GFR, and serum creatinine level are monitoring methods to regularly check and evaluate the progress of a disease. Understanding these factors, monitoring methods, and prognostic markers helps healthcare providers predict the course of the disease, tailor treatments, and manage patient care more effectively.
Although our primary focus is on the role of cytokines in MN pathogenesis, it is also important to consider TGFβ. In relation to Th17 cell promotion and the activation of IL-17, which induces autoantibody production against podocytes, IL-6, myeloid suppressor cells, and TGFβ are key factors. IL-17 has an antagonistic relationship with Treg cells, leading to antibody production and attacks on podocytes. Local expression of IL-17 in the kidneys plays a significant role in causing kidney damage and enhancing local inflammation. IL-17 contributes to the inflammatory response within the kidney tissue, which can lead to injury and further deterioration of kidney function. Besides the interaction of TGFβ with IL-6, several reports suggest that Monocyte Chemoattractant Protein-1 (MCP-1) expression is associated with increased myofibroblast infiltration in MN, contributing to the progression of renal dysfunction (Li et al., 2020). During the pathogenesis of the immune complement system, TGFβ contributes to basement membrane thickening and abnormal expression in glomeruli and renal tubules. MCP-1 is known as an inflammatory biomarker for renal function progression in nephropathy, whereas Growth Differentiation Factor-15, part of the TGFβ superfamily, predicts pMN progression by indicating inflammation, fibrosis, and kidney damage (Ham et al., 2018; Liu et al., 2024). The other interleukin that serves as a potential biomarker for monitoring treatment response and predicting disease outcomes is IL-35 (Roccatello et al., 2016). Higher levels of circulating IL-35 are associated with clinical remission in patients with pMN undergoing treatment with rituximab. This is linked to an increase in Treg cells, which might play a role in enhancing the therapeutic response to the treatment. IL-4 and IL-13 play two distinct roles in MN pathogenesis: they contribute to antibody production by facilitating the differentiation and maturation of B cells, and they enhance the complement system through IgG deposition. In pMN, the glomeruli are infiltrated with M2a-type macrophages. The infiltration of M2a macrophages in pMN is associated with the deposition of IgG1, IgG2, and IgG3, which may promote complement activation (Hu et al., 2021). Although the treatment of IL-4/STAT6 in asthma has shown promising results in animal experiments, it may not be applicable to pMN. However, IL-4 in pMN is considered a potential therapeutic target due to its crucial role in antibody production and class switching. Further surveillance and research are necessary before fully exploring IL-4 as a therapeutic target in pMN (Oh et al., 2010; Simpson et al., 2020). As accurately summarized by Zhao et al. (Zhao et al., 2022), TNFα and IL-10 are not effective targets for therapy in pMN because they fail to reduce proteinuria and immune complexes, and IL-10 has a dual role in MN pathogenesis. Conversely, IL-6 (TCZ), low-dose IL-2 (to increase Treg cells), IL-4 (for class-switching), IL-4/IL-13 (though uncertain due to the lack of suitable animal models), and most notably, BAFF are promising targets for therapy in pMN (belimumab).
Footnotes
Authors’ Contributions
C.W.: Conceptualization, Language Review. C.L.: Methodology, Software. Z.H.: Supervision. R.F.: Validation.
Availability of Data and Materials
The datasets used in this study are available upon reasonable request.
Author Disclosure Statement
The author declares no competing interests, whether of a financial or personal nature, that could influence the research or its interpretation.
Funding Information
This work was supported by