
Abstract
This prospective study investigated the utility of baseline CXCL13 levels in predicting methotrexate response and monitoring disease activity in 50 treatment-naive early rheumatoid arthritis (RA) patients (2010 American College of Rheumatology/European League Against Rheumatism criteria) treated with methotrexate. Participants were categorized into methotrexate responders (MTX-R, n = 29) and nonresponders (MTX-NR, n = 21) at 12 weeks. Baseline CXCL13 levels were significantly higher in MTX-R compared with MTX-NR (P = 0.035). Receiver operating characteristic curve analysis identified a baseline CXCL13 cutoff of >100 pg/mL for predicting methotrexate response, with 69% sensitivity, 52% specificity, and 62% accuracy. Posttreatment, CXCL13 levels decreased significantly in MTX-R (P < 0.001) but remained unchanged in MTX-NR. Disease activity parameters (eg, DAS-28) correlated with CXCL13 dynamics, though specific coefficients were not detailed. The study highlights CXCL13 as a potential biomarker for stratifying methotrexate therapy, with higher baseline levels favoring therapeutic response and posttreatment reductions reflecting clinical improvement. While moderate diagnostic accuracy limits standalone use, CXCL13 may complement existing tools to guide early personalized treatment. Further validation in larger cohorts is warranted to confirm its role in optimizing RA management.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory disease characterized by inflammation, persistent synovitis, progressive joint destruction, and extraarticular manifestations. Most of the recent guidelines for the management of RA, including the American College of Rheumatology (ACR) 2015 and European League against Rheumatism (EULAR) 2016 guidelines, recommend disease-modifying antirheumatic drugs (DMARD) monotherapy, preferably methotrexate, over DMARD combination therapy as the first-line treatment in treatment-naive (no prior use of DMARDs or corticosteroids) RA (Singh et al., 2016; Smolen et al., 2017).
However, as shown by different studies, only about one-third of RA patients will respond to methotrexate monotherapy. The remaining two-thirds will require either a combination of conventional synthetic DMARDs (csDMARD) or newer biological DMARDs (bDMARD) (Bakker et al., 2007; De Jong et al., 2014; Den Uyl et al., 2014; Grigor et al., 2004; Hazlewood et al., 2016; Möttönen et al., 1999; O’Dell et al., 2002). Hence, starting methotrexate monotherapy in all treatment-naive RA patients has the potential risk of missing the “window of opportunity” in two-thirds of them. So, the patients with inadequate response to methotrexate continue to have ongoing disease activity, pain, and reduced quality of life for at least 3–6 months until managed with a combination of csDMARDs or bDMARDs. Studies have shown that delay in controlling the inflammation and starting the accurate treatment can lead to bony erosions and joint damage as early as 3 months of disease onset (Steunebrink et al., 2018)(Finckh et al., 2006; Goekoop-Ruiterman et al., 2005; Korpela et al., 2004; Moreland et al., 2012; Saunders et al., 2008). Although high rheumatoid factor (RF) and anticitrullinated protein antibodies (ACPA) titers and early bony erosions are considered poor prognostic factors, they are not conclusively proven indicators to start combination DMARDs as the initial treatment. Hence, a biomarker to identify RA patients who may respond to methotrexate monotherapy will help to save precious time and can reduce the possible risk of joint damage and functional impairment due to the delay in initiating the optimal treatment.
CXCL13 (BCA-1, BLC) is a B cell-specific chemokine thought to play a vital role in the organization of extra-nodal lymphoid aggregate (Carlsen et al., 2004). The interaction of CXCL13 with CXCR5 promotes the process of lymphoid follicle and germinal center formation through the recruitment of naive B cells and follicular T cells (TFH) to the lymphoid follicle. Thus, CXCL13 produced locally represents the primary environment for ectopic B cell interaction with other cell subsets and also for local affinity maturation of the immunoglobulin gene (Shi et al., 2001). The CXCL13–CXCR5 axis is critical to the generation of immunological memory based on long-lived plasma cells because the interaction between TFH and B cells is necessary for the formation of plasma cells and autoantibody production. Hence, CXCL13 is the key to the development of autoantibodies like IgG ACPAs and IgA-RF long before the development of clinical signs and symptoms (Humby et al., 2009). In addition to the development of autoantibodies in the preclinical phase, CXCL13 has been associated with synovial inflammation in RA, which can be detected on clinical examination as well as imaging (Bao et al., 2020; Li et al., 2022).
Researchers have observed 1.5 times higher serum levels of CXCL13 in patients with active disease than in quiescent disease (Rioja et al., 2008). It was established that there is a strong relationship between synovial CXCL13 mRNA expression and serum CXCL13 level in a cohort of patients with long-standing RA (Rosengren et al., 2011). Thus, synovial production appears to account for the increased serum CXCL13 level. Similarly, serum CXCL13 levels would reflect the impact of CXCL13 on synovial inflammation and the shaping of the clinical and serologic phenotype.
Researchers also observed that serum CXCL13 expression was much higher in seropositive than seronegative RA patients, which justifies the role of CXCL13 in the development of the autoantibodies (Jones et al., 2013). Baseline CXCL13 plasma levels were found to be increased in early RA patients in comparison with healthy volunteers (Rioja et al., 2008). However, the baseline CXCL13 was lower in established disease than in patients with early disease (Jones et al., 2013). In addition, CXCL13 expression is found to be upregulated by tumor necrosis factor-alpha (TNF-α) and by T cell receptor stimulation. Evaluations based on these observations indicated that baseline CXCL13 plasma levels in early RA have reflected the response to treatment in a drug-naive cohort treated with TNF-α inhibitors (TNFi). Baseline CXCL13 was thus established to be a biomarker of predictive power in patients treated with TNFi in the early disease phase (Greisen et al., 2014).
In light of these findings, we were curious about the role of CXCL13 in determining the therapeutic effect of methotrexate, the anchor drug in the treatment of early RA. To our knowledge, no studies were conducted to establish the power of serum CXCL13 in predicting the response to treatment with methotrexate. We studied the relationship between serum CXCL13 and methotrexate in a treatment-naive, prospectively recruited cohort of patients with RA.
Materials and Methods
This was a prospective cohort study, conducted with approval from the institutional ethics committee (EC-AIMS-2017-RUMAT-217), at a quaternary care center in South India. All consecutive patients who attended the Department of Rheumatology and Clinical Immunology with RA, diagnosed as per ACR/EULAR 2010 classification criteria for RA, were screened (Kay and Upchurch, 2012). The patients who were treatment-naive and aged over 18 years of age were invited to participate in the study. We obtained written informed consent from all participants before inclusion. Participant recruitment began on January 1, 2017, and concluded on August 31, 2018.
At baseline, a complete medical history and treatment history were recorded. Patient global assessment, physician global assessment, blood workup, serological assessment, and disease activity assessments like disease activity scores (DAS) 28 erythrocyte sedimentation rate (ESR)/C-reactive protein (CRP), simplified disease activity index (SDAI), and clinical disease activity index (CDAI). SDAI and CDAI were done at baseline and at a 12th week follow-up. Seronegative patients were further evaluated for the evolution of the disease during the study duration and were excluded if they were fulfilling an alternative diagnosis. As per international guidelines, methotrexate was initiated at the first visit itself at a dose of 10 mg weekly once dosing, and it was slowly escalated to a best-tolerated dose with a maximum of 25 mg/week (Bello et al., 2017; Pavy et al., 2006). Folic acid supplementation was given to all patients to improve tolerability by reducing gastrointestinal and hepatic adverse events (Shea et al., 2013). Low-dose glucocorticoids were initiated at baseline as a bridge therapy for all patients at the lowest dose and were tapered off in the shortest duration (Fraenkel et al., 2021). Monthly assessment of disease activity was done for all patients, and drug titrations were made. As per the EULAR response criteria for RA, we categorized participants into methotrexate responders (MTX-R) and nonresponders (MTX-NR) at the end of a 3-month follow-up (van Gestel et al., 1996).
Based on the mean and standard deviation of CXCL13 from a previous publication (Greisen et al., 2014), with 95% confidence and 80% power, a minimum sample size of 24 in each group was estimated.
The blood taken for CXCL13 enzyme-linked immunosorbent assay (ELISA) evaluation was stored at −80°C until the sample size was achieved and was evaluated together at the end of the study duration. Serum CXCL13 levels were quantified according to the manufacturer’s instructions using a commercially available sandwich ELISA kit (Quantikine human CXCL13/BCL/BCA-1, #DCX130 R&D Systems, Minneapolis, MN, USA). All samples were diluted 1:2 in Calibrator Diluent RD6-41 supplemented with mouse and bovine IgG to ensure preaggregation of heterophilic antibodies. Samples were analyzed in duplicates, and the minimum detection limit (cutoff) was calculated as two standard deviations of the blanks. Values below the cutoff value were assigned the same value as the cutoff. The ELISA kit was validated as previously described by Greisen et al. (2014).
Statistical analysis was performed using IBM SPSS version 20.0 software 10. Categorical variables are expressed by frequency and percentage. Continuous variables are presented using mean ± standard deviation. Receiver operating characteristic (ROC) curve analysis was used to find the cutoff value of CXCL13 with the response to the treatment. To test the statistical significance of the association of the CXCL13 cutoff value with the response, Pearson’s χ2 test was used. Diagnostic measures such as sensitivity, specificity, and accuracy were calculated. Pearson correlation/Spearman Rank correlation method was used to test the relationship of core set variables with CXCL 13 values. To test the statistical significance of the mean difference of different variables between MTX-R and MTX-NR groups, Student’s t-test/Mann–Whitney U test was used. To test the statistical significance of the mean difference of different variables pre- and post- within MTX-R and MTX-NR groups, Wilcoxon signed-rank test was used.
Results
Baseline characteristics
A total of 72 patients were enrolled in the study. Ten patients were removed as they were on alternative therapy during or before the initiation of treatment, intolerant to MTX, or had an alternative diagnosis. Twelve patients were lost to follow-up after a natural calamity that occurred during the study period. Among the remaining 50 active participants of the study, 41 were females, and 9 were males. Four of the 50 patients were seronegative. Among the seropositive patients, 39 had both RF and ACPA positivity, 5 had only ACPA positivity, and 2 had only RF positivity. The mean age of the patients in the study was 52 ± 13 years. At baseline, 42 patients had high disease activity, and 8 patients had moderate disease activity as per DAS28 ESR score. The patients were divided into MTX-R and MTX-NR at the end of the study. With twenty-nine patients in the MTX-R group and twenty-one patients in the MTX-NR group, the baseline parameters were comparable among the two groups (Table 1).
Baseline Characteristics of the Participants Included in the Analysis, Categorized by Their Remission Status at the End of 12 Weeks of Methotrexate Monotherapy (N = 50)
Summary estimates are expressed in mean ± standard deviation.
CDAI, clinical disease activity index; DAS, disease activity score; MTX-NR, methotrexate nonresponders; MTX-R, methotrexate responders; SDAI, simplified disease activity index.
Baseline serum CXCL13 levels
The mean baseline CXCL13 level of the MTX-R group was higher than the MTX-NR group, which was statistically significant (P = 0.035) (Fig. 1). The correlation of baseline CXCL13 values with the various core set outcome variables in the determination of disease activity did not have a statistically significant difference between the MTX-R and MTX-NR groups. However, there was a negatively trending correlation between baseline CXCL13 values with the core set variables in the MTX-R group (Table 2).
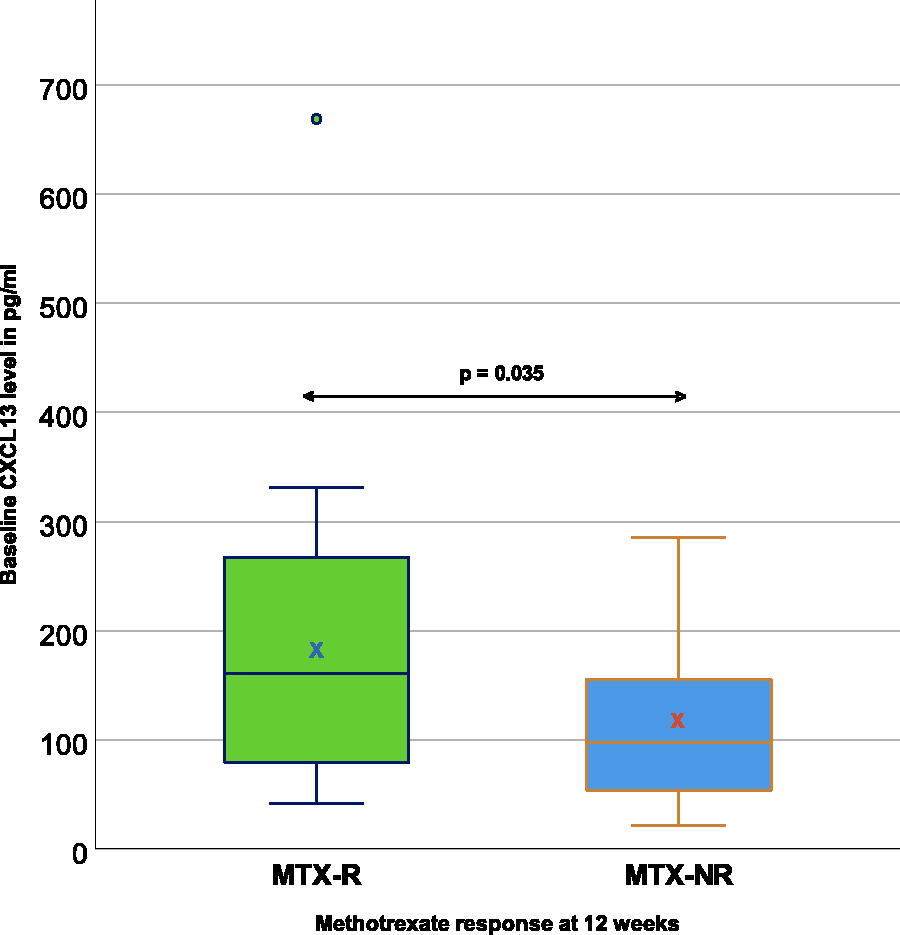
Box plot depicting the mean difference between the baseline CXCL13 levels of the methotrexate responders (MTX-R) and methotrexate nonresponders (MTX-NR) groups. The mean of CXCL13 values are marked in box with x.
Correlation of CXCL13 Levels with Core Variables and Disease Activity
Response of treatment with methotrexate on CXCL13
Mean CXCL13 levels in the MTX-R group reduced from 183.73 ± 130.6 pg/mL to 85.9 ± 48.33 pg/mL at the end of the third month; however, the MTX-NR group CXCL13 value reduced from 116.81 ± 80.69 pg/mL to 101.82 ± 81.33 pg/mL at the end of 3 months of treatment (Fig. 2). The difference in the CXCL13 value in the MTX-R group was found to be statistically significant (P < 0.001) in contrast to the MTX-NR group.
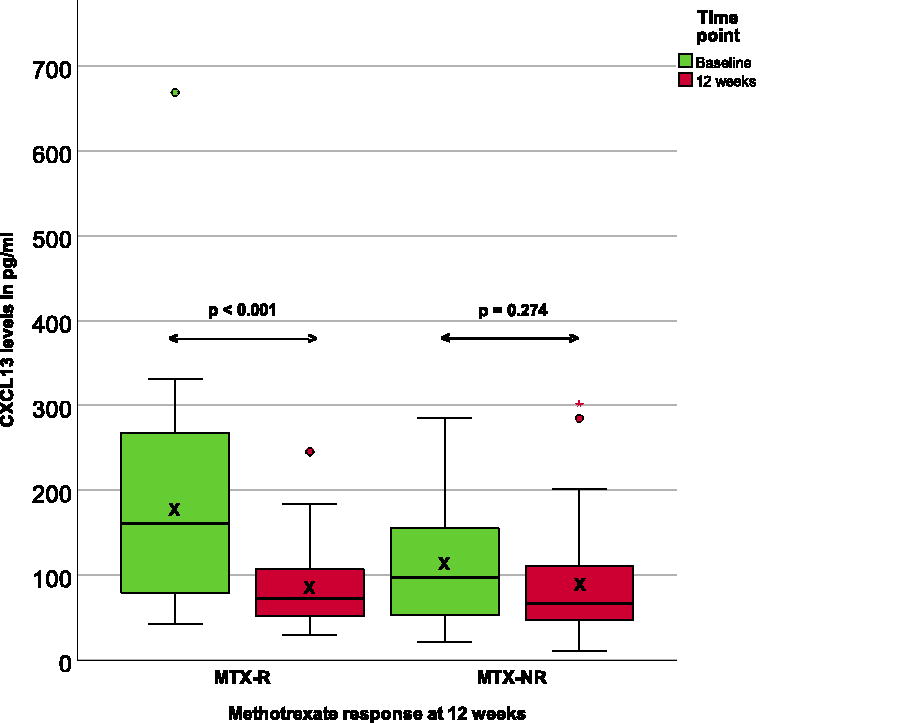
A box plot to demonstrate the change in CXCL13 values in patients with RA upon treatment with MTX. The box in the green boxes represents the responders (MTX-R group) and the blue boxes represent the nonresponders (MTX-NR group). The mean of CXCL13 values are marked in box with x. RA, rheumatoid arthritis.
Prediction of clinical response to methotrexate by baseline CXCL13 levels
The ROC curve (Fig. 3) was used to estimate the cutoff of CXCL13, which would predict remission as the response to treatment with methotrexate. It shows that a CXCL13 value of 100 pg/mL could predict a methotrexate response with a sensitivity of 69% (95% CI: 0.49–0.85) and a specificity of 52.4% (95% CI: 0.30–0.74), and an accuracy of 62% (95% CI: 0.47–0.75). The positive predictive value with a CXCL13 level >100 pg/mL was 66.67% (95% CI: 0.55–0.77) and a negative predictive value of 55% (95% CI: 0.38–0.71). CXCL13 was found to be better than baseline CRP and ESR in predicting the response to methotrexate.
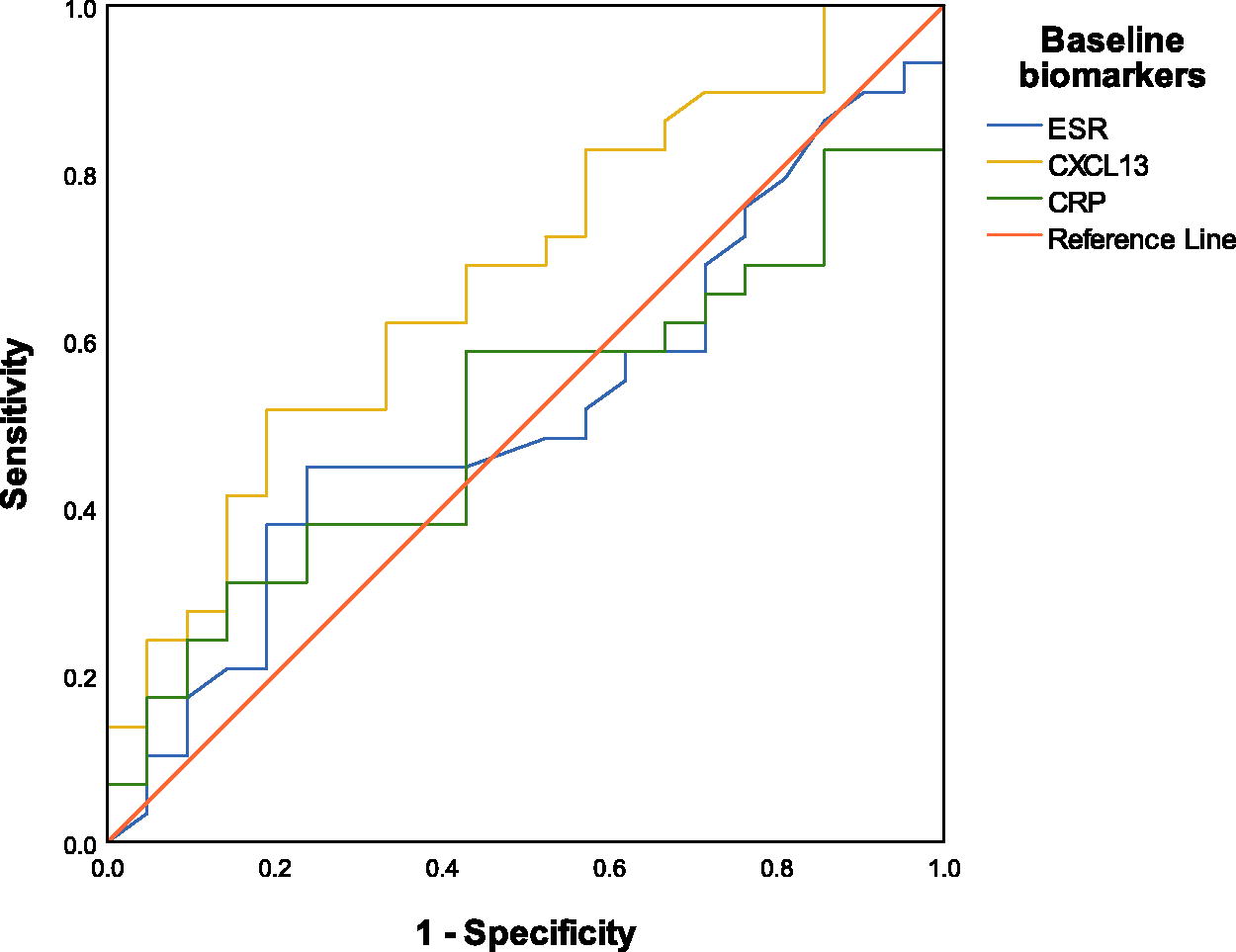
Receiver operating characteristics curve analysis for attaining remission after treatment with methotrexate. The increase in area under the curve corresponds to better diagnostic test yield.
Discussion
Our prospective cohort reveals that CXCL13 levels are higher in responsive patients—at baseline and subsequently fall when treated - compared with nonresponsive patients after a 12-week regimen of methotrexate monotherapy. Given these findings, if proven a valid predictor, CXCL13′s clinical utility in RA management can be far-reaching.
In our study, female preponderance was seen in the cohort, similar to other RA in the previous studies. The patients were unequally distributed into the two groups, and only 21 patients were categorized into the MTX-NR group, whereas 29 patients were categorized as MTX-R. Categorizing more patients in the MTX-R group was expected, as methotrexate with oral corticosteroids is demonstrated to be effective in 70% of patients. The majority of the patients belonged to the seropositive status, and only 4 patients were seronegative. The patients were distributed among the two groups with similar average gender and age. The patients in the two groups had a statistically similar distribution of tender joint count, swollen joint count, duration of the early morning stiffness, pain score, ESR, CRP, and DAS. However, it is noteworthy that the various core sets of disease variables had slightly higher but statistically nonsignificant values in the MTX-NR group. While there was significant participant attrition (12 lost to follow up), leading to their exclusion from analysis, this is unlikely to cause a selection bias toward either group, as the cause of their attrition (natural calamity) was unrelated to their disease status or treatment response.
The primary aim of the study was to determine CXCL13 as a predictive biomarker for the response to methotrexate therapy. A value above 100 pg/mL at baseline was found to be of clinical significance in differentiating the responders from nonresponders. This finding was in concordance with the international studies where the CXCL13 values were divided into the low CXCL13 group and the high CXCL13 group with a cutoff of 100 pg/mL (Greisen et al., 2014; Han et al., 2016; Rioja et al., 2008). However, the modest sensitivity and specificity in the study could be due to two reasons. First of all, the time frame used in classifying the patients as responders and nonresponders. Most studies used a time frame of 6 months or even more to classify the patients. The second reason may be the smaller sample size and the limited duration of the study. It would be ideal if the time frame to classify patients into responders and nonresponders were 24 weeks and not 12 weeks. This is mainly because of two reasons: (1) even though the therapeutic effect of methotrexate surfaces around 6–12 weeks after initiation of treatment, it peaks toward 24 weeks, and (2) the use of steroids in the early phase of treatment can mask many patients who do not have an adequate response to methotrexate.
The mean comparison of baseline CXCL13 values between the two groups showed that CXCL13 values at baseline were significantly higher in the MTX-R group. The posttreatment CXCL13 value was lower in the MTX-R group, and on comparing the mean difference between the two groups, the MTX-R group was found to have a significant difference in the pre- and posttreatment values of CXCL13. This was a significant observation in the study and suggests that patients who respond to methotrexate may have higher baseline CXCL13 values. However, contradicting this inference, a recent report by De Stefano et al. found that high baseline CXCL13 predicts lower odds of disease remission at 6 months and higher odds of second-line treatment use at 2 years of follow-up, with no significant variation by ACPA status (De Stefano et al., 2025). De Stefano and colleagues included 243 Italian participants from a 2005 treatment-naive early RA cohort who met the 1987 ACR and 2010 EULAR/ACR criteria and had available baseline serum samples. Given that these samples were stored for nearly two decades and underwent an unknown number of freeze–thaw cycles, concerns arise regarding their viability for CXCL13 testing. Nevertheless, if accurate, De Stefano’s findings suggest that the utility of CXCL13 as a biomarker may vary significantly across different ethnicities and warrants further investigation.
The observation of a higher baseline CXCL13 and the better response to treatment in these patients with higher CXCL13 values was noticed in other prior clinical studies with TNFi (O’Dell et al., 2002; Saunders et al., 2008). Bugatti et al. have already shown that higher CXCL13 levels were seen in those RA patients with a disease duration of <12 months. Here also we think that the reason for remission in patients with high CXCL13 values would be the early disease they have and the absence of fully formed memory cells in comparison with those patients in the MTX-NR group. The low levels of CXCL13 levels in chronic joints were established by Kobayashi et al. in his study, which supports the theory of low CXCL13 in established disease (Kobayashi et al., 2013). Hence, as observed in our study, the MTX-NR group, which has low CXCL levels despite being treatment naive, would have a longer disease duration and a chronic joint with a disease memory that cannot be curtailed by methotrexate monotherapy.
Correlation of CXCL13 values with the core set variables and disease activity was not established with statistical significance. However, it is interesting to notice that there was a trend toward a negative correlation in the MTX-R group and a positive correlation of swollen joint count in the MTX-NR group. Upon comparison with the previous studies, which showed a positive correlation of CXCL13 values and core set variables, DAS and radiological progression, it would become evident that these studies were conducted on patients with established RA (Rosengren et al., 2011). Similarly, the evaluation done in early RA, the OPERA cohort by Greisen et al., shows a negative correlation between CXCL13 levels, the core set variables, and disease activity (Greisen et al., 2014).
A recent systematic review by Bechman et al., which summarized 31 previous studies, suggested that CXCL13 levels have a weakly positive correlation with disease severity—similar to our results (Bechman et al., 2020). However, due to conflicting results from a limited number of studies, the authors did not find compelling evidence to recommend CXCL13 to predict treatment responses, particularly when patients received a bDMARD. Aldridge et al. also reported that blood chemokine levels, including CXCL13, reflect disease activity in early RA but do not predict remission after 24 weeks of treatment (Aldridge et al., 2022). Since we only assessed treatment response at 12 weeks and not disease remission at 24 weeks, like Albridge et al., our results are discordant. While disease remission is the ultimate therapeutic goal—which can depend on a multitude of factors - treatment response at 12 weeks is more clinically a pragmatic goal, as we initiate DMARDs in early RA to prevent complications like deforming arthritis, leading to a better prognosis for remission.
In line with Bugatti et al.’s study, Meeuwsisse et al. show that high CXCL13 is associated with increased radiographical destruction (Bugatti et al., 2014; Manzo et al., 2011; Meeuwisse et al., 2011). We did not evaluate for radiological progression, as the cohort is of early RA, and it would be too early to find any association with radiographical progression. Greisen et al. did not do the radiological evaluation and also showed that patients with high CXCL13 values were found to have a significant difference in the posttreatment values and were responders to treatment. Hence, it is evident here that the correlation of CXCL13 and the stage of the disease can be correlated. An early disease will have a high CXCL13 value and negative correlation to the core set variable, and an established disease will have a low CXCL13 value and be directly proportional to damage and methotrexate incomplete response.
The patients in the MTX-R group likely had neither established a full memory response nor fully developed a lymphoid follicle antigen response and were at an early stage of disease, and those in the MTX-NR group would have a well-developed tertiary lymphoid follicle, correlating the CXCL13 value to the swollen joint count positively. This would imply that the memory process to some degree could be halted, possibly by aggressive treatment regimens. This finding could further support that high baseline CXCL13 may be an indicator of recent-onset and active disease and that an “open window” for successful treatment does exist when the disease is in its earliest phase. It also proved that the identification of very early disease could limit the use of drugs, and methotrexate alone would be sufficient enough to revert the disease process, as high CXCL13 values could give a guide to response to treatment as well as the stage at which the disease resides at the point of treatment.
However, there are limitations to consider in the present study. Within the stipulated study recruitment period, we were only able to recruit 21 participants who were categorized as MTX-NR, reducing the power of the analysis. Nevertheless, the analysis revealed a true difference in CXCL13 levels between the groups as per our objective. Hypothetically, low-dose glucocorticoids could have lowered CXCL13 levels in RA patients; however, this was not observed in our cohort. Both groups received low-dose glucocorticoids, but after 12 weeks of treatment with methotrexate, only the MTX-R group’s mean CXCL13 levels fell to <100 pg/mL, whereas the MTX-NR group’s mean CXCL13 remained very similar to their baseline levels.
Conclusion
In conclusion, CXCL13 is a novel biomarker that predicts the stage of the disease process. CXCL13 can be used as a biomarker to identify the response to treatment with methotrexate. Treatment with csDMARDs, especially methotrexate, which is the anchor drug in the treatment of RA at the right window, would increase the response rate with methotrexate alone.
Footnotes
Acknowledgments
The authors would like to thank their patients and staff for their support in the conduct of this study.
Ethics Statement
The authors obtained approval from the institutional ethics committee before recruiting participants for this study (EC-AIMS-2017-RUMAT-217).
Authors’ Contributions
V.S.C. and M.C.B.: Conceptualized the study. M.C.B. and S.S.: Recruited participants for the study. V.S.C., S.K., and C.S.: Collected data, performed laboratory assays, and followed up with the patients. M.P.: Performed the data analysis. V.S.C. and C.S.: Wrote the first draft, while all other authors contributed critical revisions to the article.
Data Availability Statement
The corresponding author can provide the anonymized dataset upon reasonable request.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This study was conducted as part of the V.S.C.’s DM residency program requirement and received monetary support from Amrita Vishwa Vidyapeetham (University), Coimbatore, India.