
Abstract
Among honey's benefits are its anti-inflammatory and antimicrobial effects. Because gastroenteritis is an acute inflammation of the gastrointestinal tract that may be caused by a variety of microbes, the aim of the present study was to verify whether the addition of honey in oral rehydration solution (ORS) could affect the duration of symptoms of acute gastroenteritis in infants and children. One hundred infants and children with acute gastroenteritis were randomly assigned to one of two treatment groups, each consisting of 50 patients: Group I received ORS for rehydration (control), and Group II received ORS with honey. The mean ages of patients of Groups I and II were 1.5 ± 1.2 and 1.1 ± 0.8 years, respectively. In the honey-treated group the frequencies of vomiting and diarrhea were significantly reduced compared to the control group (P < .001 and P < .05, respectively). Also, the recovery time, defined as the number of hours from initiation of treatment to when normal soft stools are passed, with the patient showing normal hydration and satisfactory weight gain, was significantly shortened after honey ingestion (P < .001). In conclusion, honey added to ORS promoted rehydration of the body and sped recovery from vomiting and diarrhea.
Introduction
D
Pure honey is bactericidal for many pathogenic organisms, including enteropathogens such as Salmonella species, Shigella species, enteropathogenic Escherichia coli, and other Gram-negative organisms 3 and is a readily available source of glucose and fructose. 4 Honey substituted for glucose in the ORS was shown to shorten the duration of bacterial diarrhea, and it did not prolong the duration of nonbacterial diarrhea. 5 In the present study we evaluated the effects of adding honey, rather than substituting it for glucose, to the ORS in treatment of gastroenteritis.
Subjects and Methods
This study was a clinical trial during which 100 infants and children 2 months to 7 years old with acute gastroenteritis were admitted to the pediatric hospital of Ain Shams University, Cairo, Egypt, and were randomly assigned to one of two treatment groups, each consisted of 50 patients: Group I received an ORS for rehydration. The ORS was based on the recommendations of the World Health Organization. 6 The mean age of patients in this group was 1.5 ± 1.2 years. Group II received ORS with honey. The mean age of patients in this group was 1.1 ± 0.8 years.
The honey used was a pure unprocessed honey of multifloral origin, collected from Al Mahala, Gharbia Governorate, Egypt. The honey was supplied directly from the beekeeper without heating or gamma-irradiation, and it was tested for the presence of Clostridium botulinum spores before use (no spores were detected). Honey in a dose of 5 mL was dissolved in each 100 mL of ORS. The mixture of honey and ORS was prepared fresh and given within a maximum of 2 hours; otherwise, the mixture was discarded to avoid fungal growth. 7
Examination of honey for C. botulinum spores was done by centrifugation and filtration of the supernatant, followed by culture on cooked meat medium. 8
Dehydration severity was assessed according to Duggan et al. 9
Cases with severe dehydration or/and intractable vomiting and inability to tolerate oral fluids were excluded from the study.
Antibiotics were given in all cases with evidence of bacterial infection outside the gastrointestinal tract.
Stools (before starting treatment) were subjected to microscopic examination for parasites, culture on SS agar medium to exclude Salmonella, Shigella, and other pathogenic bacteria, and culture on specific medium for Campylobacter (Campylobacter agar base from HIMEDIA Laboratories, Mumbai, India).
The osmolarity of the mixture of ORS and honey was measured using the following equation
10
:
Because there was no urea the last factor equals 0.
Table 1 shows the composition of ORS and ORS with honey.
WHO, World Health Organization.
The frequencies of vomiting and diarrhea (times/day) throughout the period of treatment were recorded.
“Recovery time” was defined as the number of hours from initiation of treatment to when normal soft stools are passed, with the patient showing normal hydration and satisfactory weight gain. 5
The study was approved by the local ethical committee of the hospital, and an informed consent was obtained from at least one parent of each patient before the study.
Statistical analysis
The standard computer program SPSS for Windows, release 13.0 (SPSS Inc., Chicago, IL, USA) was used for data entry and analysis. All numeric variables were expressed as mean ± SD values. Comparison of different variables in various groups was done using Student's t test and the Mann-Whitney test for normal and nonparametric variables, respectively. Wilcoxon signed ranks tests were used to compare multiple readings of the same variables. The χ2 test was used to compare frequency of qualitative variables between the groups. 11 For all tests a probability (P) < .05 was considered significant.
Results
As shown in Table 2, there was no statistically significant difference between patients of both groups as regards age, sex ratio, and weight. Before starting treatment, the frequency and duration of vomiting and diarrhea did not differ significantly between the two groups. Regarding the severity of dehydration upon admission (i.e., before starting treatment), in Group I, 70% of patients had mild dehydration, and 30% had moderate dehydration, whereas in Group II, 64% had mild dehydration, and 36% had moderate dehydration, with no statistically significant differences between the two groups. Also, the results of stool examination, including microscopic examination and culture, did not differ significantly between the two groups (Fig. 1).
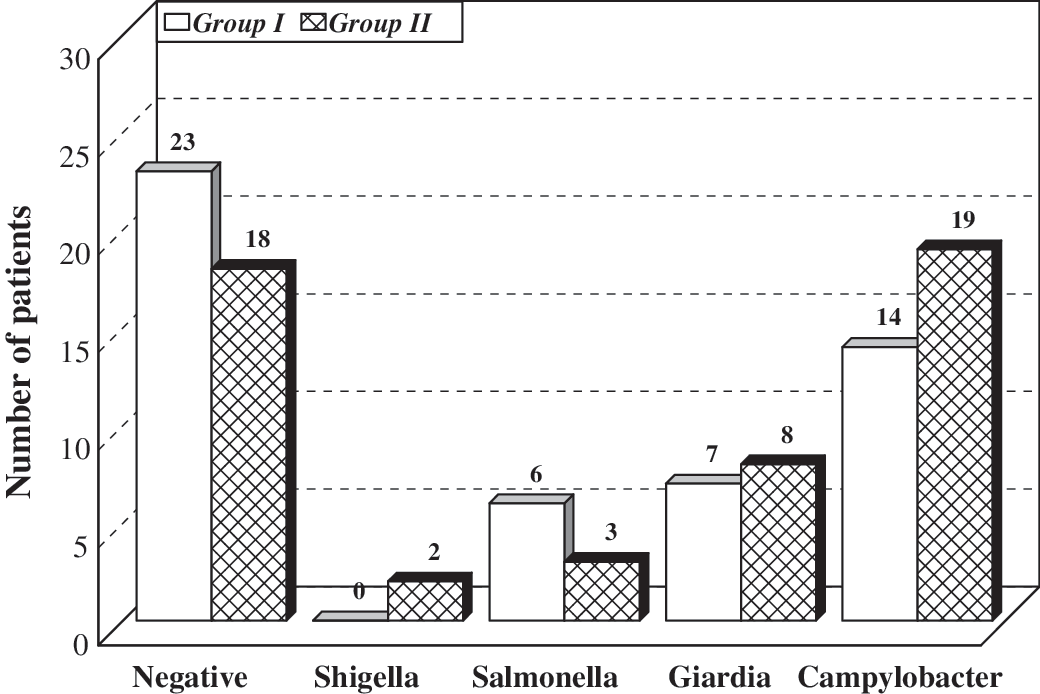
The results of stool examination before the beginning of the trial (microscopy and culture) (P > .05).
Data are mean ± SD or number (%) values as indicated. P < .05 is significant.
Table 3 shows that the weight of the patients did not differ significantly between the two groups after treatment (P > .05). However, in each group the weight showed a significant increase after treatment (P < .001).
P < .05 is significant.
As shown in Figure 2 the frequency of vomiting, before starting treatment, did not differ significantly between the two groups. However, after starting treatment, the frequency of vomiting decreased significantly in the honey-treated group compared to the control group, with the statistical difference being highly significant (P < .001).
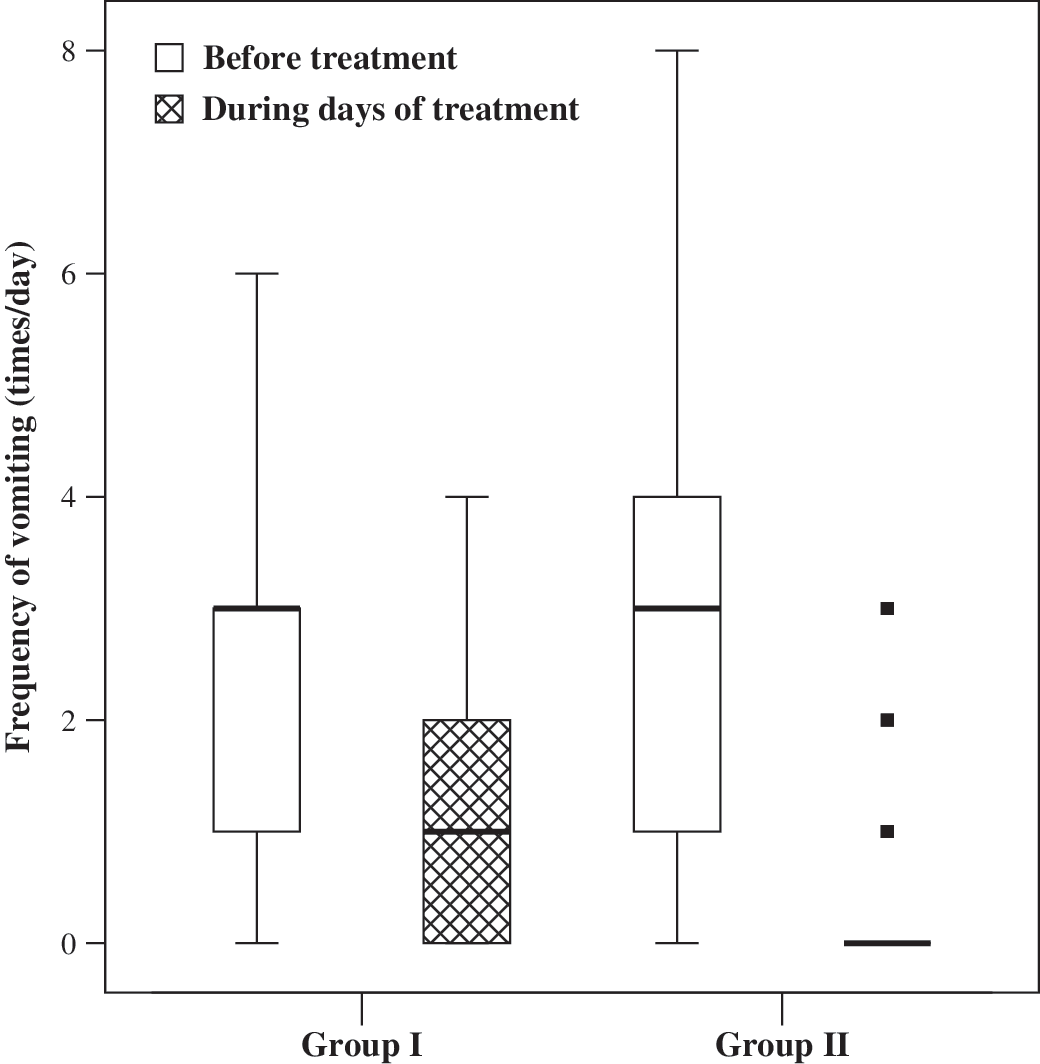
Median and interquartile range values of the frequency of vomiting among the two groups before starting treatment (P > .05) and after treatment (P < .001).
As shown in Figure 3 the frequency of diarrhea, before starting treatment, did not differ significantly between the two groups. However, after starting treatment, the frequency of diarrhea decreased significantly in the honey-treated group compared to the control group (P < .05).
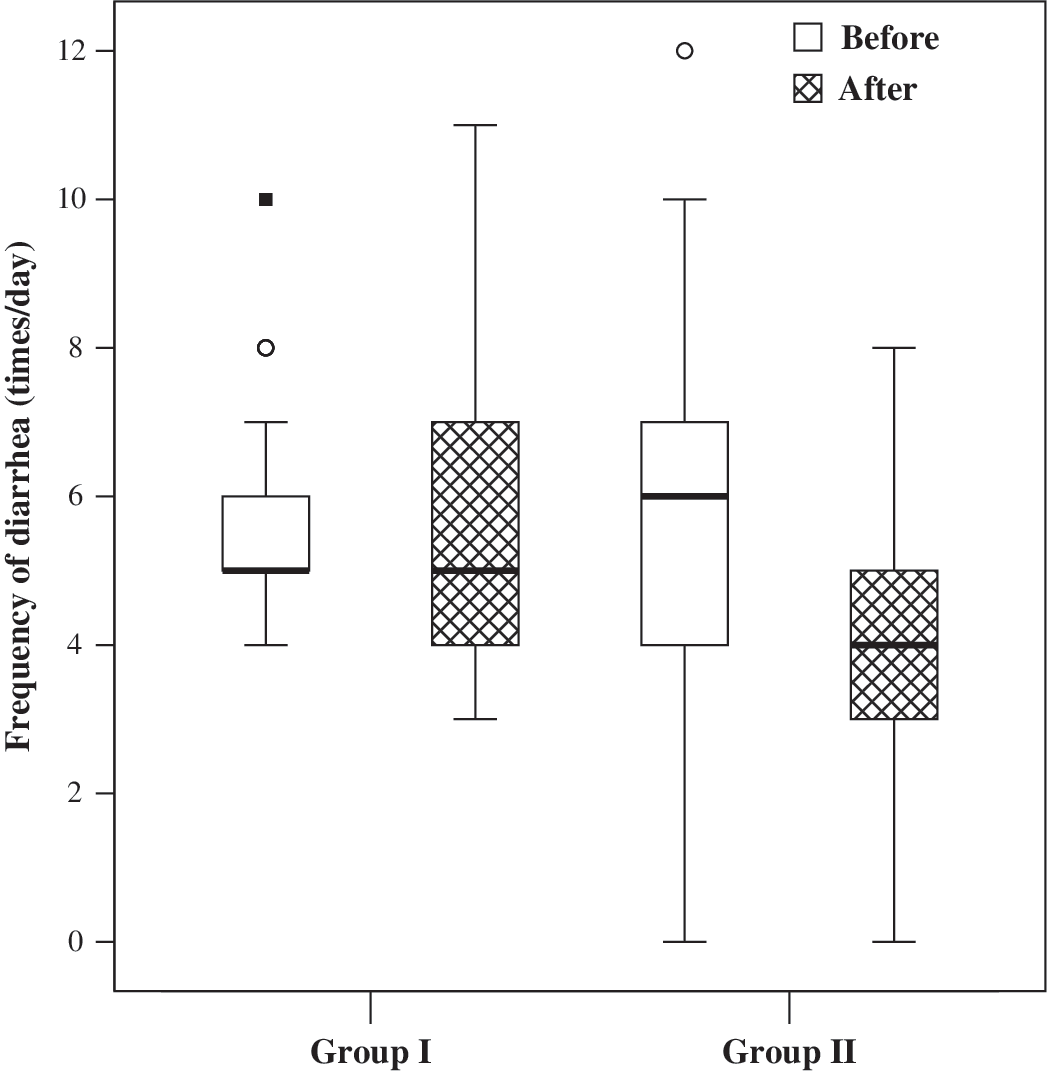
Median and interquartile range values of the frequency of diarrhea before treatment (P > .05) and after starting treatment (P < .05).
The number of patients who received antibiotics during treatment did not differ significantly between the two groups (Table 4).
P > .05 is nonsignificant.
Recovery time was significantly reduced in the honey-treated group compared with the control (P < .001) (Table 5 and Fig. 4).
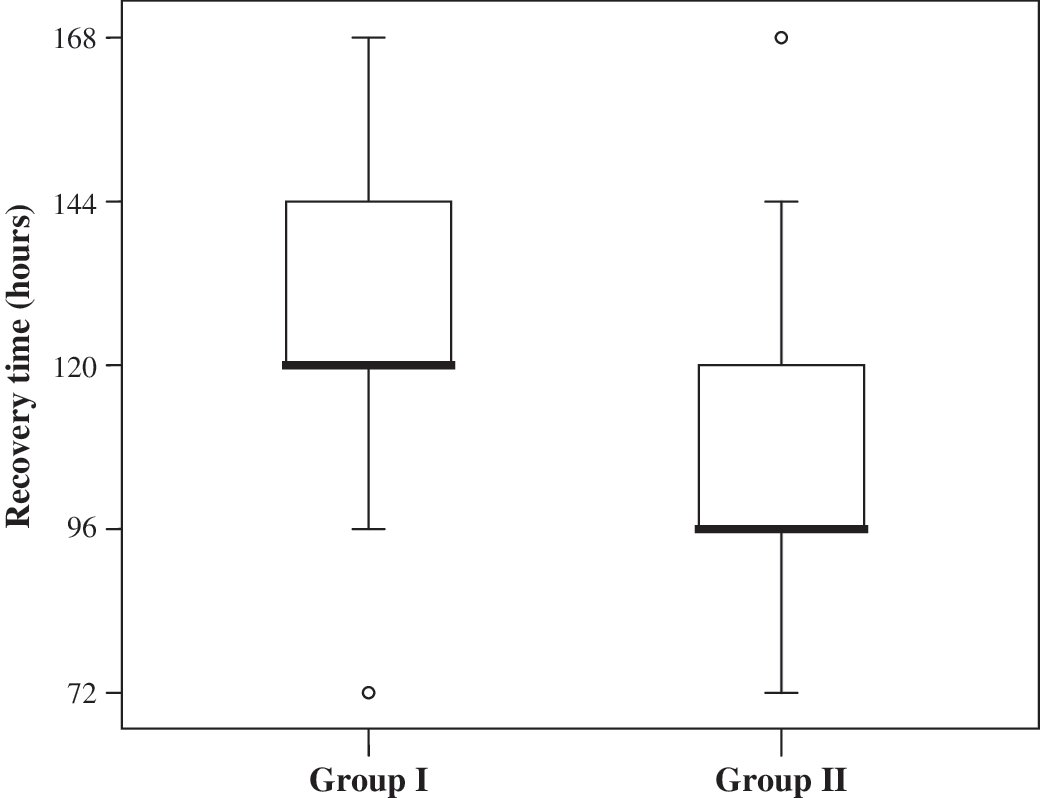
The recovery time in the two groups studied (P < .001).
P < .001 is highly significant.
Z value of the Mann-Whitney test (for nonparametric variables)/T value of Student's t test (for normal parametric variables).
Discussion
Acute gastroenteritis is an acute inflammation of the gastrointestinal tract that may be caused by a variety of microbes (viruses, bacteria, and parasites). Honey has a specific action against bacteria causing gastroenteritis 7,12,13 and has also antiviral activity, antiparasitic activity, 14 and anti-inflammatory 15 properties. The aim of the present study was to verify whether the addition of honey in the ORS could affect the duration of symptoms of acute gastroenteritis in infants and children.
The results of our study showed that honey reduced the frequency of diarrhea in patients with gastroenteritis. A possible explanation may be the known antimicrobial properties of honey against bacteria that cause gastroenteritis, 7 although we did not repeat the stool cultures to see whether the causative bacteria had been eliminated because in most cases the results of positive culture became available only after the patient had made a clinical recovery and been discharged. Concerning the antibacterial activity of honeys, studies using a wide range of honey dilutions reported the minimum inhibitory concentrations of the honeys tested to range from 4% to 10%. 7 Thus the concentration of 5% honey used in our study must have been effective as an antibacterial agent. The use of antibiotics, which were given to some of our patients for indications other than the gastroenteritis, cannot explain the difference in the treatment outcome because there was no significant statistical difference between the honey-treated and the control groups as regards the frequency of intake of antibiotics.
The present study also showed that honey may safely be added to the ORS. Although the osmolarity of such solution (i.e., honey + ORS) was more than that of the standard ORS, recovery was achieved more rapidly in the honey-treated group.
Because honey has a high sugar content it could be used to promote sodium and water absorption from the bowel in a manner analogous to the use of oral rice water and sucrose. 16 From 70% to 80% of honey is composed of fructose and glucose, with the ratio of fructose to glucose varying from 0.95 to 1.60, depending on the honey's botanical origin. 4 Fructose, which is absorbed by facilitated diffusion rather by active transport and is not coupled to sodium ions, 17 would be expected to promote water absorption without augmenting the absorption of sodium. All oral fluids containing glucose and electrolytes are used for their sodium-coupled active absorption of glucose to rehydrate patients. 18 The dose of honey used in our study—that is, 5 mL per 100 mL (50 mL/L) of oral fluid containing 75.4 mmol of sodium, 20.7 mmol of potassium, and 70 mmol of chloride per liter—provided 109 mmol of glucose/L. Honey added to ORS resulted in an additional 0.4 mmol of sodium and 0.7 mmol of potassium in each liter of oral fluid containing honey. In our opinion these are very small amounts and would not be expected to influence the outcome. Furthermore, despite its high sugar content honey did not result in osmotic diarrhea when added to the ORS. This is because in the honey-treated group the frequency of diarrhea and the recovery time were significantly reduced. In the study of Haffejee and Moosa 5 honey was substituted for glucose in the ORS, and they found that honey shortened the duration of bacterial diarrhea and did not prolong the duration of nonbacterial diarrhea. In our study the frequency of both bacterial and nonbacterial diarrhea was reduced, although honey was added to and not substituted for glucose in the ORS. Furthermore, probably adding honey to ORS is technically easier and less expensive than substituting honey for glucose in the ORS. In addition, honey added to ORS made the solution a little bit sweet and possibly more acceptable.
Footnotes
Author Disclosure Statement
No competing financial interests exist. No funds were received for this work.