
Abstract
Pressurized whey supplementation, by its antioxidant and nutritional properties, may improve exercise tolerance and potentiate the effects of exercise training in patients with chronic obstructive pulmonary disease (COPD). In this randomized, double-blind, placebo-controlled study, 22 patients with COPD were allocated to receive active pressurized whey or placebo (casein) dietary supplementation for a 16-week period. Patients continued their usual physical activities for the first 8 weeks, whereas they were subjected to an exercise training program for the remaining 8 weeks of the study. Patients were evaluated at baseline, after 8 weeks of supplementation alone (time point, 8 weeks), and after 8 weeks of its combination with exercise training (time point, 16 weeks). The constant workrate cycle endurance test (CET), potentiated quadriceps twitch force, mid-thigh cross-sectional area, and Chronic Respiratory Questionnaire (CRQ) were used to evaluate the effects of treatments. The inflammatory (C-reactive protein and interleukin-6) and oxidant/antioxidant (protein oxidation and glutathione) blood profiles were also characterized. At week 8, there was no increase in CET time in either group. At week 16, there was a statistically significant increase in CET time in the whey-only group (P < .05). Further, at week 16, there was clinically significant improvement in the Dyspnea and the Mastery scales of the CRQ in both groups. Also, the Fatigue and Emotional Control scales of the CRQ showed clinically significant improvement in the whey-only group. Study interventions did not modify significantly the systemic inflammatory and oxidative stress markers that were assessed. Thus dietary supplementation with pressurized whey may potentiate the effects of exercise training on exercise tolerance and quality of life in patients with COPD.
Introduction
E
Oxidative stress is already a prominent feature in COPD linked to disease progression, 6 exercise intolerance, 13 and peripheral muscle dysfunction. 14 –16 Therefore, use of a combination of pressurized whey supplementation with antioxidant properties (to combat oxidative stress) and exercise training (to improve exercise tolerance and peripheral muscle function) in patients with COPD is likely to provide greater beneficial effects compared to exercise training alone. In the healthy population, this combination has resulted in decreased oxidative stress 17 with no significant improvement in exercise tolerance. 18 In patients with COPD, no studies have investigated the effects of the combination of antioxidant supplementation and exercise training. However, one study investigating the effects of antioxidant supplementation on acute exercise tolerance has shown that it can increase exercise tolerance in patients with COPD. 13
Lands et al. 19 have developed dietary supplementation based on pressurized whey. Treatment of whey with hyperbaric pressure results in protein unfolding 20 and enhanced in vitro digestion. 21 Whey is rich in cysteine and other essential amino acids, 22 which can increase the synthesis of glutathione, a crucial intracellular antioxidant. 23,24 In previous studies, we demonstrated that supplementation with pressurized whey increased intracellular glutathione 24 and improved pulmonary function and systemic markers of inflammation in patients with cystic fibrosis. 19
In addition, dietary supplementation with pressurized whey provides essential amino acids and could address protein malnourishment in patients with COPD. Patients with COPD are at risk for malnutrition, 25 with oxidative stress and inflammation implicated in an alteration of protein metabolism. 26 Nutritional intervention alone has no significant effect on anthropometric measurements or exercise tolerance, 27 but its combination with exercise training may improve both total and fat-free mass and exercise tolerance. 28
In light of the impaired antioxidant capacity in COPD and the role of oxidative stress balance in peripheral muscle function, we hypothesized that whey supplementation would potentiate the effects of exercise training on exercise tolerance in patients with COPD. To address this hypothesis, we conducted a randomized, double-blind, placebo-controlled pilot study. We evaluated the impact of the combination of dietary supplementation with pressurized whey and exercise training on (1) exercise tolerance, (2) peripheral muscle function, (3) health-related quality of life, and (4) systemic markers of inflammation, oxidative stress, and antioxidant status. We further assessed to what extent pressurized whey supplementation alone would improve the aforementioned parameters.
Subjects and Methods
Subjects and study design
Twenty-two patients were recruited to participate in this randomized, double-blind, placebo-controlled pilot study. Sedentary, ex-smoker, and stable patients with COPD (forced expiratory volume in 1 second [FEV1] < 70% predicted, FEV1/forced vital capacity [FVC] ratio <0.7), free of other systemic diseases (cancer, diabetes, heart disease), were included in the study. Baseline evaluation included spirometry and lung volumes, constant workrate cycle endurance test (CET), peripheral muscle fatigue assessment using magnetic stimulation, health-related quality of life questionnaire, and systemic markers of inflammation, oxidative stress, and antioxidant status. Figure 1 shows study design. After baseline evaluation, patients were randomized to receive 16 weeks of placebo (casein) or pressurized whey supplementation. During the first 8 weeks, participants were asked to continue their normal activities (supplementation phase). After a repeated evaluation, patients embarked on an 8-week exercise training program to complete this 16-week study (supplementation + exercise training phase). The training program consisted of 8 weeks of triweekly 90-minute exercise sessions that combined endurance and resistance exercises. 29 Education about the COPD and self-management strategies were also provided to the participants. The trial ended at week 16, after the third evaluation. This study was approved by the ethics committee of our institution, and all the patients gave informed consent to participate.
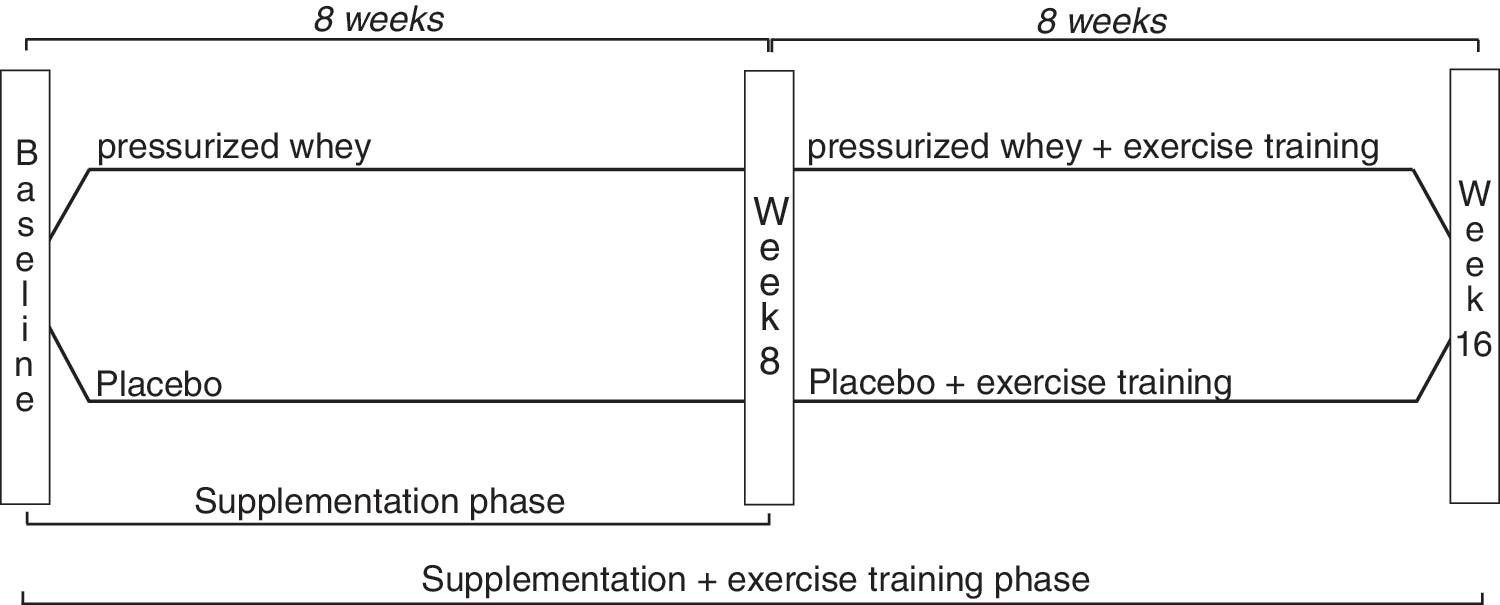
Study design.
Pulmonary function testing
Spirometry and lung volumes were measured according to recommended procedures. 30,31 Results were compared with predicted normal values from the European Community for Coal and Steel/European Respiratory Society. 32
CET
Peak cycling capacity was determined with progressive cycle ergometry with workload increases of 10 W/minute until exhaustion. 33 Peak work capacity was related to the normal values of Jones. 33
The CET was performed on an electromagnetically braked cycle ergometer (Quinton Corival 400; A-H Robins, Seattle, WA, USA), and the workload was set at 80% of peak work capacity achieved during incremental cycle ergometry. The CET was preceded by a 1-minute unloaded warm-up period, and patients were asked to cycle for as long as possible at a speed of 60 rpm. No encouragement was provided during the tests to avoid any potential confounding effect on exercise performance. 34 Subjects were connected to the exercise circuit through a mouthpiece and wore a noseclip during the test. Ventilation, oxygen consumption, and carbon dioxide output were measured at rest and during exercise on a breath-by-breath basis (Vmax® Legacy, SensorMedics®, Yorba Linda, CA, USA). Heart rate was monitored by an electrocardiograph (Cardiosoft program and Corina amplifier, GE Medical Systems, Milwaukee, WI, USA). The minimal clinical important difference for the change in endurance time to CET was set at 100 seconds. 35
Peripheral muscle function
Maximal voluntary strength of the quadriceps (maximal voluntary contraction [MVC]) was recorded during 3-second isometric maximal contractions. Each MVC maneuver was separated by 30 seconds, and reported values correspond to the mean of the three strongest contractions. Verbal encouragements were provided during this maneuver. Subjects were sitting in a recumbent chair (N-K 330 Exercise Table, N-K Products, Elsinore, CA, USA) with 90° knee flexion and the ankle attached to a strain gauge (Hewlett-Packard, Palo Alto, CA, USA). The strain gauge was adjusted perpendicularly to the leg, and the position was maintained throughout the protocol. The strain gauge signal was amplified (model 8811A amplifier; Hewlett-Packard), transformed by an analog transducer (Biopac, Santa Barbara, CA, USA), and linked to a computer for data analysis.
To evaluate lower limb muscle endurance, cycles of 5-second isometric contractions at 60% of MVC followed by 5 seconds of rest were repeated until exhaustion. Time to exhaustion was noted. In repeated evaluations, the intensity and duration of the isometric exercise were identical to baseline, so that the same fatigue stimulus was provided throughout all evaluations. The degree of peripheral muscle fatigue induced by the lower limb endurance protocol was assessed by measuring quadriceps strength during magnetic stimulation of the femoral nerve, prior to and 10, 20, and 30 minutes after the protocol, as previously reported. 5,36 In the supine position, the dominant leg was stabilized on a wooden frame with the knee and the hip flexed at 45°. The box design ensured a standard leg position during all measurements, and the flexion of the quadriceps remained identical throughout the experiment. The ankle was attached to a strain gauge (Hewlett-Packard) through a nonelastic ankle strap to measure the isometric knee-extension tension. Care was taken to ensure that the ankle strap and gauge were perpendicular to the leg and the frame box. The position of the strap was marked on the leg, ensuring that it remained identical throughout the pre- and post-exercise measurements. The strain gauge signal was amplified (model amplifier 8811A; Hewlett-Packard), transformed by an analog transducer (Biopac), and stored on a computer for data analysis.
The femoral nerve was stimulated using a commercial magnetic stimulator (Magstim 200; Magstim, Whitland, UK) and a 42-mm figure-eight coil. The coil was positioned over the femoral nerve. The coil position leading to the strongest muscle contraction was localized and used for subsequent twitches. Because potentiated twitches appear to be more sensitive for detecting fatigue than nonpotentiated twitches, 37,38 quadriceps twitch force was obtained 1 second after a 5-second isometric contraction at near-maximal intensity. A set of 10 potentiated twitches was obtained at 100% of stimulator output before (after 15 minutes of rest) and 10, 20, and 30 minutes after exercise. At this intensity, magnetic stimulation is supramaximal, i.e., an increase in stimulus intensity does not result in a further increase in the strength of the contraction. 5 Reported quadriceps twitch force values are the mean of the three strongest contractions. The preload on the strain gauge was subtracted from the peak tension measured during the twitch maneuvers so that the reported quadriceps twitch force values include only the tension developed by the quadriceps contraction. We have previously reported the validity and reproducibility of this method. 5
Health status
Health status was evaluated using a validated French-Canadian version of the Chronic Respiratory Questionnaire (CRQ). 39 The CRQ is a COPD-specific questionnaire of health status. 40 The 20 items are separated into four domains: Dyspnea, Fatigue, Mastery, and Emotional Control. A mean item change of 0.5 in any domain is considered clinically significant. 41
Blood inflammatory and oxidant/antioxidant profiles
The antecubital venous blood was sampled before the isometric quadriceps muscle exercise, at the same time of the day (±90 minutes). Blood was centrifuged for 15 minutes, and plasma was obtained, aliquoted, and stored at –80°C until further analysis. Commercial enzyme-linked immunosorbent assay kits (R&D Systems, Minneapolis, MN, USA) were used to measure the plasma levels of interleukin-6 (IL-6). C-reactive protein (CRP) plasma levels were measured with a nephelometer immunoassay (BN ProSpec nephelometer; Dade Behring, Deerfield, IL, USA). Protein oxidation was detected using the Oxyblot™ kit (Serologicals Corp., Norcross, GA, USA) and analyzed by western blot.
To evaluate antioxidant status, we quantified total glutathione in whole blood lysates. Venous blood was collected in EDTA-containing tubes and immediately placed on wet ice. Two hundred microliters of blood was diluted with 200 μL of 100 mM phosphate buffer (pH 7.4) and deproteinized with 400 μL of ice-cold 10% trichloroacetic acid. After vigorous vortex-mixing, samples were incubated on ice for 5 minutes. Proteins were removed by high-speed centrifugation (microcentrifuge, 12,000 g, 10 minutes, 4°C). Aliquots of protein-free supernatants were stored at –80°C until further analysis. To quantify total glutathione, samples were diluted with 10% trichloroacetic acid and neutralized with 100 mM phosphate buffer (pH 7.4) containing 5 mM EDTA. Glutathione analysis was conducted by the method established in our previous publications. 42,43
Dietary supplementation with pressurized whey
Dietary supplementation with pressurized whey consisted in a 20-g daily dose of pressurized whey. This supplementation has been proven to increase intracellular concentrations of glutathione 24 and improved pulmonary function and systemic markers of inflammation in patients with cystic fibrosis. 19 Matching placebo supplementation consisted of 20 g of casein. Active and casein supplementations were premixed in individual packages (120 mL) of applesauce and had a similar appearance. Patients were instructed to take one 120-mL portion per day. The applesauce ued for this study contained 20 g of carbohydrate/120 mL and no fat or protein and had a caloric content of 80 kcal/120 mL. The supplementation therefore added 80 nonprotein kcal and 80 protein kcal in both study groups.
Statistical analysis
Data are reported as mean ± SD values. The primary outcome was the change in endurance time to CET from baseline to week 16 (combination of exercise training and whey supplementation). Endurance time was defined as the total duration of pedaling, excluding the 1-minute warm-up period. Repeated-measure analysis of variance was used to compare longitudinal changes within each group. Between-groups comparisons were done using analysis of variance. Statistical significance was set at .05.
Results
Patient characteristics
Table 1 shows patient characteristics and baseline lung function. Patients had on average moderate to severe airflow obstruction in association with hyperinflation and reduced diffusion capacity. Age, body mass index, and smoking history were not significantly different between groups. There was a significantly higher proportion of women in the casein group compared to the whey group (P < .05). Twelve patients were randomized to the whey supplementation group, and 10 patients were allocated to casein supplementation. Two patients randomized in the whey group completed only the supplementation phase because of pneumonia (n = 1) and refusal to participate in the exercise training program (n = 1). Thus, 10 patients in each group completed the 16-week duration study. Attendance to the exercise training sessions was closely monitored and was similar between the two groups: all patients attended at least 90% of sessions (22 sessions).
Data are mean ± SD values. There was no statistically significant difference between groups.
FRC, functional residual capacity; IC, inspiratory capacity; TLC, total lung capacity.
Average amount of protein supplementation per kg of body mass was 0.25 ± 0.4 and 0.30 ± 0.60 g/kg/day (whey and casein group, respectively; P = .02), corresponding to 0.98 ± 0.16 and 1.19 ± 0.25 kcal/kg/day (whey and casein group, respectively; P = .02). The increased caloric intake related to the applesauce vehicle alone averaged 2.0 ± 0.3 kcal/kg/day and 2.4 ± 0.5 kcal/kg/day in the whey and casein group, respectively (P = .02).
Table 2 shows the time course of expiratory flows, lung volumes, and lung diffusion capacity for carbon monoxide (DLCO) throughout the trial. There were no significant changes in lung function, lung volumes, or DLCO within and between groups with either intervention (all P > .05). Compared to baseline, body weight changed by 0.39 ± 2.54 and 0.35 ± 1.58 kg at week 8 (whey and casein group, respectively; P = .99) and by −0.09 ± 2.42 and −1.14 ± 2.59 kg at week 16 (whey and casein group, respectively; P = .40). These changes were small and not significantly different from baseline at week 8 or 16 for either group.
Data are mean ± SD values. There was no statistically significant change between and within groups.
Exercise tolerance
Time courses in endurance time to CET are shown in Figure 2A. Baseline CET time was not different between groups (277.2 ± 108.8 vs. 226.6 ± 77.1 seconds for whey and casein, respectively; P = .23). At week 16, the whey group showed statistically significant improvements in CET time (P < .05) that was not seen in the casein group. However, the evolution of CET time during the trial was not significantly different between groups. Figure 2B shows individual improvements in CET time at week 16; a clinically significant improvement 35 (>100 seconds) was seen in five (33%) and two (20%) patients in the whey and casein groups, respectively (P = .16). At week 8, there was no significant improvement in exercise tolerance for either group.

CET: (
Peripheral muscle function and mid-thigh cross sectional area (MTCSA)
During the isometric quadriceps endurance protocol, load (25.8 ± 4.3 vs. 23.7 ± 7.2 kg for whey and casein, respectively; P = .42) and time to exhaustion (606.4 ± 347.4 vs. 602.5 ± 362.9 seconds for whey and casein, respectively; P = .98) were not different between groups. Peripheral muscle strength (MVC and potentiated twitch force at rest [TWqre]), the decrease in quadriceps force after the quadriceps endurance protocol (potentiated twitch force at 10 minutes [TW10]), and MTCSA results are shown in Figure 3. There was no significant change in any of these parameters with the study interventions for either group.

Evolution of (
Health-related quality of life
Improvements in quality of life are shown in Table 3. There was clinically significant improvement in the Dyspnea and the Mastery scales in both groups at week 16. However, the whey group showed clinically significant improvements in the Fatigue and Emotional Control scales that were not observed in the casein group, also at week 16. At week 8, whey supplementation induced clinically significant change in the Fatigue and Dyspnea scales of the CRQ that were not observed in the casein group. Also, the improvements in the Fatigue and Emotional Control scales at week 8 were statistically greater in the whey group compared to the casein group (P < .05).
Data are mean ± SD values. Minimal important clinical difference was P = .05.
P < .05 versus baseline within group, † P < .01 versus baseline between groups.
Inflammatory and oxidant/antioxidant profiles
Blood inflammation and oxidative stress results are shown in Table 4. Baseline IL-6, CRP, and advanced oxidation protein products (AOPP) were not significantly different between groups. Neither group showed significant variation in IL-6, CRP, or AOPP at week 8 or week 16. At week 16, blood glutathione was not significantly increased in either group.
Data are mean ± SD values. There was no statistically significant change between and within groups.
Discussion
This is the first study to investigate the effects of combining whey protein supplementation and exercise training in patients with COPD. The main study findings are as follows: (1) pressurized whey supplementation in combination with exercise training increased exercise tolerance measured by the CET, (2) pressurized whey protein supplementation may potentiate the impact of exercise training on exercise tolerance, (3) increased CET time in this study was not associated with reduced contractile fatigue of the quadriceps muscle or with an increase in quadriceps strength or mass, (4) pressurized whey protein supplementation alone improved dyspnea and fatigue on the CRQ, and (5) exercise training and whey protein supplementation in patients with COPD did not modify significantly the systemic inflammatory and oxidative stress markers under protocol.
It is possible to look at the results from two different perspectives: the supplementation constitutes an added caloric intake that, combined with an anabolic stimulus, might improve anthropometric profile. Both supplementations constituted of 20 g (80 kcal) of proteins, resulting in increases of 0.98 ± 0.16 and 1.19 ± 0.25 kcal/kg/day (whey and casein, respectively; P = .02). These small increases in protein caloric intake did not affect body weight during the study in either group. It is likely that caloric value of the supplementation was not sufficient to induce changes in body weight. 6,27,44 –47
Pressurized whey protein supplementation can also have antioxidant properties by increasing intracellular glutathione concentrations. 24 In a recent pilot study in pediatric and adult patients with cystic fibrosis, 19 1-month supplementation with pressurized whey (20 g/day under 18 years of age, 40 g/day greater than 18 years of age) enhanced nutritional status in both children and adults and improved lung function in children. The supplementation resulted in patients receiving on average 0.7 g/kg/day protein and 7–8 kcal/kg/day calories. Of note is that whole blood glutathione did not change in that study. The lack of increase in muscle mass in the current study may be due to the relatively low dose of the supplement. This may also account for the lack of change in whole blood glutathione. Alternatively, the lack of glutathione change may be that whole blood values do not adequately reflect changes in inflammatory cells or other tissue. 24
The significant increase in CET time observed in the whey group supports the effect of the experimental supplementation in our patients with COPD. Previous studies support the positive impact of antioxidant supplementation on this outcome parameter, but methodology for evaluating exercise tolerance has not been consistent across studies. In a study on healthy men, Lands et al. 42 found that peak power and 30-second work capacity were significantly increased following antioxidant supplementation. These tests of exercise capacity, however, relate more to anaerobic power 48 than to the endurance time to CET, as assessed in the present study. Studies have also shown an improvement in local muscle endurance following N-acetylcysteine supplementation in patients with COPD. 13 Whether supplementation with thiol donors can improve whole-body exercise capacity may improve exercise is currently being debated, 49 –52 and additional research is required.
One potential mechanism by which antioxidant supplementation could improve endurance time on the CET is by increasing quadriceps function. A well-balanced redox status yields the best contractile force in skeletal muscle. 53 Based on the fact that exercise training in COPD may result in oxidative stress, the trend of increased quadriceps strength in the pressurized whey group (Fig. 3A) supports this theory. We failed, however, to detect any significant effect on quadriceps susceptibility to fatigue after pressurized whey supplementation. In vivo studies using N-acetylcysteine have shown reductions in muscle fatigue between 15% and 60% in varying muscle groups. 54 –57 However, these studies show discrepancies in the muscle group (quadriceps, tibialis anterior, diaphragm, and forearm) and methods (electrostimulation, voluntary contractions) used to investigate the effects of antioxidant supplementation on muscle fatigue, therefore making conclusions difficult.
In the study by Koechlin et al., 13 quadriceps muscle function of patients with COPD was evaluated by repeated dynamic contractions of the quadriceps until exhaustion. In our study, we used a similar fatiguing stimulus (isometric contractions of the quadriceps until exhaustions), repeated after supplementation alone and its combination with exercise training. Instead of using time to exhaustion, muscle fatigue was evaluated using magnetic stimulation. It is quite possible that these two methods do not measure the same type of muscle fatigue. Time to exhaustion requires volitional activation and is as much a measure of muscle contracting capacity as of psychophysiological tolerance to fatigue. By bypassing volitional activation, we were able to estimate in a truly physiological manner the effects of pressurized whey supplementation on the quadriceps's contractile apparatus, and we could not find evidence supporting an effect of our supplementation on this parameter. Previous studies have, however, shown that thiol donors can improve muscle performance following a nonvolitional exercise using electrical stimulation. 55 It therefore seems that contractile fatigue was not significantly influenced by glutathione in the present study. Again, this could be related to the relatively small amount of pressurized whey protein supplied and the inability of this supplementation to increase substantially glutathione levels.
One important finding is that the improvement in exercise tolerance seems associated with an increased tolerance to central fatigue, as shown by the significant changes in fatigue perception on the CRQ. Although there was no correlations between improvements in CET time and improvements in CRQ fatigue scale, the significant decrease in perceived fatigue, both statistically and clinically, points to an involvement of the pressurized whey supplementation in the patient's perception of fatigue. Research in the field of fibromyalgia and chronic fatigue syndrome, both characterized by whole-body fatigue, has shown evidence of an implication of oxidative stress in the clinical manifestations of the disease. 58,59 It also of interest to note that pressurized whey supplementation alone had an impact on perceived fatigue and emotional control that was not significantly inferior to that of exercise training. Whey protein is rich in branched-chain amino acids. Several supplementation trials indicate that branched-chain amino acids can contribute to combat fatigue and to improve mental and physical performance in athletes. 60,61 Furthermore, relative high blood levels of tryptophan relative to the levels of branched-chain amino acids have been implicated as a possible cause of acute physiological and psychological fatigue (central fatigue) during exercise 62 and the chronic fatigue syndrome. 63
Study limitations
Exercise training is known to increase exercise tolerance 64 and to specifically increase endurance time to CET. 35 One problem we faced was the fact that exercise training in combination with placebo (casein) did not increase time to CET. Lower adherence to the exercise training program in the casein group could have lowered its efficacy, but it was not different between groups. Intensity of the training was standardized for all patients, but actual work done by patients during individual sessions was not compiled. It may have been higher in patients taking pressurized whey supplementation and thus have potentially increased the benefits of training, as higher-intensity training is known to be more beneficial in terms of improving exercise tolerance to constant workrate exercise. 65
This pilot study was undertaken to investigate whether pressurized whey supplementation could potentiate exercise training along with the physiological mechanisms that supported it. Sample-size calculations based on previous data 13 suggested that 20 patients would be sufficient to attain significance in CET time. However, based on the variability in CET time observed in this study, post hoc analysis determined that 80 patients in each group would be needed to confirm that the whey supplementation group has statistically and clinically (improvement in endurance time to CET > 100 seconds) greater efficacy to improve endurance time to CET than the casein supplementation group, when these two nutritional therapies are associated with exercise training.
Conclusions
Dietary supplementation with pressurized whey may potentiate the impact of exercise training on exercise tolerance, with no evidence of an improvement in quadriceps strength or mass or in the occurrence of contractile fatigue of the quadriceps. Pressurized whey supplementation was associated with an improvement in dyspnea and fatigue on the CRQ, suggestive of an involvement of central mechanisms to the observed improvement in exercise tolerance seen in this study.
Footnotes
Acknowledgments
The authors would like to thank Leahy Orchards Inc. for providing the whey supplementation and the medium. They also extend their thanks to Annie Michaud, Marie-Ève Paré, and Christine Racine for their assistance with blood sample analysis. They would also like to thank Josée Picard, Brigite Jean, Marthe Bélanger, and Marie-Josée Breton for their help in gathering clinical data. They would also like to thank Dr. Stan Kubow of the McGill School of Dietetics and Human Nutrition for helpful editorial comments. F.M. is a research scholar of the Fonds de la Recherche en Santé du Québec. This study was supported by the Réseau en Santé respiratoire du Québec and the Canadian Institute of Health Research (grant MOP-84091).
Author Disclosure Statement
L.C.L. is an inventor on a McGill University patent application for pressurized whey. He is also a shareholder in Medibarics, which has an exclusive license from McGill University for pressurized whey. L.L., N.D., D.S., J.M., S.P., P.L., and F.M. declare no competing financial interests exist.