
Abstract
Alterations in plasma cholesterol concentrations, especially increases in low-density lipoprotein (LDL), are well-known risk factors in the development of atherosclerosis. Numerous studies have examined the lipid-lowering effects of functional soy-containing foods, but few have specifically examined soymilk, with equivocal findings reported. In September 2008, a single-blind, randomized, controlled trial was conducted on 32 postmenopausal women at Baylor University, Waco, TX, USA. After a 2-week run-in period, subjects were randomly assigned to consume three servings of vanilla soy (n = 16) or reduced-fat dairy (n = 16) milk per day for 4 weeks. Plasma lipid profiles were obtained pre- and post-supplementation. Plasma high-density lipoprotein, LDL, and triglycerides were not significantly different between groups post-intervention (P = .45) or from baseline (P = .83). Separate analysis of plasma total cholesterol levels yielded similar results (P = .19 and P = .92, respectively). Furthermore, subanalyses controlling for dyslipidemia (n = 23) and lipid-lowering medication usage (n = 28) did not significantly alter results. Despite good dietary compliance, our study failed to show a significant hypocholesterolemic effect of soymilk consumption in this postmenopausal female population. Potential reasons for this nonsignificant finding are discussed, and future research directions are presented.
Introduction
C
The exact mechanism by which soy lowers blood lipids remains unclear, but in 1999 the Food and Drug Administration approved a health claim stating that the inclusion of soy protein into a diet low in saturated fat and cholesterol may reduce the risk of coronary heart disease by lowering blood cholesterol levels. 8 This claim was substantiated in numerous clinical trials, including the seminal meta-analysis by Anderson et al., 7 which showed that an average intake of 47 g of soy protein/day resulted in a 9% decrease in total cholesterol (TC), 13% decrease in LDL, 10% decrease in triglyceride (TG), and a moderate 2.4% increase in high-density lipoprotein (HDL). More recent studies 6 suggest that the beneficial effect of soy protein on cholesterol may be more modest than originally proposed; however, over a period of many years even a modest improvement in blood lipids levels has the potential to decrease coronary heart disease risk.
With regard to isoflavones, current research indicates that when consumption of soy protein-containing isoflavones is compared to that of isoflavone-depleted soy protein, lipid profiles are significantly improved. 5,9 Results from a recent meta-analysis 6 suggest that soy protein coupled with at least 40 mg/day isoflavones has lipid-lowering effects and that such effects are magnified when ingestion increases to 80 mg/day. Interestingly, these beneficial results may not apply to isoflavone intake alone. In a study examining the effects of 6 weeks of isolated isoflavone intake (90 mg/day vs. placebo) on cardiovascular risk factors in moderately hypercholesterolemic, postmenopausal women, 10 the authors found that while both groups experienced small reductions in total and LDL cholesterol, this decrease was not statistically significant, and no difference was noted between groups. Therefore, in light of recent research, it appears that supplementing a combination of soy protein with appreciable amounts of isoflavones may yield the most favorable lipid-lowering effect.
Unfortunately, many of the clinical studies addressing the lipid-lowering potential of soy often fail to incorporate commercially available soyfoods, such as soymilk. Because it is plausible that synergistic effects may exist among isolated soy constituents, there is considerable need for studies examining whole soyfood consumption. To date, only a few studies have specifically examined the lipid-lowering benefits of soymilk consumption, 11 –15 and the results of these studies have been equivocal. Due to the lack of consensus in the literature, as well as the current reevaluation of the support for the Food and Drug Administration health claim, the purpose of this study was to examine the effects of soymilk consumption on plasma lipid levels in a postmenopausal female population.
Materials and Methods
Primary and secondary outcomes
This analysis was a part of a trial originally designed to examine the ability of soymilk to attenuate exercise induced inflammation and oxidative stress. The primary outcome of this substudy was to examine the lipid-mediating properties of soymilk. We hypothesized that participants randomized to consume three servings of soymilk per day for 4 weeks would have statistically greater reductions in traditional markers of cholesterol than the control (dairy) group. Specifically, we examined plasma levels of TG, TC, LDL, and HDL in the entire group of participants post-intervention. Secondary outcomes included the change in the aforementioned cholesterol values over the supplementation period and two subanalyses of the dataset controlling for select confounders. Because of concerns that lipid-lowering medications may affect study results, we performed a subanalysis omitting study participants who reported current use of any prescription lipid-lowering or lipid-controlling medication. Additionally, subanalysis of the individuals with dyslipidemia, as defined by the National Cholesterol Education Program Adult Treatment Panel III criteria 16 in at least one of the lipid markers measured was also conducted to determine if baseline cholesterol status impacted treatment efficacy.
Participants
Thirty-two apparently healthy, recreationally active, postmenopausal women between the ages of 40 and 60 years were used as participants in the study. A power calculation revealed that 16 participants per group were necessary to detect a significant difference between groups in markers of lipid lowering (LDL effect size of 20 mg/dL 11 ) given a Type I error rate of 0.05, SD of 19 mg/dL, and a power of 0.80. Participants were recruited from the Central Texas area and were considered eligible to participate in the study if they were physically active but not trained (not engaged in an exercise program involving either resistance or endurance training more than three times per week for 1 year) and postmenopausal (naturally or surgically amenorrheic >1 year prior to start of study) and could adhere to the study protocol. Exclusionary criteria included active use of hormone replacement therapy, presence of coronary artery diseases and/or other significant uncontrolled cardiovascular, renal, hepatic, gastrointestinal, mental, and endocrine disorders including diabetes mellitus, a body mass index of <19 kg/m2 or >35 kg/m2, active smoking status (within the past 3 years), an average intake of more than two alcoholic drinks per day, and/or the consumption of any dietary supplements that could affect antioxidant status (excluding multivitamins) 3 months prior to beginning the study. All eligible subjects were required to obtain medical clearance from their personal physician and sign Baylor University (Waco, TX, USA)-approved informed consent documents.
Study design
This study was conducted as a 4-week single-blind, randomized, controlled trial. Prior to randomization, the protocol included a 2-week run-in phase in which participants met with a registered dietitian and were educated and instructed to limit the amount of dairy products consumed (avoid dairy milk completely and limit dairy servings to two per day) and to avoid isoflavone-containing soy products. This was done in attempt to minimize baseline dietary differences between groups with regard to dietary treatments. At this time, participants also provided a 24-hour baseline dietary recall to the registered dietitian so that baseline protein intake could be assessed using the Food Processor Dietary Assessment Software program (ESHA Research Inc., Salem, OR, USA).
After the run-in phase, participants were then scheduled to report to the Exercise & Sport Nutrition Laboratory at Baylor University for baseline testing. This testing session included personal and medical questionnaires, height and weight measurements, blood sampling, dietary intake assessment, and aerobic fitness (maximal oxygen uptake [VO2 max]) testing by performing a cardiopulmonary graded exercise test on a treadmill ergometer (Quinton, Inc., Bothell, WA, USA). After the testing session, participants were matched based on baseline protein intake and cardiopulmonary fitness level, as both have been shown to affect circulating blood lipids, 7,17,18 and were randomly assigned to consume three servings of either soymilk or dairy milk per day for 28 days. The milk was provided to the participants in black bags labeled “A” or “B” in such a way that investigators were blinded to treatment order. Participants were instructed to return to the Exercise & Sport Nutrition Laboratory 2 weeks into the supplementation period, to pick up additional milk, and again at 4 weeks, for follow-up testing including the same battery of tests performed at baseline with the exception of the aerobic fitness test.
Milk products
Both milk products were provided by WhiteWave Foods, Inc. (Broomfield, CO, USA). The soy product was the Silk® brand very vanilla flavored soymilk, and the dairy product was the Horizon® brand reduced-fat organic dairy milk. The commercial beverages were matched as closely as possible for fluid volume, total caloric, and macronutrient intake. Nutrient profiles of the milk beverages obtained from the nutrition facts panel are shown in Table 1. Because the milk products were not matched based upon dietary fat or cholesterol intake and because slight alterations in macro- and micronutrient intake were likely over the 4-week supplementation period (despite instructions to maintain a similar diet to baseline), equations were used to predict changes in TC 19 and LDL. 20 The prediction equations used dietary intake of saturated and polyunsaturated fat and cholesterol to predict changes in plasma cholesterol values.
Dietary intake
To assess dietary intake, each participant was asked to keep 4-day dietary records at baseline and during the second half of the 4-week supplementation period. The dietary records were then analyzed using the Food Processor Dietary Assessment Software program. In an attempt to determine compliance with the milk supplementation protocol, each participant was instructed to keep a compliance log of daily milk ingestion to be submitted to investigators at the 4-week testing session. Authors of similar studies 21,22 have suggested the standard of compliance is between 80% and 100%; thus, a threshold of <80% consumption of the prescribed supplement was defined as “non-compliant” a priori. Finally, a reported side effects questionnaire was administered at baseline and at 2 and 4 weeks to determine if any significant negative side effects occurred during the course of the study because of the dietary supplementation.
Plasma lipid assessment
Fasting venous blood samples were obtained before and after the supplementation period from the antecubital vein into a 10-mL collection tube using a standard Vacutainer™ apparatus (BD, Franklin Lakes, NJ, USA). Blood samples were allowed to stand at room temperature for 10 minutes and then centrifuged. For each sample, the plasma was removed and frozen at −80°C for later analysis. Plasma HDL, LDL, TG, and TC levels were then assessed by a trained technician using the Dimension RxL Clinical Chemistry System (DADE Behring Inc., Deerfield, IL, USA).
Statistical analysis
Baseline demographic, health, and dietary characteristics were summarized as sample mean and SD values. Means between groups were compared using independent t tests to assess the adequacy of our randomization scheme. Study compliance, defined as the percentage of prescribed beverage consumed, was assessed across groups using a two-sample Wilcoxon rank-sum test as these data were demonstrably non-normal.
We analyzed the reported dietary intake variables to evaluate the potential confounding effects of certain nutritional variables known to interact with plasma lipid levels. We then compared means across groups at baseline using univariate t tests, and, using repeated-measures analyses of variance on each variable, we assessed the effect of the time/intervention on the dietary intake.
Group-specific means were compared for the primary study outcome for the full analysis and subgroup analyses using a multivariate analysis of variance. The outcome of within-individual change from baseline was assessed using a repeated-measures analysis of variance; specifically of interest is whether a group × time interaction was statistically significant. We then repeated these analyses using the univariate outcome of plasma TC and the change in plasma TC from baseline. All numerical summaries and statistical comparisons were conducted using SAS version 9.1.3 (SAS Institute, Cary, NC, USA), and the Type I error rate (α) was held constant at 0.05 for all tests.
Results
Study population
Recruitment for this study began September 2008, and participant testing ended December 2008. A total of 33 individuals who met entrance criteria were recruited to begin the study. Baseline blood work for one participant was unable to be collected because of an early non-intervention-related dropout, leaving 32 participants retained for analysis. Baseline demographics for the 32 individuals who completed the study are found in Table 2. No statistically significant differences were observed in any of these variables between treatment groups. Additionally, no significant weight changes were observed during the course of the intervention (P = .25).
Data are mean ± SD values.
Dietary compliance
According to a Wilcoxon-rank sum test, there was no statistically significant difference in compliance between the treatment groups (P = .35). Although compliance logs are often unreliable indicators of dietary adherence, results from 4-day food records analyzed post-intervention also support this conclusion. A per-protocol compliance threshold was defined as >80% supplement consumption, and only one participant was defined as non-compliant. Removing this participant from analysis yielded average compliance rate of 98% across both groups. Analysis excluding this individual from the data set revealed no significant differences with regard to the primary outcome measures; therefore, only intention-to-treat analysis is presented. Reported side effects questionnaires administered at baseline and at 2 and 4 weeks also revealed minimal and equivocal side effects between treatment groups.
Dietary intake
Dietary intake data are presented in Table 3. No differences were observed in any of the dietary variables by group prior to supplementation. A time effect across both groups was observed for kilocalories (P = .02), protein (P < .01), fat (P = .02), and saturated fat (P < .01), with all values increasing over the course of the intervention. Although discrepancies did exist in the supplement nutrient profiles, dietary intake analysis did not reveal statistically significant caloric or macronutrient differences between groups post-intervention. Saturated fat values were found to be elevated in the dairy group overall (P = .05), and a significant group × time interaction was noted for fiber (P < .01) and cholesterol (P = .02).
Data are mean ± SD values.
Denotes significant differences from baseline (P < .05).
Denotes a significant group effect (P < .05).
Denotes significant group × time interaction (P < .05).
According to the predictive equation by Keys, 19 the predicted change in TC was an overall increase in both the soy and dairy groups, with no significant difference observed between groups (2.54 ± 0.28 vs. 1.73 ± 0.32 mg/dL, respectively; P = .61). Based on the equation of Hegsted et al., 20 the predicted change in LDL was significantly different between the soy and dairy groups, with the soy group having a projected decrease versus a projected increase in the dairy group (-1.51 ± 0.24 vs. 1.65 ± 0.26 mg/dL, respectively; P = .02).
Plasma lipid outcomes
Figure 1 displays final plasma lipid markers post-intervention by treatment group. No statistically significant differences were observed between groups (soy vs. dairy) with regard to TG (105.94 ± 72.79 vs. 112.38 ±62.79 mg/dL), LDL (111.44 ± 30.38 vs. 122.56 ± 33.48 mg/dL), or HDL (62.69 ± 13.29 vs. 68.13 ± 15.32 mg/dL) values post-intervention (P = .45). Likewise, no changes were observed from baseline (P = .83). Because total plasma TC is a linear combination of LDL, HDL, and other lipid components, it was assessed separately. No changes were observed post-intervention (195.88 ± 35.28 vs. 213.50 ±40.50 mg/dL; P = .19) or from baseline (P = .92).
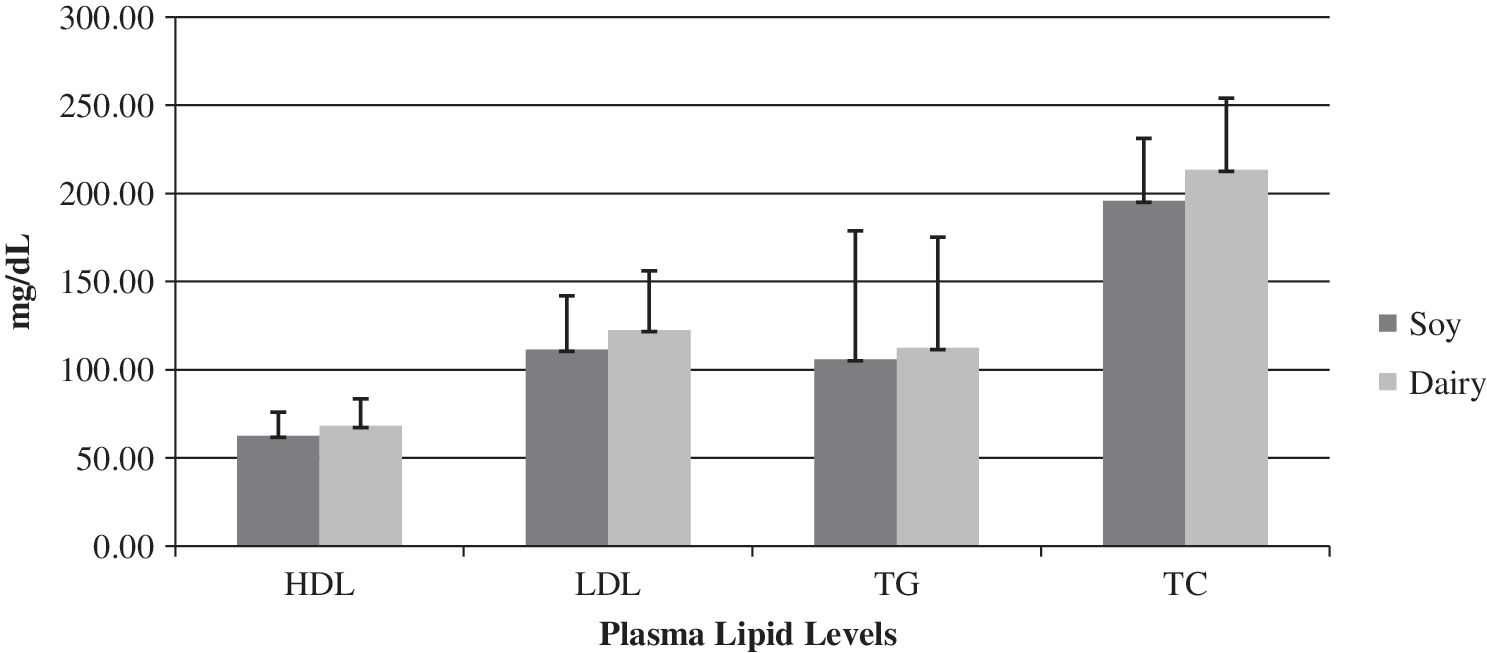
Final plasma lipid markers after 4 weeks of milk supplementation by treatment group.
To preserve the original randomization scheme, participants reporting active use of cholesterol-lowering medication were retained for the initial analysis. However, because of the potential for confounding, a subanalysis was performed excluding four participants who reported use of cholesterol-lowering medications on medical history questionnaires (n = 28). Such an analysis did not significantly alter the change in lipid values from baseline (TG, LDL, and HDL, P = .69; TC, P = .97) or post-intervention between groups (TG, LDL, and HDL, P = .68; TC, P = .41). Additional subanalysis of those individuals with dyslipidemia (n = 23) did not reveal any significant changes in TG, LDL, or HDL from baseline (P = .92) or post-intervention between groups (P = .74). Likewise, TC remained unchanged (P = .95 change from baseline and P = .57 post-intervention).
Discussion
In this 4-week intervention study, we failed to find a significant hypocholesterolemic effect of soymilk consumption in a postmenopausal female population, despite good reported compliance with the dietary protocol. Although discussion of the plausible factors contributing to this nonsignificant result is warranted, it is first prudent to reflect on these findings in the context of related clinical trials.
Several studies have shown that soymilk consumption is associated with a reduction in plasma lipid levels, especially in hypercholesterolemic patients. Gardner et al. 11 enrolled 28 hypercholesterolemic men and women in a crossover study comparing the lipid-lowering responses to two commercially available soymilks (one with appreciable amounts of isoflavones [125 ± 17 mg/day] and one without (39 ±1 mg/day]) with low-fat dairy milk. After 4 weeks of intervention, results showed that consumption of soymilk was associated with a modest reduction in LDL cholesterol compared to low-fat dairy milk, regardless of isoflavone content. Interestingly, results from a previous study of similar design 23 suggest that the isoflavone-containing fraction is an important factor in the lipid-lowering properties of soy products, with the authors reporting a significant increase in the total and LDL cholesterol-lowering ability of a soy protein plus isoflavone beverage compared to a beverage prepared solely with isolated soy protein.
Two other studies worthy of note also examined the lipid-lowering potential of soymilk consumption in hypercholesterolemic patients. 12,13 Bricarello et al. 12 recruited 60 hypercholesterolemic men and women, between the ages of 20 and 70 years, to consume either soy or nonfat dairy milk at 1 L/day for 6 weeks. No effect of soymilk was observed for TC and TG, but soymilk consumption reduced plasma LDL cholesterol and increased HDL cholesterol compared to baseline and the dairy milk group. Conversely, when 16 hypercholesterolemic men and women participated in a crossover study in which diets were supplemented with either 500 ml/day dairy or high-glycitein soymilk for 4 weeks, no statistical differences from baseline and between dietary groups was observed for any cholesterol values. 13
Lastly, in a randomized trial that compared the effects of soy proteins from differently processed products with animal protein on a variety of CVD risk factors, 14 no difference was observed between groups in any of the cardiovascular outcomes assessed. Furthermore, a separate analysis of the soymilk-based diet (i.e., included plain soymilk, plain soy yogurt, and tofu) revealed a significantly greater lipid-modulating potential (4% decrease in LDL cholesterol) than the other experimental diets relative to the animal-protein diet.
Given our findings and the inconsistencies in the literature regarding the lipid-lowering potential of soyfoods, it is of further interest to explore what factors may have contributed to this nonsignificant result. Baseline cholesterol status, supplement type, dosage, and duration, as well as dietary control, are all potential confounding agents that have been identified and are discussed below.
Baseline cholesterol status
It is recognized that the extent of cholesterol lowering by soy may be dependent on initial plasma levels, 6,7 with some studies suggesting that definitive hypocholesterolemic effects only occur in patients with significant hypercholesterolemia (TC values of ≥ 270 mg/dL). 7 In an attempt to control for baseline cholesterol values, a subanalysis of our dataset was performed, including only those individuals with some form of dyslipidemia as defined by the National Cholesterol Education Program Adult Treatment Panel III criteria 16 (n = 23), although doing so did not significantly alter the results. However, in our entire cohort, the highest baseline TC level was 250 mg/dL; therefore, it is possible that baseline plasma TC levels may not have been sufficiently elevated to observe a significant reduction. Despite this line of reasoning, it should be noted that recent results suggest that hypocholesterolemic effects of soymilk can be seen in normolipidemic subjects. 15
Supplement dosage
Another reason for the nonsignificant finding of this study could be due to the type and amount of soy provided. Although multiple studies have reinforced the need for combined isoflavone and soy protein consumption to obtain more favorable cardioprotective benefits, perhaps we did not supply participants with enough of either or both to see a pharmacologic effect. At present, the Food and Drug Administraiton health claim states that consumption of 25 g of soy protein/day is needed to see a reduction in the risk of heart disease. In our study (assuming an average of 98% compliance with the dietary protocol), total soy protein consumed by the soymilk group was roughly 18 g/day. Although more recent studies suggest that as little as 20 g of soy protein/day can lower non-HDL cholesterol and have favorable cardiovascular effects, 24 the possibility remains that the amount of soy protein provided in approximately 3 cups of soymilk per day was not enough to significantly improve blood lipid levels. In terms of isoflavone content, recent meta-analyses support the notion that intakes of soy protein coupled with isoflavone above 40 mg/day have lipid-lowering effects. 6 Although the isoflavone content of the soymilk used was not analyzed, Gardner et al. 11 used a similar product and showed that 3 cups of soymilk supplies approximately 90 mg of isoflavones, although the content per sample was noted to be highly variable. Despite this, it is likely that our study design provided a sufficient amount of isoflavones to potentiate a reduction in cholesterol levels. Lastly, the possibility remains that in spite of reported dietary compliance, participants may not have adhered to the study protocol, rendering intake insufficient. Unfortunately, because of funding restraints we were unable to analyze blood or urinary isoflavones and were dependent on participant truthfulness in compliance reporting. We implore the need for future studies to assess these markers with more objective indicators of compliance as a means of process evaluation.
Time course of administration
Although the amount of time allotted for supplementation in our study was comparable to 11 or only slightly shorter in duration than 12,13 other studies observing favorable outcomes, our study failed to find a significant result. Results from the meta-analysis performed by Zhan and Ho 6 suggest that the strongest lowering effects of soy protein containing isoflavones on TC, LDL, and TG occurs within the short initial period of intervention (≤6 weeks). Therefore, it is likely that our study was of sufficient duration to see initial improvements in these specific markers. HDL improvements, however, appear to require a longer intervention period as Zhan and Ho 5 found that increases in HDL cholesterol were only observed in studies of greater than 12 weeks of duration.
Dietary control
This study was conducted in free-living individuals. Although this may have hindered protocol adherence, dietary and compliance analysis suggests that it did not. All dietary variables included in this analysis were similar by group at baseline, but there were significant changes in select dietary variables at 4 weeks. The increases observed across both groups for kilocalories, protein, fat, and saturated fat across time were likely due to the intervention itself as participants in these types of studies often do not reduce dietary intake to account for supplemental intake. However, while this increase could confound the plasma lipid changes from baseline, it would not explain the lack of difference between groups post-intervention. Conversely, the overall increased amount of saturated fat intake observed in the dairy group (particularly post-intervention) as well as the group × time interaction for fiber and cholesterol intake may explain the nonsignificant post-intervention findings with regard to plasma lipids, although this is quite speculative.
Attempts were made to control for dietary fat intake by using predictive equations. No changes in TC were projected based upon dietary intake of saturated and polyunsaturated fat and cholesterol, but it was predicted that the soy group would have a decrease in LDL, while the dairy group would observe an increase in LDL. Unfortunately, these predictive equations do not incorporate other dietary variables associated with alterations in plasma cholesterol, such as fiber or select antioxidants. Additionally, error with the use of predictive equations also exists. Similar to our results, a meta-analysis examining the effects of dietary fat on serum cholesterol found that the predicted TC and LDL levels were significantly lower on a high polyunsaturated diet relative to a high monounsaturated fat diet; however, the observed lipid differences were not significant. 25 Finally, it is possible that inaccuracies in using a 4-day dietary record to assess food intake confounded our results. Dietary records are considered accurate for estimating stable dietary components, such as total kilocalories and percentage of macronutrients, but more variable nutrients such as dietary cholesterol may require 2–3 weeks of recording to accurately estimate intake. 26
Conclusions
In light of increasing use, it is important to understand the health effects of soymilk. Although numerous studies have reinforced the need for combined isoflavones and soy protein consumption to obtain favorable cardioprotective benefits, our study failed to show an improvement in the lipid profile. Future research should seek to clarify the biological mechanism responsible for the lipid-lowering benefit of soyfoods, as well as the importance of study population characteristics, intervention type, dosage, and time course of soyfood consumption necessary to achieve a significant improvement in lipid profiles.
Footnotes
Acknowledgment
We would like to thank Dr. Mark J. Messina for thoughtfully reviewing this manuscript and significantly contributing to its completion.
Author Disclosure Statement
The authors have no relevant financial relationships to disclose. Funding for this study was provided by WhiteWave Foods, Inc. (Broomfield, CO, USA).