
Abstract
The present study was examined the effects of xylitol feeding on diabetes-associated parameters in nondiabetic rats. Seven-week-old male Sprague–Dawley rats were randomly divided into three groups: control (five rats), sucrose (six rats), and xylitol (six rats). Animal had free access to a commercial rat pellet diet, and ad libitum water, 10% sucrose solution, and 10% xylitol solution were supplied to the control, sucrose, and xylitol groups, respectively. After 3 weeks of feeding of experimental diets, food intakes were significantly (P<.05) lower in the sucrose and xylitol groups compared with the control group. Drink intake was significantly higher in the sucrose group but significantly lower in the xylitol group compared with the control group. Body weight gain was significantly lower in the xylitol group compared with the sucrose group. Weekly nonfasting blood glucose was significantly increased, but fasting blood glucose was significantly decreased, in the sucrose group compared with the control and xylitol groups. Significantly better glucose tolerance was observed in the xylitol group compared with the control and sucrose groups. Serum insulin and fructosamine concentrations were not significantly influenced by the feeding of xylitol or sucrose. Relative liver weight and liver glycogen were significantly increased in the xylitol group compared with the sucrose group, whereas no difference was observed between the xylitol and control groups. Serum total cholesterol and low-density lipoprotein-cholesterol were significantly decreased in the sucrose and xylitol groups, and serum triglyceride of the xylitol group, but not the sucrose group, was significantly increased compared with the control group. Data of this study suggest that xylitol can be a better sweetener than sucrose to maintain diabetes-related parameters at a physiologically safer and stable condition.
Introduction
S
Xylitol is a white crystalline five-carbon sugar alcohol usually manufactured by the hydrogenation of its precursor, xylose. It is widely used as a nonsugar sweetener or sugar substitute in various food products because of its nearly similar sweetness but relatively lower caloric value (2.4 kcal/g) compared with sucrose (4.0 kcal/g). 23 About 50% of xylitol is absorbed in the small intestinal tract, whereas the rest of it enters into the large intestine for fermentation by bacteria. 2 Numerous recent and previous studies have confirmed the effects of xylitol in the prevention of dental caries, plaque, and oral biofilm formation in both children and adults. 24 –27 It has been reported that daily consumption of 5–10 g of xylitol with different vehicles can reduce dental caries by up to 82%. 28 –33 Therefore, the use of xylitol is gradually increasing in those products that are especially popular among young children, who are particularly susceptible to dental caries. In a recent report, it has been recommended that chewing a xylitol-containing gum after a meal, instead of brushing, is effective in preventing possible dental caries; 34 xylitol is recommended as a powerful preventive weapon against dental caries in this report. Habitual use of a relatively smaller amount of polyol-containing chewing gum by young children significantly reduced the growth of mutans streptococci and dental plaque. 16 In this case, xylitol was found to be more effective than some other widely used sugar alcohols. Maternal use of xylitol-containing chewing gum also significantly reduced the mother–child transmission of salivary mutant streptococci. 15 Higher intakes and higher dosages of most of the sugar alcohols cause several gastrointestinal discomforts or diarrhea, but xylitol has been reported as a safer sugar alcohol compared with others. Besides the excellent effects of xylitol on oral healthcare, the effects of xylitol on glycemic control has also been reported in several previous studies. 35 –39
Hassinger et al. 35 reported that the requirement of insulin to control blood glucose is significantly lower for xylitol compared with the same amount of calorie-containing starch or sucrose in insulin-dependent diabetic subjects. Additionally, xylitol has a significantly lower glycemic index (13) compared with sucrose (65) and glucose (100), 2 and recently there has been a growing interest in low glycemic index food for reduction of diabetic hyperglycemia. 40,41 Several previous studies have also reported the significantly lower glycemic and insulinemic response after the consumption of 20–50 g of xylitol compared with sucrose in normal human subjects. 36 –39 However, the overall antidiabetic effects of xylitol as a sugar replacement on diabetes-associated parameters have not yet been investigated in either normal or diabetic humans or experimental animals.
The present study was performed to examine the overall effects of xylitol as a sugar replacement on diabetes-associated parameters in nondiabetic rats.
Materials and Methods
Animals
Seventeen 7-week-old male Sprague–Dawley rats were obtained from the Biomedical Resource Center of the University of KwaZulu-Natal, Westville Campus, Durban, South Africa. Animals were randomly divided into three groups: control (five rats), sucrose (six rats), and xylitol (six rats). They were housed in a maximum of three in one medium polycarbonated cage in a temperature- and humidity-controlled room with a 12-hour light–dark cycle. Animals were maintained according to the rules and regulations of the University of KwaZulu-Natal Animal Ethics Committee.
Xylitol and other chemicals and reagents
The pure xylitol was kindly donated by a local South African company, Sweet Nothings (Pietermaritzburg, South Africa). Sucrose was purchased from the local supermarket, and other chemicals and regents were obtained from different local and international chemical companies.
Feeding and monitoring weekly body weight and blood glucose level
Animals had free accessed to a commercially available rat chow diet and the respective experimental drinks ad libitum during the 3-week experimental period. Animals in the control, sucrose, and xylitol groups were supplied ad libitum with drinking water, 10% sucrose solution, and 10% xylitol solution, respectively. Food and drink intakes were measured daily, and body weight changes and blood glucose concentrations were measured in a weekly basis. The weekly nonfasting or fasting blood glucose (NFBG and FBG, respectively) concentration of each animal was measured in a drop of blood collected from the tail vein by using a portable glucometer (GlucoPlus Inc., Saint-Laurent, Canada) with a maximum measuring capacity of 600 mg/dL.
Intraperitoneal glucose tolerance test
In order to measure the glucose tolerance level, the intraperitoneal glucose tolerance test (IPGTT) was performed in each animal in the last week of the 3-week experimental period. In brief, after intraperitoneal injection of a glucose solution (2.0 g/kg of body weight) to fasted animals, subsequent glucose concentrations were measured in the blood collected from tail veins at 0 (just before glucose injection), 30, 60, 90, and 120 minutes after the glucose injection.
Collection of blood and liver
At the end of the experimental period, animals were decapitated while under halothane anesthesia, and blood and liver samples were collected. The whole blood of each animal was collected in a 14-mL Falcon tube (BD Biosciences, Franklin Lakes, NJ, USA) and refrigerated immediately for subsequent analysis. The refrigerated blood of each animal was centrifuged at 1,600 g for 15 minutes, and then serum was separated to individual microtubes and preserved at −30°C for subsequent analysis of serum concentrations of insulin, fructosamine, and lipids (total cholesterol, high-density lipoprotein [HDL]-cholesterol, low-density lipoprotein [LDL]-cholesterol, and triglycerides [TGs]). Liver was weighed, washed with normal saline, wiped with filter paper, and preserved at −30°C for subsequent analysis of liver glycogen concentrations.
Analytical methods and calculations
Serum concentrations of lipids (total cholesterol, HDL-cholesterol, and TGs) were measured photometrically by using commercial assay kits (lot number 9002) purchased from Labtest Diagnostica (Lagoa Santa, Brazil). The fraction of LDL-cholesterol in the serum was calculated by using the equation of Friedewald et al. 42 as follows: LDL-cholesterol (in mg/dL)=Total cholesterol − (HDL-cholesterol + VLDL), where very-LDL-cholesterol (VLDL)=TG/5.
The serum fructosamine concentration was measured photometrically by using a commercial assay kit (lot number 9002) purchased from Labtest Diagnostica. The serum insulin concentration was measured by using an ultrasensitive rat insulin enzyme-linked immunosorbent assay kit (lot number 18016) from Mercodia (Uppsala, Sweden) in a multiplate enzyme-linked immunosorbent assay reader. The liver glycogen level was measured photometrically using the phenol–sulfuric acid method proposed by Lo et al. 43
Statistical analysis
Data are presented as mean and their corresponding SDs for all animal groups. All data were analyzed statistically by using a statistical software package (Statview version 5.0, Statview, Cary, NC, USA) using the Tukey–Kramer multiple range post hoc test. Values were considered significantly different at P<.05.
Results
Food and drink intake and body weight
Data for overall food intake, weekly drink intake, and weekly body weight gains are presented in Table 1. Food intake was significantly (P<.05) lower in the sucrose and xylitol groups compared with the control group, whereas no significant difference was observed between the sucrose and xylitol groups.
Data are mean±SD values of five or six animals.
Different superscript letters present within a row indicate values are significantly different from any other group of animals (Tukey–Kramer multiple range post hoc test, P < .05).
*P < .05, ***P < .001, significantly different from the sucrose group.
Weekly drink intake was significantly higher in the sucrose group and significantly lower in the xylitol group compared with the control group. Drink intake of the xylitol group was also significantly lower than in the sucrose group.
Drink intake was significantly higher in the sucrose group compared with the control group; however, weekly body weight gains were not significantly different during the experimental period. The overall body weight gain was lower in the xylitol group compared with the sucrose group, but significant differences were observed only for week 1 and week 2 (Table 1).
Weekly blood glucose
The data for weekly NFBG and FBG concentrations are presented in Figure 1. Initial blood glucose concentrations were not significantly different. No significant difference was observed after 1 week of feeding; however, after 2 weeks of feeding, NFBG of the sucrose group was significantly higher than those of the control and xylitol groups, whereas no significant difference was observed between the control and xylitol groups. The effects of xylitol and sucrose on NFBG and FBG may not be similar. After the 3-week feeding, although FBGs of the control and xylitol groups were not significantly different, they were significantly higher than the FBG of the sucrose group.
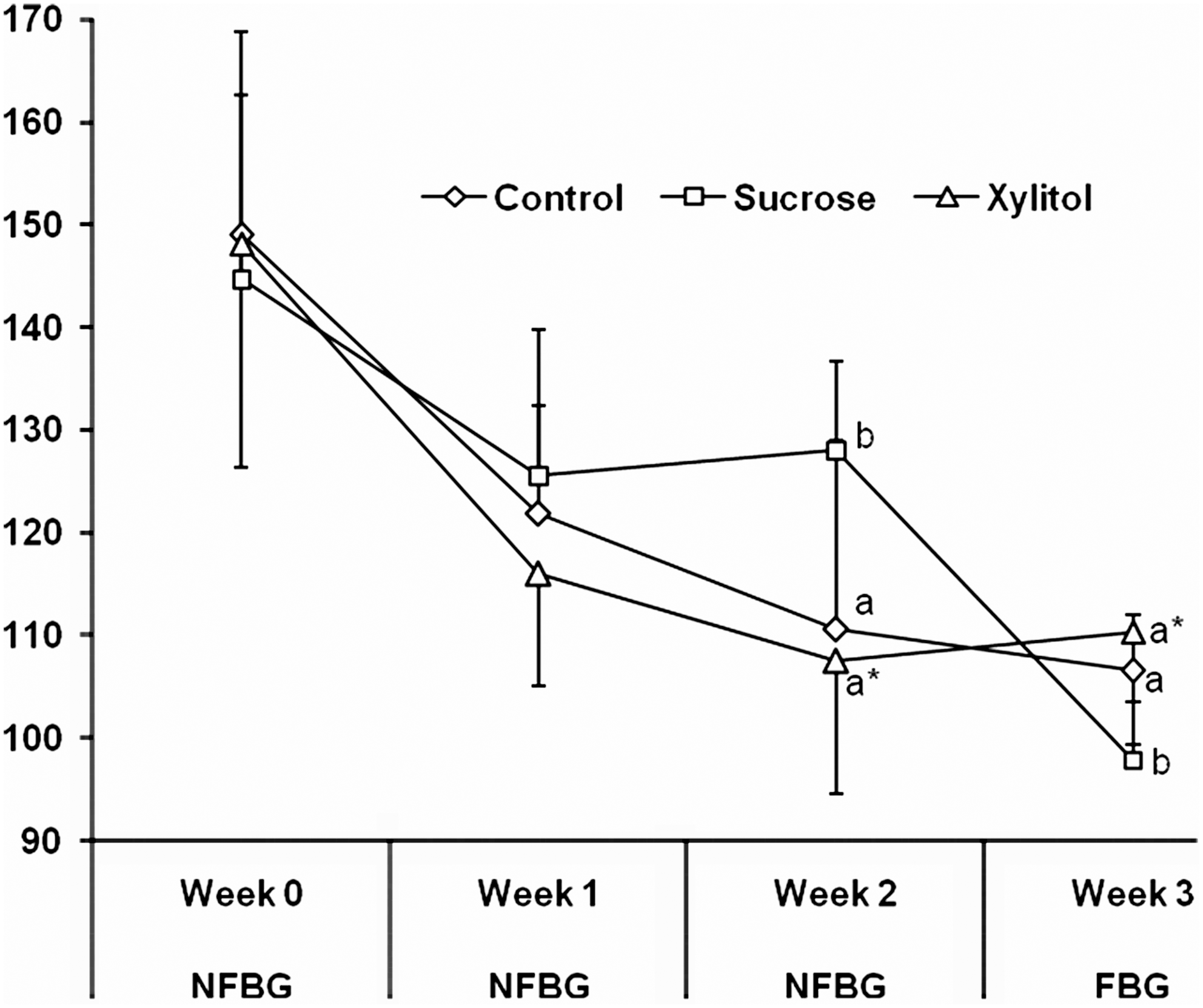
Weekly nonfasting and fasting blood glucose (NFBG and FBG, respectively) concentrations during the experimental period. Data are mean±SD values of five or six animals. abDifferent letters present near the lines for a given week indicate values are significantly different from any other group of animals (Tukey–Kramer multiple range post hoc test, P<.05). *Significantly different from the sucrose group (P<.05).
IPGTT
The IPGTT data are presented in Figure 2. This test was performed in the last week of the experimental period in all animals after an overnight fast. At 0 minute after glucose injection (fasting), there was no significant difference between the blood glucose concentrations of the control and xylitol groups; however, they were significantly higher than the blood glucose concentration of the sucrose group. Better glucose tolerance was observed for the xylitol group compared with the control and sucrose groups during the following period of IPGTT. Data were not significantly different at 30, 60, and 90 minutes after glucose injection because of high SDs between the data, but significantly better glucose tolerance was observed in the xylitol group compared with the sucrose group at 120 minutes after the glucose injection (Fig. 2).
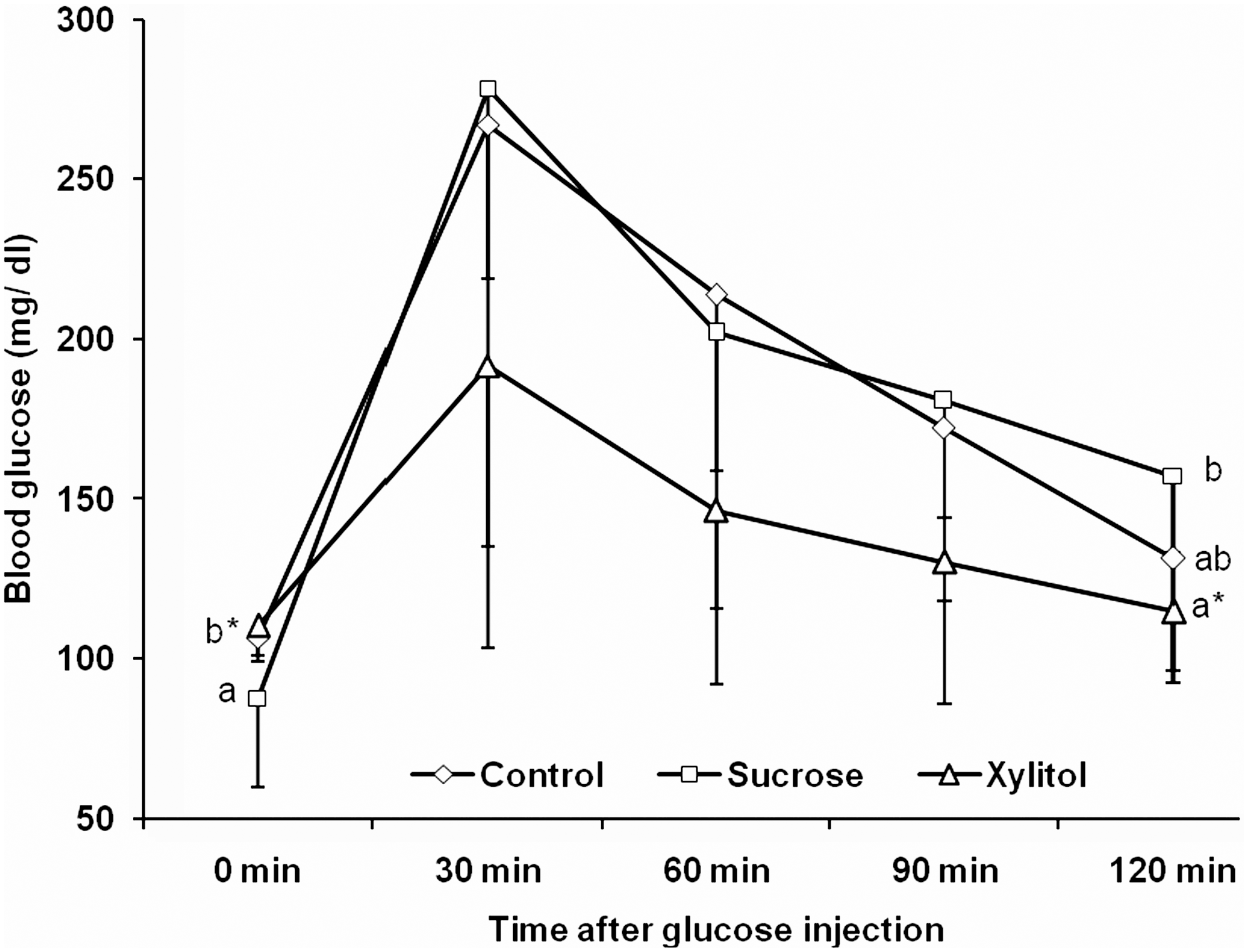
Results of the intraperitoneal glucose tolerance test in the last week of the experiment. Data are mean±SD values of five or six animals. abDifferent letters present near the lines for a given period of time indicated values are significantly different from any other group of animals (Tukey–Kramer multiple range post hoc test, P<.05). *Significantly different from the sucrose group (P<.05).
Serum insulin and fructosamine concentrations
The data for serum insulin and fructosamine concentrations are presented in Figure 3. Although data were not significantly different between the groups, relatively higher serum insulin and lower serum fructosamine concentrations were observed in the xylitol group compared with the control and sucrose groups.
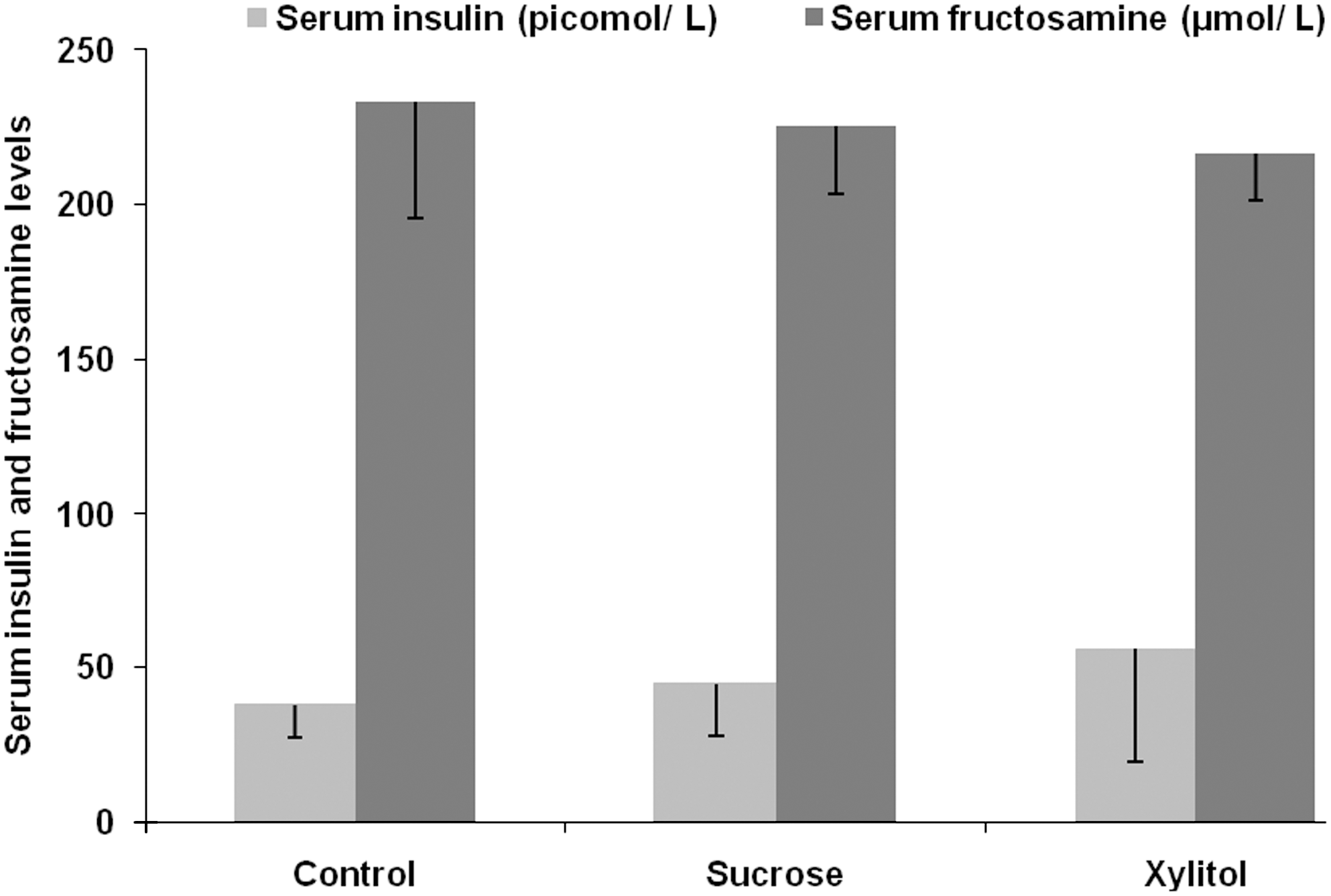
Serum insulin and fructosamine concentrations at the end of the 3-week experimental period. Data are mean±SD values of five or six animals. No statistically significant difference was observed for either serum insulin or fructosamine concentrations among the groups (P>.05).
Liver analyses
The data for liver weight, relative liver weight, and liver glycogen concentrations are presented in Figure 4. No significant difference was observed for liver weight between the groups, but the relative liver weight of the xylitol group was significantly higher than that of the sucrose group. Similarly, the liver glycogen concentration of the xylitol group was significantly higher than that of the sucrose group (Fig. 4). Although the liver glycogen concentration of the control group was markedly higher than that of the sucrose group, it was not significantly different because of high SD.

Liver weight, relative liver weight, and liver glycogen levels at the end of the 3-week experimental period. Data are mean±SD values of five or six animals. abDifferent letters present near the lines for a given period of time indicate values are significantly different from any other group of animals (Tukey–Kramer multiple range post hoc test, P<.05). *Significantly different from the sucrose group (P<.05).
Serum lipid profile
The data for serum lipid profiles are presented in Figure 5. Serum HDL-cholesterol was not affected by the consumption of sucrose or xylitol, but serum total cholesterol and LDL-cholesterol concentrations of the sucrose and xylitol groups were significantly lower compared with the control group, whereas no significant difference was observed between the sucrose and xylitol groups. Finally, serum TG concentrations of the control and sucrose groups were significantly lower than that of the xylitol group (Fig. 5).
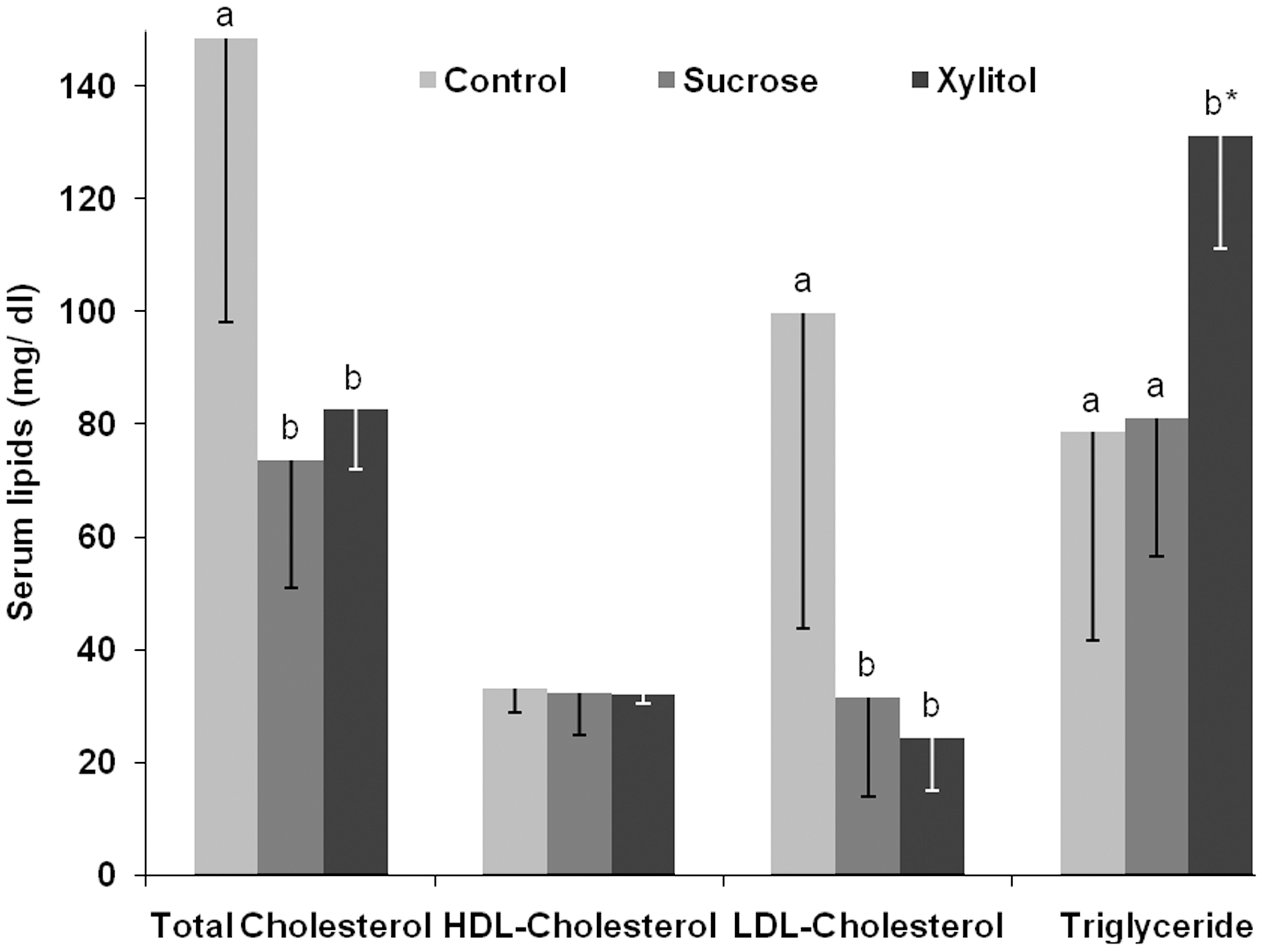
Serum lipid profile (total cholesterol, high-density lipoprotein [HDL]-cholesterol, low-density lipoprotein [LDL]-cholesterol, and triglyceride) at the end of the 3-week experimental period. Data are mean±SD values of five or 6 animals. abDifferent letters present over the bars for a given parameter indicate values are significantly different from any other group of animals (Tukey–Kramer multiple range post hoc test, P<.05). *Significantly different from the sucrose group (P<.05).
Discussion
The present study was conducted to examine the hypoglycemic antidiabetic potentials of xylitol, which is widely used as a sugar replacement in various food products. A considerably lower dose of xylitol (10% solution) was given to the nondiabetic rats instead of drinking water, and 10% sucrose solution was supplied to the sucrose group. The data of this study suggest that xylitol has some significant antidiabetic effects. Nondiabetic animals have been used initially to examine whether xylitol has overall potentials to ameliorate diabetes-associated parameters or not. Based on the results of this study, our further research on the antidiabetic effects of xylitol in the type 2 diabetes model of rats is currently being conducted in our laboratory.
Food intake was not significantly different between the sucrose and xylitol groups, but drink intake and body weight were significantly increased in the sucrose group compared with the xylitol group (Table 1). Duration of gastric emptying and food intakes are closely associated with each other: a longer gastric emptying time can significantly reduce the food intake compared with a shorter gastric emptying time, and vice versa. It has been reported that feeding of xylitol significantly prolonged gastric emptying time but decreased food intake compared with glucose, fructose, or sucrose in normal human volunteers. 44 Our results completely support the results of this previous study. In our study, relatively lower food intake and significantly lower drink intake in the xylitol group compared with the sucrose group might be due to the lower gastric emptying in the former group compared with the latter. At the same time, lower food and drink intakes are directly related to the lower calorie intake as well as the lower body weight gain that was found in the xylitol group compared with the sucrose group in our study (Table 1).
It has been determined that about 50% of xylitol is absorbed in the small intestinal tract, whereas the rest of it enters into the large intestine for fermentation by bacteria. 2 Because of the lower small intestinal absorption and slower gastric emptying of xylitol compared with sucrose, 44 the rate of induction of blood glucose will not be similar between these two compounds. In our study, the significantly lower NFBG concentration in the xylitol group compared with the sucrose group might be due to the above-mentioned reasons. At the end of the 3-week experimental period, although the FBG level was significantly lower in the sucrose group (97.83±5.71 mg/dL) compared with the xylitol group (110.33±11.04 mg/dL), the FBG level of the xylitol group was not significantly different from that of the control group (106.60±5.37 mg/dL) (Fig. 1). These blood glucose data suggest that xylitol could maintain both the NFBG and FBG levels in a physiologically safer and significantly better stable condition compared with sucrose. Additionally, the significantly better glucose tolerance ability of the xylitol group compared with the sucrose group also confirmed that xylitol has significantly better effects in blood glucose and diabetes management compared with sucrose (Fig. 2). Thus, xylitol has better potential to reduce and maintain the NFBG and FBG levels at a physiologically safer state compared with sucrose.
After several in vitro studies on isolated islets of Langerhans from rats, it has been reported that the mode of action of xylitol on insulin secretion may be different from that of glucose. 45 However, a recent study 46 reported that the intravenous administration of xylitol (0.1 g/kg of body weight) appeared to cause secretion of insulin similar to that caused by glucose in nonlactating cattle.
It has been reported that giving a single oral dose of xylitol (30 g) produced only a minimal rise in blood glucose level but no rise in serum insulin concentration in healthy human subjects. 39 However, in another study, Muller-Hess et al. 47 reported that either 30 or 50 g of oral xylitol caused a small but statistically significant increase in blood glucose and plasma insulin concentrations in normal human subjects. Kuzuya et al. 48 have studied the effects of several compounds, including glucose and xylitol, on insulin release followed by their injection into the pancreatic artery of dogs and reported that xylitol produced a slower insulin release than glucose; on the other hand, when xylitol or glucose was given by constant infusion into a systemic vein for 50 minutes in dogs, then the plasma insulin level was higher for xylitol compared with glucose infusion. 49 Hence, the effect of xylitol on insulin secretion is different from species to species and also depends on several factors such as dose, route of consumption, etc. On the other hand, no report has been found on the effect of xylitol on serum fructosamine concentration. In this study, the relatively, but not significantly, higher serum insulin concentration and relatively lower serum fructosamine concentration in the xylitol group compared with the sucrose and control groups revealed that the insulinemic value of xylitol is lower than that of glucose. 2 Results of this study support the results of several above-mentioned previous studies in this regard.
Lower hepatic glycogen is a common pathogenesis during the hyperglycemic or diabetic condition due to higher glycogenolysis or gluconeogenesis and lower insulin concentration. 50 In this study, the almost same and significantly higher liver glycogen concentrations in the control and xylitol groups, but different from that of the sucrose group, confirm the glucose-lowering activity of xylitol in nondiabetic rats (Fig. 4). The significantly better glucose tolerance level in the xylitol group compared with the sucrose group also supports this effect of xylitol (Fig. 2).
Consumption of xylitol did not significantly influenced the level of total, HDL-, and LDL-cholesterol compared with the sucrose group, but the significantly higher concentrations of total and LDL-cholesterol and significantly lower concentration of TG in the control group compared with the xylitol group (Fig. 5) revealed that most of the cholesterol of the xylitol group might be converted into TG. It has been also reported that postprandial serum TG was significantly increased in a xylitol formula–consuming group compared with a fiber-free formula–consuming group in healthy human subjects. 51 The result for serum TG of this study is also consistent with the results of the above-mentioned report.
In summary, data from this study suggest that xylitol not only reduces the blood glucose concentration but also significantly improves the glucose tolerance level compared with sucrose in nondiabetic rats. Significantly lower food intake and relatively lower body weight gain in the xylitol group compared with the control and sucrose groups confirm that xylitol can also be used as an appetite-suppressing sugar substitute for patients with overweight- and obesity-related metabolic diseases. Therefore, xylitol can be a better sweetener than sucrose to maintain the diabetes-related parameters at a physiologically safer and stable condition.
Footnotes
Acknowledgment
This study was supported by a Competitive Research Grant from the Research Office, University of KwaZulu-Natal, Westville Campus, Durban, South Africa.
Author Disclosure Statment
No competing financial interests exist.