
Abstract
Cinnamon, the dry bark and twig of Cinnamomum spp., is a rich botanical source of polyphenolics that has been used for centuries in Chinese medicine and has been shown to affect blood glucose and insulin signaling. Cinnamon's effects on blood glucose have been the subject of many clinical and animal studies; however, the issue of cinnamon intake's effect on fasting blood glucose (FBG) in people with type 2 diabetes and/or prediabetes still remains unclear. A meta-analysis of clinical studies of the effect of cinnamon intake on people with type 2 diabetes and/or prediabetes that included three new clinical trials along with five trials used in previous meta-analyses was done to assess cinnamon's effectiveness in lowering FBG. The eight clinical studies were identified using a literature search (Pub Med and Biosis through May 2010) of randomized, placebo-controlled trials reporting data on cinnamon and/or cinnamon extract and FBG. Comprehensive Meta-Analysis (Biostat Inc., Englewood, NJ, USA) was performed on the identified data for both cinnamon and cinnamon extract intake using a random-effects model that determined the standardized mean difference ([i.e., Change 1control – Change 2cinnamon] divided by the pooled SD of the post scores). Cinnamon intake, either as whole cinnamon or as cinnamon extract, results in a statistically significant lowering in FBG (–0.49±0.2 mmol/L; n=8, P=.025) and intake of cinnamon extract only also lowered FBG (–0.48 mmol/L±0.17; n=5, P=.008). Thus cinnamon extract and/or cinnamon improves FBG in people with type 2 diabetes or prediabetes.
Introduction
O
Animal and in vitro studies have consistently shown that cinnamon powder or extracts improve insulin sensitivity and insulin signaling by increasing tyrosine phosphorylation activity and by decreasing phosphatase-mediated insulin receptor inactivation. 6 Cinnamon extract has been reported to reduce blood glucose, plasma insulin, triglycerides, and total cholesterol in fructose-fed rats 7 and more recently to do so while altering plasma adipose-derived factors and expression of multiple genes related to carbohydrate metabolism and lipogenesis in adipose tissues. 8 In the db/db mouse, a methanol extract of cinnamon improved FBG, decreased hepatic free fatty acids, and increased serum insulin and adiponectin. 9 A recent short-term study in healthy human subjects showed lower postprandial blood glucose concentrations and improved insulin sensitivity when 5 g of cinnamon was eaten 12 hours before or ingested at the same time as an oral glucose tolerance test was performed. 10 In a small pilot trial, cinnamon extract also lowered homeostasis model of assessment–insulin resistance in women with polycystic ovary syndrome. 11 The long-term effects of cinnamon consumption in human subjects have not been studied; however, its use as a spice for thousands of years suggests that any adverse effects of long-term use are likely minimal, although high doses of whole cinnamon may be of concern. For example, concerns about coumarin intake with high doses of Cinnamomum cassia have been raised and evaluated. 12 The total dietary intake for a 70-kg individual for aqueous cinnamon extracts is less than 7% of the maximum recommended daily dose, as coumarin is poorly soluble in water but can reach as high as 64% of the maximum recommended daily dose for some powder supplements.
Several clinical trials using modest sample populations have investigated the impact of cinnamon or cinnamon extract on FBG. In 2008, Baker et al. 13 published a meta-analysis of five clinical studies and concluded that the intake of cinnamon did not significantly alter FBG. However, in a 2009 review by Kirkham et al., 14 the evidence was considered as inconclusive as to whether cinnamon reduced FBG. Since 2008, three additional clinical studies have been published as well as positive animal studies supported by new molecular mechanisms for cinnamon. These events have led us to again analyze the clinical data available. We have extracted the results from the studies identified that met our inclusion criteria and then performed a meta-analysis on those clinical study results. The meta-analysis was performed using a random-effects model, and the results of the meta-analysis of the larger number of clinical studies show that consuming cinnamon, especially cinnamon extract, does produce a modest but statistically significant lowering in FBG.
Materials and Methods
To be included in this meta-analysis, human trials had to be randomized, placebo-controlled using cinnamon and or cinnamon extract and report data on FBG. Literature searches were done in Biosis and Pub Med and using key words related to “cinnamon” and “glucose” in May 2010. In addition, we searched the 2010 abstracts for the American Diabetes Association and Federation of American Societies for Experimental Biology. Comprehensive Meta-Analysis (Biostat Inc., Englewood, NJ, USA) was used to analyze the data. We calculated standardized mean difference and 95% confidence intervals using standardized mean difference (i.e., Change 1 – Change 2) divided by the pooled SD of the post scores. This approach was adopted as the data, as reported by various studies selected, provided neither the pre–post correlation of the results nor the raw data necessary to compute this number. Pre–post correlation is required in the meta-analysis to allow the computation of variance used to weight each study and compute the variance of the combined effects. In addition, funnel plot analysis was undertaken to assess for possible publication bias effects.
Results
The results of the literature search up to 2010 were substantially similar, and we used (Table 1) those detailed by Baker et al. 13 except Altschuler et al. 15 and as well as the same ones identified by Kirkham et al. 14 except Suppapitiporn and Kanpaksi, 16 which was only accessible as an abstract with no discrete glucose data for any of their groups. We also identified but did not use the report of Altschuler et al. 15 or any of the reports from Crawford, 17 Solomon and Blannin, 18 Mettler et al., 19 or Wang et al. 11 for analysis in this study: the latter four studies were not used as they did not discretely report FBG levels, and Altschuler et al. 15 was not used as it was done in type 1 diabetics, and cinnamon decreases insulin resistance, which is not a mechanism of type 1 diabetes. The series of studies by Hlebowicz and co-workers, 10,20,21 while demonstrating acute postprandial effects, were not included because long-term effects of cinnamon were not studied. Of the cinnamon studies 10,11,18 –21 identified that were nonqualifying because of being either acute or the absence of FBG data, all reported an effect of cinnamon on glucose or a glucose metabolism-related parameter.
The characteristics of the studies included are summarized (Table 2) as to the type of subject, cinnamon used, dosage and schedule, study duration, number of subjects, and mean FBG and SD in the cinnamon and control groups for each of the studies. All studies reported the use of C. cassia except for that of Tang et al., 27 which did not specify the species.
FBG, fasting blood glucose.
The eight studies whose data were used for this meta-analysis include Khan et al., 23 Roussel et al., 25 Mang et al., 24 Ziegenfuss et al., 29 Blevins et al., 22 Vanschoonbeek et al., 28 Tang et al., 27 and Stoecker et al. 26
The study by Khan et al. 23 showed that the ingestion of 1, 3, or 6 g of cinnamon daily for 40 days lowered concentrations of FBG in women and men with type 2 diabetes already receiving oral blood glucose-lowering treatment.
The study of Roussel et al. 25 had 22 subjects with impaired FBG with a body mass index ranging from 25 to 45 kg/m2 who were given capsules containing either a placebo or 250 mg of an aqueous extract of cinnamon two times per day for 12 weeks.
Mang et al. 24 reported the results for a total of 79 mixed gender patients with diagnosed diabetes mellitus type 2, not on insulin therapy but treated with oral antidiabetics or diet, who were randomly assigned to take either a cinnamon extract equivalent to 3 g of cinnamon powder or a placebo capsule three times a day for 4 months in a double-blind study.
The study of Ziegenfuss et al. 29 was conducted with 22 mixed gender subjects with prediabetes and the metabolic syndrome who were randomly assigned to consume 500 mg of cinnamon extract/day or a placebo for 12 weeks.
The subjects in the study of Blevins et al. 22 were selected from individuals with type 2 diabetes based on American Diabetes Association criteria (n=9), stratified by sex and randomized to consume one capsule containing either 500 mg of total cinnamon (C. cassia) or placebo (wheat flour) at both breakfast and dinner for 3 months. Compliance was assessed by capsule count, and dietary patterns were monitored using a monthly 3-day food journal.
Vanschoonbeek et al. 28 recruited a total of 25 postmenopausal patients with type 2 diabetes who were asked to consume either cinnamon (C. cassia, 1.5 g/day) or a placebo for a 6-week period of intervention. Subjects maintained their normal medication as well as dietary and physical activity patterns. Dietary food intake records and details on energy intake and macronutrient composition of the diet were examined.
Stoecker et al. 26 studied the effects of a water extract of cinnamon in a double-blind randomized placebo-controlled trial (n=137) using fasting plasma glucose–impaired participants recruited from Beijing and Dalian, China. Subjects received either a 250-mg placebo (baked wheat flour) capsule twice per day or a 250-mg dried water-soluble cinnamon extract preparation (CinSulin®, standardized type-A polymer water extract [bark] from Tang-An Medical, Beijing, China) capsule twice per day for 2 months. This study was reported in abstract form but met the search criteria.
Tang et al. 27 studied 11 healthy subjects, 21–38 years old, in an 8-week, randomly assigned, crossover study that involved the ingestion of either 3.0 g of cinnamon or 2.8 g of turmeric for 4-week periods, and FBG and lipid concentrations were also assessed at the start of the study and at the crossover and end time points.
The meta-analysis (Fig. 1) of the eight trials showed that the intake of supplements of cinnamon or as cinnamon extract only results in a statistically significant lowering of FBG: –0.49±0.2 mmol/L (8.77±3.52 mg/dL) for all studies (Fig. 1, bar 9; n=8, P=.025) and −0.48±0.17 mmol/L (8.7±3.10 mg/dL) for cinnamon extract only (Fig. 1, bar 10; n=5, P=.008).
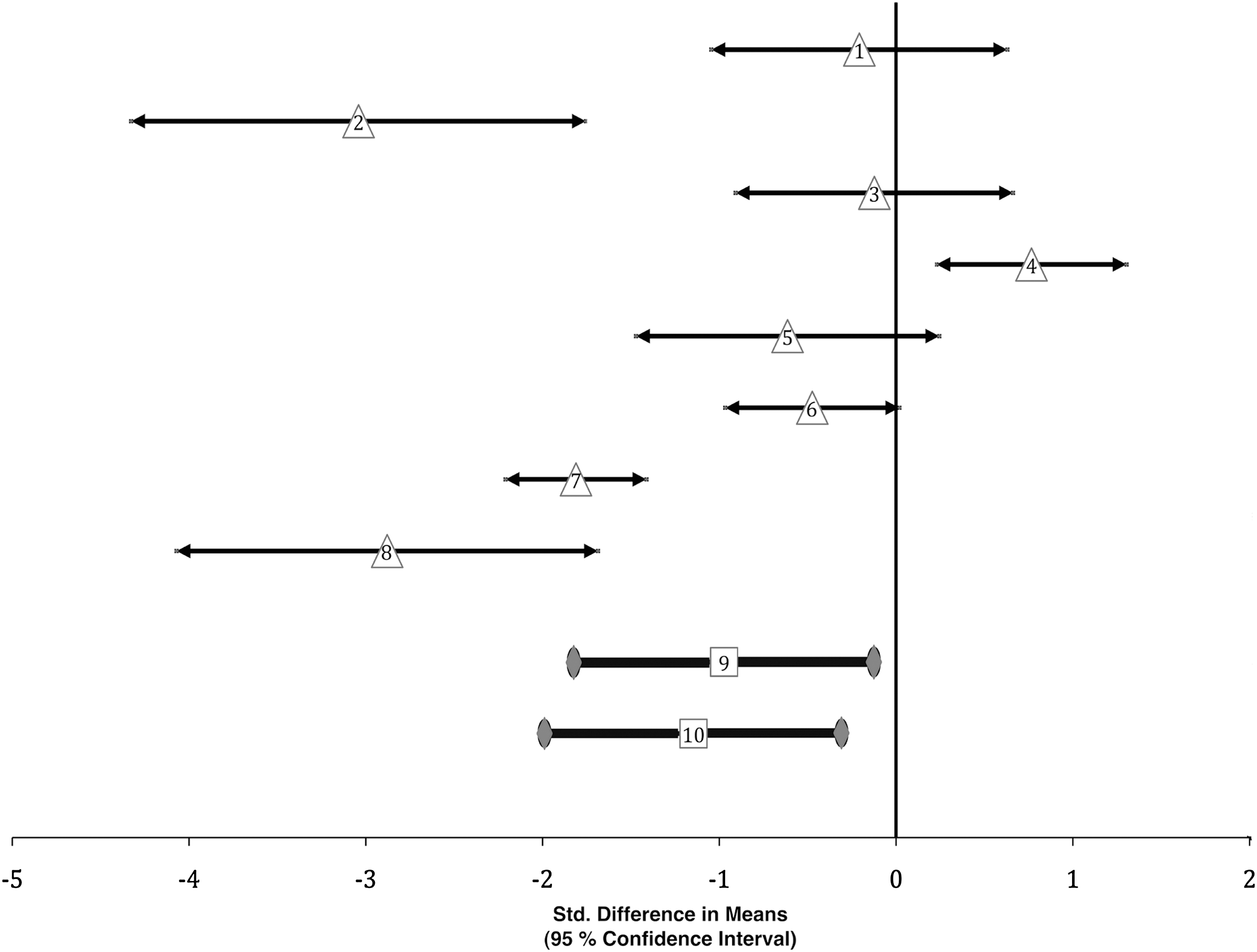
Meta-analysis data and results. Individual study standardized difference in FBG means along their 95% confidence intervals are plotted using triangles. The numbers inside the triangles refer to the individual studies: (1) Tang et al. 27 (2) Khan et al., 23 (3) Vanschoonbeek et al., 28 (4) Blevins et al., 22 (5) Ziegenfuss et al., 29 (6) Mang et al., 24 (7) Stoecker et al., 26 and (8) Roussel et al., 25 The two plots denoted with thicker lines and open square symbols are the results of the meta-analysis: (9) the overall cinnamon standardized difference in FBG means along with the 95% confidence interval (n=8; P=.025) and (10) cinnamon extract only standardized difference in FBG means along with the 95% confidence interval (n=5; P=.008).
The funnel plot analysis graph (Fig. 2) approximated an inverted symmetrical funnel, which suggests limited publication bias. However, the use of a funnel plot to assess publication bias is of limited utility as funnel plot asymmetry may arise not only from publication bias, but may also be the result of clinical heterogeneity between studies or study methodological heterogeneity.

A funnel plot was used to assess possible publication bias. Funnel plot analysis is done by examining the shape of the graph obtained by plotting treatment effect versus study size. The standardized mean difference for each study used in the meta-analysis was plotted against sample size for that study.
Discussion
Although, as noted, there have been several recent reports assessing cinnamon's effect on FBG, several factors have led us to revisit the issue of cinnamon effects on blood glucose. One is that Stoecker et al. 26 have very recently presented results of a larger (n=137) cinnamon extract trial that found that after 2 months, FBG decreased (P<.001) in the cinnamon-supplemented group (from 8.85±0.36 to 8.19±0.29 mmol/L) compared with from 8.57±0.32 to 8.44±0.34 mmol/L in the placebo group (P=.45). In addition, Roussel et al. 25 have recently reported the results of a 4-month, double-blind, placebo-controlled trial using an aqueous extract of cinnamon in 22 subjects with impaired FBG. They reported a decline in fasting glucose as well as a decline in malondialdehyde accompanied by increases in plasma antioxidant markers. The meta-analysis of Baker et al. 13 did not detail “advanced statistical methods were used to impute change scores as suggested by Follman and colleagues.” The review by Kirkham et al. 14 used data from all articles the authors deemed relevant, including reviews and meta-analyses, but did not clearly describe the metrics used to weigh the evidence that led them to their conclusions. Given this, it is problematic to assess the effect on their conclusions of what appears to be a number sign error in their data with respect to the effect of cinnamon on glucose as reported by Blevins et al. 22 The latter reported that in their study intake of 1 g of cinnamon for 3 months on average raised blood glucose (their Table 1;+9.8±5.9 mg/dL), whereas Kirkham et al. 14 reported this as a decline (their Table 5; −0.54 mmol/L).
The type of cinnamon used as well as its preparation in these studies is of significance. 30 Cinnamon provided whole or as an aqueous extract likely contains a differing number of active agents with varying antihyperglycemic actions, 31,32 as the hypoglycemic activity has been reported to appear in both aqueous extract and powdered bark. 31,33 It is difficult to obtain accurate assessments of efficacy from preparations with low levels of active components. This is reflected in the animal studies reporting significant effects for cinnamon, where higher cinnamon dosages per body weight compared with human studies were used. 33 In addition, results in humans along with differences in effects with elevated glucose load in animals have suggested a relationship between baseline FBG and FBG reduction with cinnamon. 14 However, the exact relationship between blood glucose levels and cinnamon's effect in humans remains to be established. Given the already limited number of studies available, further subdividing them reduces the power of the meta-analysis. However, it should be noted that performing the meta-analysis by using only those studies using water extracts of cinnamon retains a significant overall effect on blood glucose levels (Fig. 1, bar 10; −8.7±3.1 mg/dL; P<.008). The fact that water extracts of cinnamon have activity suggests that these may be preferable in terms of use compared with whole cinnamon. This difference arises as using water extracts of cinnamon achieves the desired blood glucose effects while avoiding the nonpolar constituents in whole cinnamon or the cinnamon flavor components that have been linked to deleterious effects (e.g., oral lesions 34 and mutagenicity 35 ).
In summary, the results of meta-analysis show that the intake of cinnamon/cinnamon extract by type 2 diabetics or prediabetics does lower their blood glucose significantly, albeit modestly. The percentage declines in FBG upon cinnamon intake are of the same order of magnitude as for metformin (i.e., −5.8% [95% confidence interval −10.4%, −1.2%] for all cinnamon versus −4.5% [95% confidence interval −6.0%, −3.0%] for metformin). 36 Metformin not only reduces weight and insulin resistance in persons with diabetes but has been shown to reduce the incidence of new-onset diabetes in people at risk by 40%. 36 This result of the current meta-analysis of eight clinical studies (i.e., the significant beneficial effect of cinnamon/cinnamon extract on FBG) is in contrast to the two previous meta-analyses using lower numbers of trials. The reasons behind the difference in outcome are likely due to inclusion of the more recent reports of studies on cinnamon's effect on FBG, which have used water extracts of cinnamon and/or larger study populations. The plausibility of the finding of activity of cinnamon on FBG is bolstered by not only the reports showing cinnamon's ability to affect glucose homeostasis in experimental animals, the majority of the over 30 studies reporting declines in glucose, and increased insulin sensitivity with whole cinnamon or components, 30 but the recent report detailing its ability to alter the postprandial curves for glucose and other glucose-related signals in humans as well. Specifically, Hlebowicz et al. 10 reported increased postprandial glucagon-like peptide-1 concentrations and decreased insulin concentrations upon cinnamon intake, which suggests that cinnamon stimulates the insulin receptor. Given that the meta-analysis results indicate that intake of cinnamon/water extracts of cinnamon reduces blood glucose, cinnamon intake in patients with impaired glucose tolerance or type 2 diabetes mellitus should improve glycemic control and decrease insulin demand, with secondary effects on β-cell mass and prevention of the loss of β-cell function. It is interesting that the use of cinnamon or cinnamon extract has been suggested as a means to deal with insulin resistance and glucose intolerance that accompanies sleep loss. 37 This suggestion has taken on increased importance following the very recent report describing the machinery involving the circadian clock, through which two transcriptional activators, Clock and Bmal1, and cryptochrome (Cry1 and Cry2) and Period (Per1, Per2 and Per3) repressors that feed back on Clock–Bmal1 activity coordinate glucose metabolism with changes in the external environment. 38 Clearly, a long-term clinical trial involving a larger number of patients is needed to evaluate the effects of cinnamon supplementation, in particular, water extracts of cinnamon, on morbidity and mortality in type 2 diabetes as well as progression to type 2 diabetes.
Footnotes
Author Disclosure Statement
P.A.D. has served as a consultant to Tang-An Medical. No other potential conflicts of interest relevant to this article are reportable. W.Y. declares no conflicts of interest. Mention of trade names or commercial products in this article is solely for the purpose of providing specific information and does not imply recommendation or endorsement by the U.S. Department of Agriculture.