
Abstract
This study was designed to investigate the anti-obesity and anti-atherosclerotic effects of supplementation with Chungkookjang (CKJ), a traditional fermented soybean food, in overweight/obese subjects. The study was a 12-week, randomized, double-blind, placebo-controlled clinical trial followed by a 3-week screening period. Overweight/obese subjects (both groups having a body mass index ≥23 kg/m2 and waist hip ratio of ≥0.90 for men and ≥0.85 for women) who were not diagnosed with any disease were included in this study. Sixty subjects were randomly divided into a CKJ (n=30, 26 g/day) or placebo (n=30) group. During the 12-week intervention period, subjects were asked to maintain their usual diet and activity and not to take any functional foods or dietary supplements. Anthropometric parameters, abdominal fat distribution by computerized tomography, and blood parameters (lipid profile, atherosclerotic indices) before and after the 12-week intervention period were measured. Fifty-five subjects (29 CKJ group, 26 placebo group) finished the study. After the 12 weeks of supplementation, subjects in the CKJ group showed a significant improvement in apolipoprotein B (P<.05) compared with the placebo group. Visceral fat areas by computerized tomography scans and apolipoprotein B/apolipoprotein A1 showed a tendency to decrease in the CKJ group, but there were no significant differences between the CKJ and placebo groups. These results suggested that CKJ supplementation has potential anti-atherosclerotic effects that might be more pronounced when combined with lifestyle modification.
Introduction
O
Soybean is a rich source of protein that has been consumed for the past 5,000 years in Oriental countries. The awareness that soy products are healthy has increased its consumption in Western countries. 3 Soybean contains functional components such as isoflavones, phytic acid, trypsin inhibitor, saponins, phytosterol and phenolic compounds, dietary fiber, and oligosaccharides. 4,5 Soybean isoflavones, including genistein and daidzein, exist in the glucosidic form and are readily digested into an aglycone form in the intestinal tract. 6
Chungkookjang (CKJ) is one of the traditional Korean fermented-soybean foods, made with bacterial inocula from rice straw and boiled soybean. It has a characteristic fragrance, taste, and nutritional components of fermented soybean. 7 Metabolites produced during CKJ fermentation in addition to the preexisting compounds in soybean could be responsible for eliciting its health-promoting effects.
CKJ has distinct characteristics compared with other fermented-soybean products. It is fermented predominantly with Bacillus subtilis for short periods (2 days) without salts or other seasoning. 8 During fermentation, isoflavonoids are converted from glycosides into their corresponding aglycones, and most proteins are degraded into small peptides and amino acids. 9,10
CKJ has antioxidative and antimicrobial properties along with other beneficial activities. 11,12 The isoflavones (genistein, daidzein, and their β-glucosides) are present in high concentrations in soybean and are correlated with phytoestrogen, antioxidative, antitumor, and antihypertensive functions. 4,13 –15 Thus, CKJ has attracted attention for its potential physiological functionalities.
Anti-obesity and anti-atherosclerotic effects of CKJ have been reported from in vivo and in vitro studies 16 –24 but have not been confirmed by clinical trials. Hence this study was designed to investigate the efficacy of supplementation with CKJ, a traditional fermented soybean food, as an anti-obesity and anti-atherosclerotic intervention in overweight/obese subjects.
Subjects and Methods
Study subjects
The study subjects were recruited from the Clinical Trial Center for Functional Foods in Chonbuk National University Hospital, Jeonju, Republic of Korea, during June 2007. A total of 89 healthy male and female subjects (19–65 years old) agreed to participate. Only those subjects who were overweight/obese (both groups having a body mass index of ≥23 kg/m2 and a waist hip ratio of ≥0.90 for men and ≥0.85 for women) and not diagnosed with any disease were included in this study. Sixty subjects met the study criteria (38.68±1.47 years old, weighing 72.2±1.47 kg) and were randomly divided into a CKJ (n=30, 26 g/day) or placebo (n=30, 26 g/day) group. Exclusion criteria for the study were as follows: (1) lipid metabolism disorder; (2) significant variation in weight (10%) in the past 3 months; (3) cardiovascular disease (e.g., arrhythmia, heart failure, myocardial infarction, a patient with a pacemaker); (4) allergic or hypersensitive to any of the ingredients in the test products; (5) history of disease that could interfere with the test products or impede their absorption, such as gastrointestinal diseases (Crohn's disease) or gastrointestinal surgery (including a cecum or enterocele surgery); (6) participation in other clinical trials within 2 months; (7) abnormal hepatic liver function or renal disease (e.g., acute/chronic renal failure, nephrotic syndrome); (8) use of antipsychosis drug therapy within 2 months; (9) a laboratory test or medical or psychological condition deemed by the investigators to interfere with successful participation in the study; (10) history of alcohol or substance abuse; or (11) pregnancy or breast feeding. All subjects gave written informed consent before beginning the study. The protocol was approved by the Functional Foods Institutional Review Board of Chonbuk National University Hospital.
Study design
This study was a 12-week, randomized, double-blind, placebo-controlled clinical trial followed by a 3-week screening period.
Subjects who responded and met entry criteria during a telephone screening interview were scheduled for a baseline visit. The evaluation included a physical examination, electrocardiogram, and screening blood parameter studies. Also, subjects were scheduled for a screening visit (within 3 weeks) where the informed consent was reviewed and signed. A random number between 1 and 60 was generated by the computer for each subject. The enrolled subjects were scheduled for the first visit, and subjects were randomly assigned to one of two groups, either the CKJ (n=30) or placebo (n=30) group.
The CKJ group took 26 g (2.7-g pills per pack, three times a day) of freeze-dried CKJ daily for 12 weeks, which was equivalent to 70 g 25 –27 of fresh CKJ; the placebo group took the same amount of an isocaloric placebo.
CKJ produced by the traditional method was purchased, freeze-dried using a freeze-dryer (model PVTFD 100R, Ilsinlab, Yangju, Republic of Korea), and then made into pills (Imshil Herbal Medicine Co., Imshil, Republic of Korea). Placebos were made with the same taste, appearance, and energy content but without the principal ingredient that was present in the CKJ. CKJ/placebo pills were provided to subjects every 4 weeks. During the intervention period of 12 weeks, subjects were asked to continue their usual diets and activity and were asked not to take any other functional foods or dietary supplements. Anthropometric and biochemical parameters, computerized tomography, vital signs, and nutrient intakes were measured before and after the intervention period for both groups. Every fourth week the subjects were asked to report for assessment of any adverse events or any changes in training, lifestyle, or eating patterns and to assess pill compliance.
Assessments
Subjects were asked to visit the clinic once every 4 weeks for a total of five clinical visits, including screenings (screening and 0, 4, 8, and 12 weeks). At each visit, current medication use was reviewed, and symptoms or side effect information was recorded. A screening visit of subjects for demographic information (sex, age), information on alcohol consumption and smoking, medical history, and urine pregnancy test was conducted.
Assessments included the following: anthropometric parameters (weight, body mass index, body fat mass, percentage body fat, lean body mass, and waist to hip ratio) were measured using Inbody version 3.0 (Biospace Co., Seoul, Republic of Korea) on each visit. Blood samples were collected after a minimum of 12 hours of fasting before and after the 12-week intervention period for measuring the blood lipid profile (total cholesterol [TC], triglycerides, high-density lipoprotein-cholesterol [HDL-C], low-density lipoprotein-cholesterol [LDL-C], free fatty acid), apolipoprotein (apolipoprotein A1 [Apo A1], apolipoprotein B [Apo B]), and atherosclerotic indices (TC/HDL-C, LDL-C/HDL-C, [TC – HDL-C]/HDL-C, [(TC – HDL-C)×Apo B]/[HDL-C×Apo A1], Apo B/Apo A1). Blood samples were analyzed on a Hitachi model 7600-110 analyzer (Hitachi High-Technologies Corp., Tokyo, Japan) by standard methods at the biochemical laboratory of Chonbuk National University Hospital. Abdominal fat distribution was performed before and after the 12-week intervention period. Visceral fat, subcutaneous fat, total fat, and visceral subcutaneous ratio were measured using computerized tomography.
Safety and dietary assessment
Safety assessments included the following: electrocardiogram, hematology tests, and laboratory tests (white blood cells, red blood cells, hemoglobin, hematocrit, platelet count, total protein, albumin, alanine aminotransferase, aspartate aminotransferase, blood urea nitrogen, and creatinine) before and after the 12-week intervention period and pulse and blood pressure at every visit (after a 5-minute rest, using the OMRON T4 digital blood pressure monitor [OMRON Corp., Tokyo]) and self-reported (at every visit). All subjects were invited to complete a 3-day dietary record, including 2 weekdays and 1 weekend day, to evaluate energy intake and diet quality at every clinical visit. Dietary intake data were analyzed by the same dietitian, using the CAN-pro version 3.0 software (The Korean Nutrition Society, Seoul).
Statistical analysis
Statistical analysis was performed using SAS version 9.0 for Windows (SAS Institute, Cary, NC, USA). Data are presented as mean±SE values. In the statistical analysis of triglycerides, one subject (101-R-55) was excluded because of experimental error.
The χ2 test was performed to determine differences at baseline in frequencies of categorized variables between the groups. A linear mixed-effects model was applied to repeated-measures data for each continuous outcome variable. Fixed effects included treatment group, treatment visit, and interaction between treatment group and visit. When the analysis of variance indicated significant differences among groups, post hoc tests (Tukey's tests) were used to separate the differences between groups before and after the 12-week intervention period. A value of P<.05 was considered statistically significant.
Results
Study subjects
Among the 89 subjects screened, 29 subjects had laboratory tests and/or physical examination results in the exclusion criteria category and hence were excluded from the study. The remaining 60 subjects fulfilled the study criteria and were distributed equally into two groups: CKJ and placebo.
One subject from the CKJ group and four subjects from the placebo group withdrew from the study because of personal reasons. At the end of the study, 55 subjects (29 CKJ group, 26 placebo group) were able to finish the study (Fig. 1).
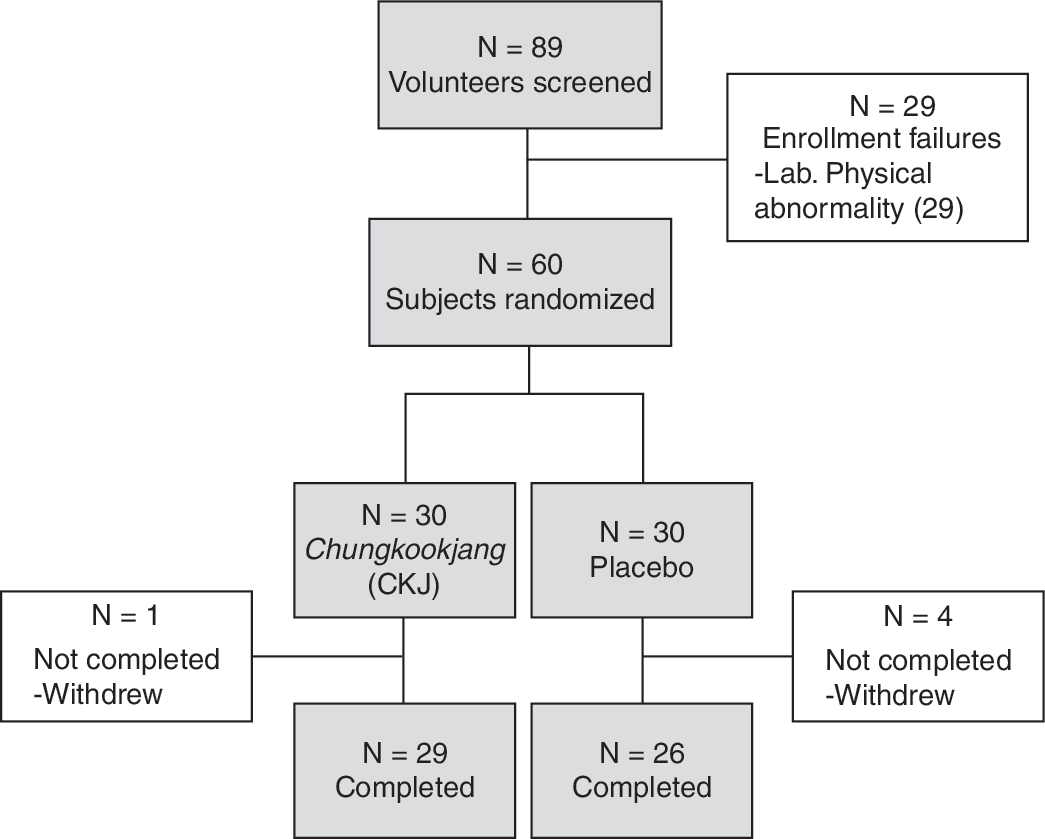
Flow chart for the study subjects.
Subject characteristics, anthropometric parameters, and dietary assessment
General characteristics of the subjects are shown in Table 1. There were no significant differences in baseline characteristics such as sex, age, height, and weight between the CKJ and placebo groups.
Data are mean±SE values.
By independent t test.
By χ2 test.
CKJ, Chungkookjang; M/F, male/female ratio.
Anthropometric parameters were not significantly affected by the treatment (data not shown). There were no significant differences in the dietary intake (calorie, carbohydrate, protein, fat) between the groups during the intervention study period (data not shown).
Abdominal fat area
Changes in abdominal fat during the 12-week intervention period are shown in Table 2. After 12 weeks of intervention, the visceral fat area showed a tendency to decrease in the CKJ group (from 8,073±734 mm2 to 7,167±554 mm2), but no significant differences were seen between the CKJ and placebo groups.
Data are mean±SE values.
Linear mixed-effect model.
Lipid profile and atherosclerotic indices
Changes in lipid profiles before and after the 12-week intervention period are shown in Table 3. After the intervention of 12 weeks, no significant changes were observed in blood TC, triglyceride, HDL-C, LDL-C, free fatty acid, or Apo A1 level in either the CKJ or placebo group. The blood TC and LDL-C level showed a tendency to decrease in the CKJ group, whereas the placebo group showed an increasing trend. In the CKJ group, the Apo B level in blood was significantly decreased (from 77.24±3.33 mg/dL to 67.24±3.21 mg/dL, P<.001), whereas the placebo group did not show a significant difference. The CKJ group showed a significant improvement in Apo B level compared with the placebo group (P<.05).
Data are mean±SE values.
By linear mixed-effect model.
By post hoc test (Tukey's tests).
P<.05 for comparison of 12-week CKJ and placebo group values; ***P<.001 for comparison with 0-week CKJ value.
Apo A1, apolipoprotein A1; Apo B, apolipoprotein B; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol.
Changes in atherosclerotic indices during the 12-week intervention period are shown in Table 3. After the 12-week intervention, no significant changes were observed in TC/HDL-C, LDL-C/HDL-C, (TC – HDL-C)/HDL-C, ([TC – HDL-C]×Apo B)/(HDL-C×Apo A1), and Apo B/Apo A1 in both the CKJ and placebo groups. The Apo B/Apo A1 ratio showed a tendency to decrease in the CKJ group (from 0.55±0.03 to 0.50±0.03, P<.01), but there were no significant differences between the CKJ and placebo groups.
Safety
At each visit, symptom or side effect information was recorded, but no moderate or severe side effects or serious adverse events were reported during the 12-week study period. The evaluation included a laboratory test, electrocardiogram, and vital signs (blood pressure, pulse) during the subjects' visits. The results of the clinical tests were in the normal range, so no subjects withdrew because of adverse effects.
Discussion
We investigated the effects of CKJ supplementation on anthropometric parameters and abdominal fat distribution by computerized tomography and blood components (lipid profile, atherosclerotic indices) in overweight/obese subjects (body mass index ≥23 kg/m2).
Abdominal fat distribution as measured by computerized tomography did was not different between the CKJ and placebo groups. However, the visceral fat area showed a tendency to decrease in the CKJ group, but no significant differences were seen between the CKJ and placebo groups.
In a study in which
After an intervention of 12 weeks, no significant changes were observed in the levels of TC or LDL-C in blood of subjects in either the CKJ or placebo group; however, the CKJ group showed a tendency to decrease, whereas the placebo group increased. Studies by Beynen et al. 17 and Tasker and Potter 24 obtained repeated success in improving hypercholesterolemia by using soybean protein in animal experiments, but its effect in human clinical trials remains inconclusive. Krauss et al. 20 reported that soybean proteins are effective even when the blood cholesterol level is higher than 258.50 mg/dL. All the subjects in this study had blood cholesterol levels lower than 250 mg/dL, which may be responsible for the lack of benefit on TC and LDL-C levels. Further studies are needed in this regard.
Apo B is the primary apolipoprotein of LDL-C, which effectively predicts the risk of coronary artery diseases, and is considered to be more useful than TC, HDL-C, and LDL-C. By having a close relationship with all potential threats from atherosclerosis and cardiovascular diseases, Apo B is known to be a better diagnostic tool than LDL-C, and the lower the value, the lower will be the risk of developing atherosclerosis. 31 Apo B in this study was significantly decreased in the CKJ group compared with the placebo group (P<.05). In a test performed on obese women, Gwak et al. 19 also showed a significant decrease in the level of Apo B. After several studies, isoflavone in soybean products were reported to be beneficial in lowering the risk of atherosclerosis. 21 An epidemiological study found that Asians have lower mortality from coronary artery diseases than do Westerners; this may be due to the fact that Asians consume a vast quantity of soybean products in their diets. 18 Saponin, phytic acid, fiber, genistein, and indigestible protein are the soybean components that act as anti-atherosclerotic agents. With these components enabling bile acid production and controlling cholesterol metabolism and endocrine functions, they reduce the blood lipid levels, eventually resulting in the anti-atherosclerotic effect. 16,22,23 The CKJ used in this study contains isoflavones that may be responsible for the results. Therefore, regular intake of CKJ will lower the blood lipid profiles in subjects with increased levels of Apo B, thus being an effective improvement strategy in managing cardiovascular diseases and especially coronary artery diseases.
Apo B/Apo A1 ≥0.55 is a borderline indicator that separates the normal group from patients with coronary artery diseases. In this study, Apo B/Apo A1 showed a tendency to decrease in the CKJ group, but no significant differences were seen between the CKJ and placebo groups. Therefore, regular intake of CKJ may help in lowering the Apo B/Apo A1 ratio, thus decreasing the risks of coronary artery diseases and cardiovascular-related diseases.
A possible weakness of this study is that the diets and activity levels were not controlled, and future studies should include a diet and exercise component. Moreover, because this study is a comparison study including a placebo group, the psychological effects of placebo and the effects of placebo components cannot be excluded.
Because no other studies have evaluated the effects of CKJ in overweight/obese subjects, it is difficult to draw firm conclusions on the efficacy of CKJ supplementation for decreasing the risk of atherosclerosis in overweight/obese people. However, the results of this study showed that 70 g (dried weight, 26 g) of CKJ supplement for 12 weeks significantly improved Apo B compared with the placebo group. Also, within the CKJ group, visceral fat and the Apo B/Apo A1 ratio showed a tendency to decrease, suggesting CKJ is a viable complementary functional food for preventing atherosclerosis without harmful effects.
Further research is needed using a study design that evaluates dietary intake data and provides the CKJ incorporated into food as it is commonly consumed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.