
Abstract
Studies have suggested that 1-α-OH-vitamin D3 and green tea polyphenols (GTPs) are promising dietary supplements for mitigating chronic inflammation-induced fibrosis of vessels because of their anti-inflammatory properties. This study evaluated (1) the impact of 1-α-OH-vitamin D3 on myocardial fibrosis in female rats with chronic inflammation and (2) if 1-α-OH-vitamin D3 and GTPs have an additive or synergistic effect to attenuate myocardial fibrosis in these female rats. A 3-month study of a 2 (no 1-α-OH-vitamin D3 vs. 0.05 μg/kg 1-α-OH-vitamin D3, five times per week)×2 (no GTPs vs. 0.5% GTPs in drinking water) factorial design in lipopolysaccharide (LPS)-administered female rats was performed. Additionally, a group receiving placebo administration was used to compare with a group receiving LPS administration only to evaluate the effect of LPS. Masson's Trichrome staining evaluated myocardial fibrosis in coronary vessels and surrounding myocardium. Spleen cyclooxygenase-2 mRNA expression was determined by real-time polymerase chain reaction. Total lipid profiles were also determined. Whole blood was used for differential cell counts. Data were analyzed by two-way analysis of variance followed by mean separation procedures. At 3 months LPS administration induced myocardial fibrosis in vessels and surrounding myocardium, spleen cyclooxygenase-2 mRNA expression, and elevated leukocyte counts, whereas both 1-α-OH-vitamin D3 administration and GTPs supplementation significantly attenuated these pro-inflammatory events. The inhibitory effects of 1-α-OH-vitamin D3 and GTPs seem to be an individual effect, instead of an additive or synergistic effect. 1-α-OH-vitamin D3 and GTPs lowered red blood cell counts, hematocrit, and hemoglobin. Neither 1-α-OH-vitamin D3 nor GTPs affected lipid profiles. In summary, both 1-α-OH-vitamin D3 administration and GTPs supplementation mitigate myocardial fibrosis through suppression of a chronic inflammation innate immune response.
Introduction
E
Unlike the plain, unmodified vitamin D, alphacalcidol (1-α-OH-vitamin D3), a hydroxylated form of vitamin D, was shown to increase the bioavailability of active D-hormone in different target tissues of patients. 6,7 1-α-OH-vitamin D3 administration is known to be associated with reduced risk for cardiovascular death in patients with end-stage renal disease, a population known to have higher cardiovascular event rates and a greater severity of coronary obstructive disease. 8 –10 Giulietti et al. 11 demonstrated that 1-α-OH-vitamin D3 down-regulated the expression of inflammatory cytokines in monocytes collected from patients with type 2 diabetes. These findings suggest that 1-α-OH-vitamin D3 may protect against CVD such as myocardial fibrosis. However, the effect of 1-α-OH-vitamin D3 on chronic inflammation-induced myocardial fibrosis, with possible mechanisms, has never been studied. On the other hand, green tea, one of the most popular beverages in the world, has received considerable attention due to its many scientifically proven beneficial effects on human health, including improvement of CVD. 12 –16 Stangl et al. 13 proposed that such beneficial cardiovascular effects of tea may be due to its vasculoprotective, antithrombogenic, anti-inflammatory, and antioxidative stress capacities. Our recent study showed that drinking water supplemented with green tea polyphenols (GTPs) mitigated myocardial fibrosis because of a reduction of innate immune responses and inflammation. 17 However, the potential impact of 1-α-OH-vitamin D3 plus green tea bioactive ingredients on this chronic inflammation-induced myocardial fibrosis and related molecular mechanisms is also not well understood.
The present study was designed to evaluate (1) the potential benefit of 1-α-OH-vitamin D3 in the treatment or prevention of myocardial fibrosis in female rats with chronic low-grade inflammation and (2) if 1-α-OH-vitamin D3 and GTPs have an additive or synergistic effect to attenuate myocardial fibrosis in these female rats. We hypothesized that (1) 1-α-OH-vitamin D3 administration will avert chronic inflammation-induced myocardial fibrosis in female rats, (2) 1-α-OH-vitamin D3 plus GTPs will additively or synergistically avert such myocardial fibrosis in female rats, and (3) this inhibitory impact will be due to an inhibition of pro-inflammatory mediators, such as COX-2, and the innate immune response. Evaluating the beneficial impact of 1-α-OH-vitamin D3 and GTPs on myocardial fibrosis in rats with chronic systemic inflammation will advance our understanding of their effects on atherosclerosis biology in order to potentially mitigate myocardial fibrosis in humans with chronic systemic inflammation.
Materials and Methods
Experimental design
The virgin 3-month-old CD female rat receiving lipopolysaccharide (LPS) administration is a well-established model of chronic inflammation-induced myocardial fibrosis. 18,19 Among the LPS-treated rats, a 2 (0 vs. 0.05 μg/kg body weight 1-α-OH-vitamin D3)×2 (no GTPs vs. 0.5% GTPs in drinking water) factorial design was used to evaluate the effects of 1-α-OH-vitamin D3, GTPs, and 1-α-OH-vitamin D3×GTPs interaction on chronic inflammation-induced myocardial fibrosis along with its related mechanism(s). In addition, a group receiving placebo administration only (P group) was used to compare with a group receiving LPS administration only (L group) to evaluate the effect of LPS.
Animals and treatments
Virgin 3-month-old CD female rats (n=50) (Charles River, Wilmington, MA, USA) were allowed to acclimate for 5 days to a rodent chow diet and distilled water ad libitum. After acclimation, the rats were subjected to the procedures of placebo or LPS administration as described previously. 20 In brief, LPS (E. coli serotype O127:B8, Sigma, St. Louis, MO, USA) was incorporated into time-release pellets (Innovative Research of America, Sarasota, FL, USA) and designed to deliver a consistent dose (33 μg/day) for 3 months. For the LPS-administered animals (n=40), the dorsal neck area was shaved, and sterile techniques were used. A small incision was made at the back of the neck, a horizontal pocket was created for LPS pellet administration using forceps, and the incision site was closed with surgical glue. The placebo-administered group (P group, n=10) received a pellet containing matrix only using the same procedures of administration described above. All rats were maintained on a regular rodent chow diet ad libitum throughout the study period.
After surgery, LPS-administered rats were randomized by weight and assigned to one of four groups (n=10 per group) throughout the 3-month study period: (1) LPS administration (L group), (2) LPS + 1-α-OH-vitamin D3 (LD group), (3) LPS + GTPs (LG group), and (4) LPS + GTPs + 1-α-OH-vitamin D3 (LGD group). The rats in the L group were given drinking water only. The rats in the LD group were orally administrated 1-α-OH-vitamin D3 at 0.05 μg/kg of body weight five times per week. The selection of 1-α-OH-vitamin D3 dose was based on a previous study showing that 1-α-OH-vitamin D3 (0.5 μg/kg, five times a week) increased the number of osteoblasts, suppressed trabecular bone resorption, and markedly increased periosteal and endocortical bone formation. 21 The rats in the LG group were given a concentration of 0.5% GTPs in drinking water daily to mimic human consumption of green tea of 4–6 cups a day. 22,23 The rats in the LGD group were given both GTPs and 1-α-OH-vitamin D3, whereas the rats in the P group were given drinking water only.
Distilled water mixed with GTPs was prepared fresh daily. The amount of water consumed was recorded for each rat. GTPs (≥98.5%) were purchased from the same source as that used previously in our studies (Waters, Milford, MA, USA). According to the high-performance liquid chromatography with electrochemical detection and high-performance liquid chromatography with ultraviolet analyses, every 1000 mg of GTPs contained 464 mg of (–)-epigallocatechin gallate, 112 mg of (–)-epicatechin gallate, 100 mg of (–)-epicatechin, 78 mg of (–)-epigallocatechin, 96 mg of (–)-gallocatechin gallate, and 44 mg of catechin. Rats were housed individually under a controlled temperature of 21±2°C with a 12-hour light–dark cycle. Rats were examined daily and weighed weekly. All procedures were approved by the Texas Tech University Health Sciences Center Institutional Animal Care and Use Committee (Lubbock, TX, USA).
Sample collection and preparation
At 1, 2, and 3 months of study, the rats were anesthetized with isoflurane, and tail blood samples were collected for the determination of differential hemopathologic counts by manual microscopy from a peripheral blood smear. At the end of the study, all animals were anesthetized and euthanized, blood samples were drawn from the heart, and serum samples were isolated and stored at −80°C for later analysis. The heart specimens were harvested and kept in 10% formalin for later histological evaluation.
Histopathologic evaluation of heart
After necropsy, the formalin-fixed heart tissue was sectioned transversely (6-μm sections). Masson's Trichrome staining was applied to the heart sections for evaluation of myocardial fibrosis in coronary vessels and surrounding myocardium. All slides were evaluated by two study pathologists for staining intensity, in a blinded manner according to the following scoring system: 0=normal with no visible staining, 1=low with mild staining, 2=medium with moderate staining, and 3=high with marked staining. 18
Spleen COX-2 mRNA expression determination
Administration of LPS to rodents produced a generalized inflammatory response with increased release of TNF-α into the circulation and that of mRNA expression in spleen. 24 Total spleen RNA was extracted using TRIzol® reagent (Invitrogen Life Sciences, Carlsbad, CA, USA). One microgram of total RNA was reverse-transcribed into cDNA using a high-capacity cDNA reverse transcription kit (Applied Biosystems Inc., Foster City, CA, USA). An aliquot of each diluted cDNA sample was used for polymerase chain reaction amplification using TaqMan® gene expression assays on the ABI GeneAmp® PCR system 7000 in the presence of 1×SYBR® Green master mix (Applied Biosystems) with respective primer pairs for COX-2 (forward primer, 5′-CGG ACT TGC TCA CTT TGT TG-3′; reverse primer, 5′-GGT ATT TCA TCT CTC TGC TCT GG-3′) and for glyceraldehyde 3-phosphate dehydrogenase (forward primer, 5′-TAT CAC TCT ACC CAC GGC AAG-3′; reverse primer, 5′-ATA CTC AGC ACC AGC ATC ACC-3′). The thermal profile of the reaction consisted of 50°C for 2 minutes, 95°C for 10 minutes, and then 40 cycles of (95°C for 15 seconds and at 60°C for 1 minute). The expression level of TNF-α was normalized to that of glyceraldehyde 3-phosphate dehydrogenase.
Total lipid profiles
Serum lipid profiles, including triglycerides, total cholesterol, low-density lipoprotein, and high-density lipoprotein, were determined using an autochemistry analyzer (Vitros® 5.1 F5 Chemistry System, Ortho Clinical Diagnostics, Raritan, NJ, USA).
Hemopathologic blood counts
Whole blood specimens were stained with Wright–Giemsa stain. White blood cell (WBC) counts with differentials, including lymphocytes, neutrophils, and eosinophils, were measured by manual microscopy. In addition, red blood cell (RBC) counts, hematocrit (Hct) counts, and hemoglobin (Hb) were also determined.
Statistical analysis
Results were expressed as mean±SEM values. All data were analyzed using SigmaStat version 2.03 (Systat Software, Inc., San Jose, CA, USA). Normality of distribution and homogeneity of variance were tested. The difference between the P group and the L group was analyzed by t test for each parameter to evaluate the effect of LPS administration. Data from the hemopathologic blood counts (RBC, Hct, Hb, WBC, lymphocytes, neutrophils, and eosinophils) were analyzed by three-way analysis of variance (1-α-OH-vitamin D3 administration×GTPs levels×time) followed by Fisher's Protected Least Significant Difference post hoc test to evaluate the effect of 1-α-OH-vitamin D3 administration, GTPs supplementation, time, or interaction. Data from the histological scoring of myocardial fibrosis, COX-2 mRNA expression, and total lipid profiles (triglycerides, cholesterol, low-density lipoprotein, and high-density lipoprotein) were analyzed by two-way analysis of variance followed by Fisher's Least Significant Difference post hoc test to evaluate the effect of 1-α-OH-vitamin D3 administration, GTPs levels, or interaction. Significant interactions between 1-α-OH-vitamin D3 and GTPs were tested using Fisher's Least Significant Difference tests to further define treatment effects (the L, LD, LG, and LGD groups). The level of significance was set at P<.05 for all statistical tests.
Results
Body weight
There was no significant difference in initial body weight among all treatment groups (229±23 g, 249±6 g, 248±5 g, 249±6 g, and 249±5 g for the P, L, LD, LG, and LGD groups, respectively). Over the course of the 3-month study, all animals gained body weight in a time-dependent manner. Neither 1-α-OH-vitamin D3 administration nor GTPs supplementation significantly affected body weights at the end of study (327±10 g, 316±6 g, 321±11 g, 315±6 g, and 301±5 g for the P, L, LD, LG, and LGD groups, respectively).
Histopathologic evaluation of heart
According to the Masson's Trichrome staining (in blue color), Figure 1 shows that after 3 months the L group (Fig. 1b) has stronger staining intensity of myocardial fibrosis in arterioles and surrounding myocardium than the P group (Fig. 1a). Both 1-α-OH-vitamin D3 administration and GTPs supplementation suppressed the intensity of myocardial fibrosis (Fig. 1). In addition, among the four LPS-treated groups, at 3 months the L group (Fig. 1b) had the strongest staining intensity of myocardial fibrosis around the arterioles (Fig. 1b–e for the L, LD, LG, and LGD groups, respectively). The results of the histological scoring were consistent with the observation of the staining images (data not shown).
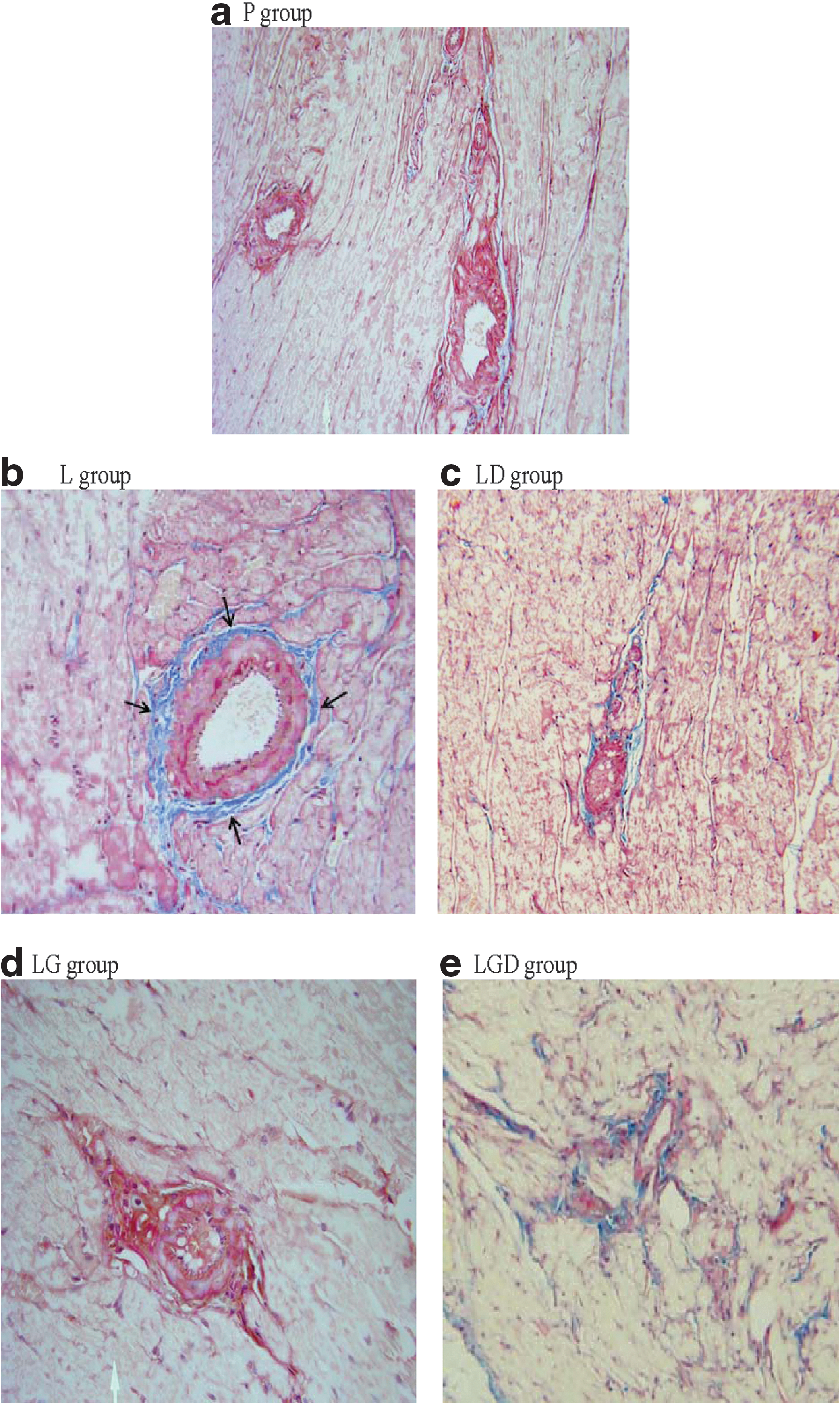
Representative sections of myocardium with Mason Trichrome staining (×20) from the
COX-2 mRNA expression in spleen
Figure 2 demonstrates the impact of 1-α-OH-vitamin D3 and GTPs supplementation on spleen COX-2 mRNA expression. The L group showed significant induction of mRNA expression of COX-2 in spleen relative to the P group. Based on the results of two-way analysis of variance, at 3 months both 1-α-OH-vitamin D3 administration and GTPs supplementation suppressed spleen mRNA COX-2 expression, and there was an interaction between 1-α-OH-vitamin D3 and GTPs.
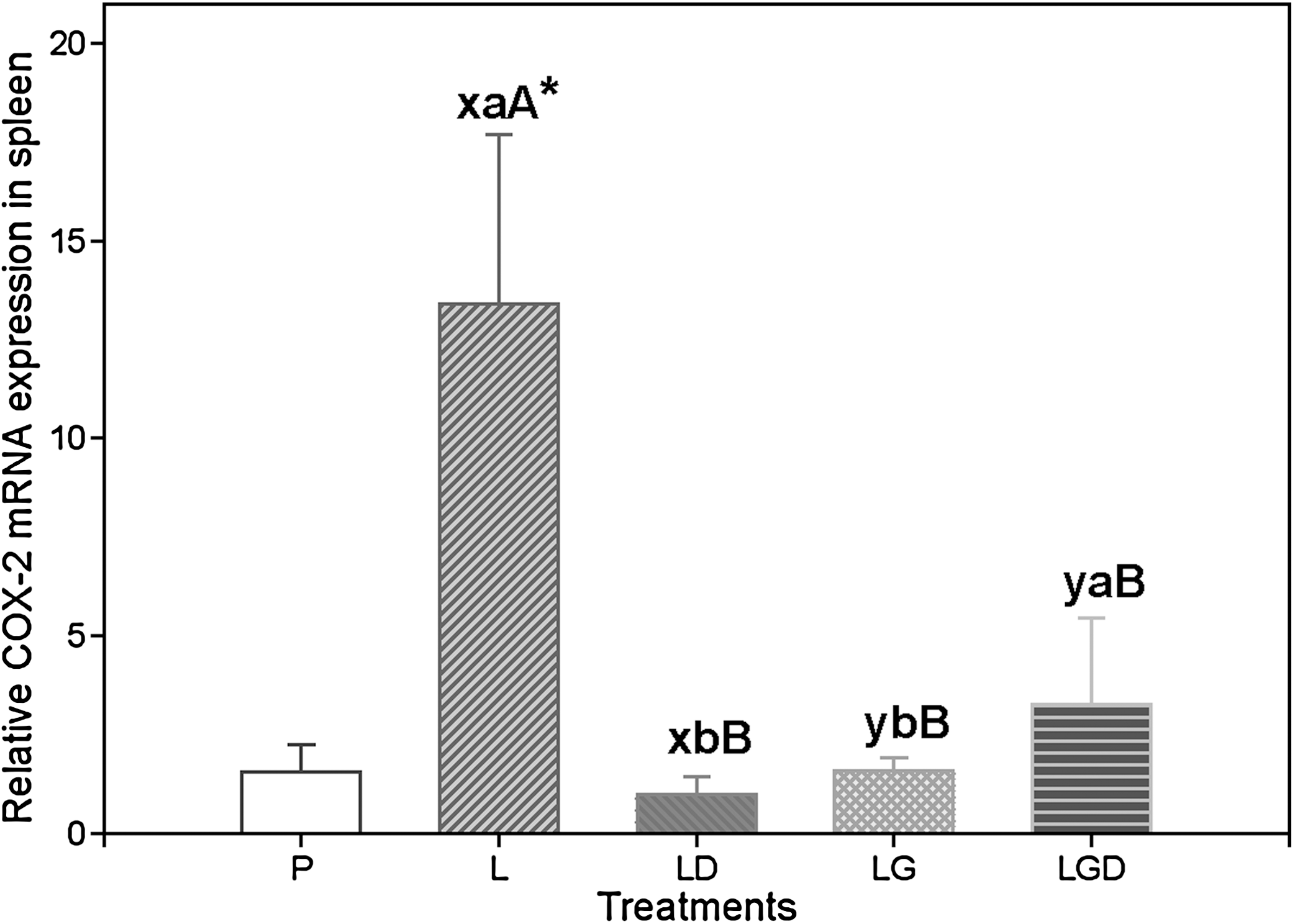
Relative mRNA expression of cyclooxygenase-2 (COX-2) in spleen of lipopolysaccharide-administered female rats given 1-α-OH vitamin D3 or supplemented with green tea polyphenols in drinking water for 3 months. Data are mean values (n=10) with their SEM represented by vertical bars. The difference between the P group and the L group was analyzed by t test to evaluate the effect of lipopolysaccharide administration. All the lipopolysaccharide-administered groups (L, LD, LG, and LGD groups) were analyzed by two-way analysis of variance to evaluate the effect of 1-α-OH-vitamin D3 administration, green tea polyphenols supplementation, or interaction. Significant interactions between 1-α-OH-vitamin D3 and green tea polyphenols were tested using Fisher's Least Significant Difference tests to further define treatment effects. *Significantly different from the P group (between the L group and the P group), P<.05; abfor 1-α-OH-vitamin D3 effect; xyfor green tea polyphenols effect; capital letters for interaction effect.
Blood leukocyte counts
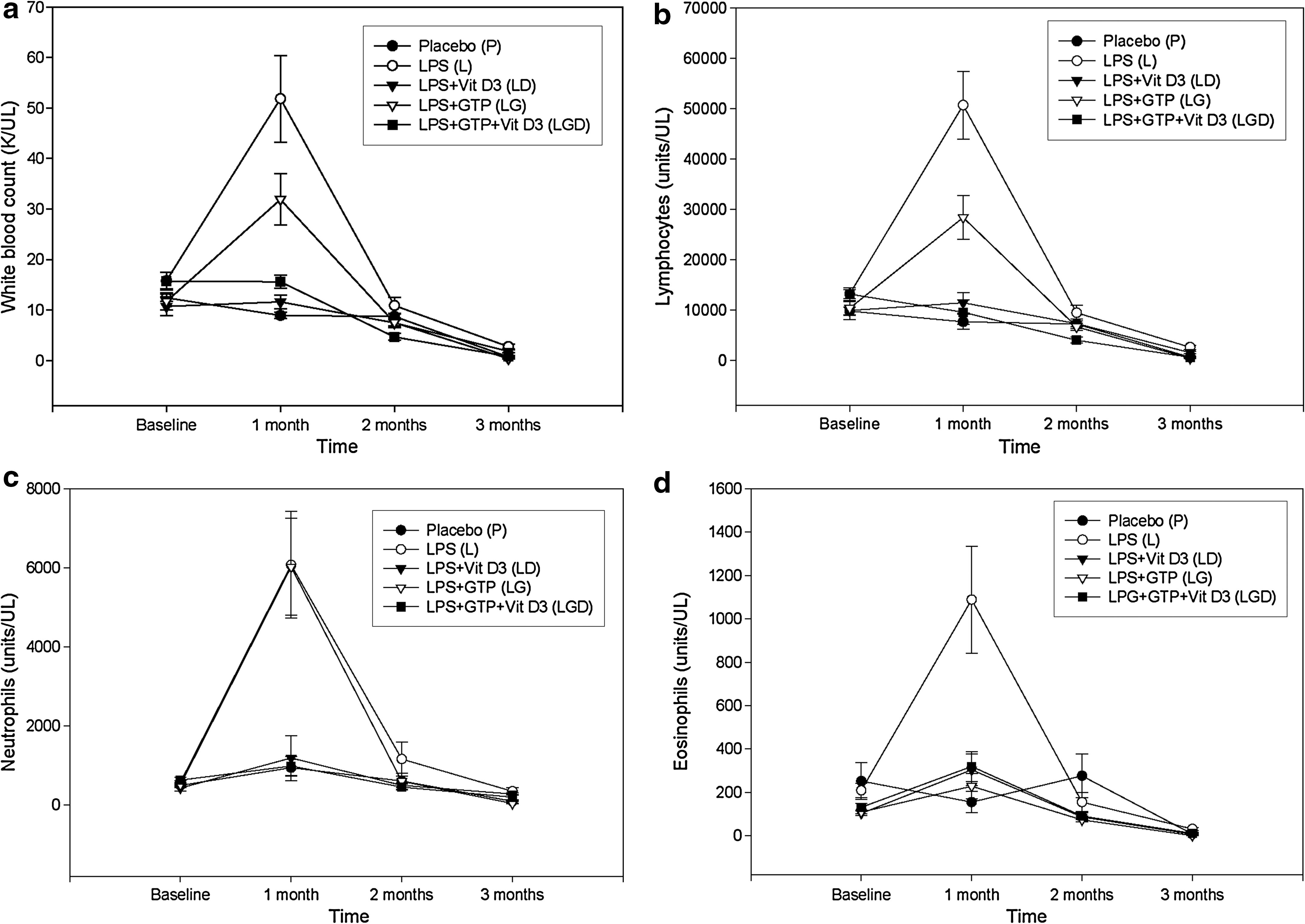
Figure 3 shows the effect of 1-α-OH-vitamin D3 administration and GTPs supplementation on hemopathologic readings. There was no difference in any blood leukocyte parameter, including WBCs (Fig. 3a), lymphocytes (Fig. 3b), neutrophils (Fig. 3c), and eosinophils (Fig. 3d), between the L group and the P group at baseline. Absolute WBC counts were significantly elevated in the L group relative to those in the P group at 1 month and at subsequent months (2 and 3 months) but to a lesser degree (Fig. 3a). Similar impacts of LPS administration and time on differential leukocytes, including lymphocytes (Fig. 3b), neutrophils (Fig. 3c), and eosinophils (Fig. 3d), in the L group were also observed compared with those in the P group. However, there was a significant decreased trend throughout the study period.
Effect of 1-α-OH-vitamin D3 (Vit D3) administration or green tea polyphenol (GTP) supplementation on
In terms of the four LPS-treated groups (L, LD, LG, and LGD groups), no difference was observed in any blood leukocyte parameters among these groups at baseline. In general, the results of two-way analysis of variance show both 1-α-OH-vitamin D3 administration and GTPs supplementation suppressed these parameters (WBCs, lymphocytes, neutrophils, and eosinophils shown in Fig. 3a–d, respectively) at various time points. There were significant interactions between 1-α-OH-vitamin D3 administration and GTPs supplementation in WBC counts, lymphocytes, and eosinophils at 1 and 3 months. The WBC, lymphocyte, neutrophil, and eosinophil counts were significantly decreased throughout the study period in a time-dependent pattern, regardless of the treatment groups.
RBC, Hct, and Hb levels
In terms of RBCs, Hct, and Hb, Table 1 shows that (1) there was no difference between the P group and the L group and (2) throughout the 3-month study period, there was no significant difference in any parameters between the L group and the P group, except for Hb levels at 1 month (19.0±0.4 and 15.7±0.1 g/dL for the L and P groups, respectively).
Results are expressed as mean±SEM values.
The difference between the P group and the L group was analyzed by t test to evaluate the effect of LPS administration. All the LPS-administered groups (L, LD, LG, and LGD groups) were analyzed by two-way analysis of variance (ANOVA) to evaluate the effect of GTP supplementation, 1-α-OH-vitamin D3 (D3) administration, or interaction. Significant interactions between GTP and D3 were tested using Fisher's Least Significant Difference tests to further define treatment effects (for the L, LD, LG, and LGD groups). The level of significance was set at P<.05 for all statistical tests. Means within a row having different superscripts (xyfor GTP effect; abfor D3 effect; capital letters for interaction effect) are significantly different by two-way ANOVA and Fisher's Least Significant Difference test (P<.05). *Significantly different from the P group (between the L group and the P group), P<.05.
Hb, hemoglobin; Hct, hematocrit; RBC, red blood cell.
There was a significant interaction between 1-α-OH-vitamin D3 administration and GTPs supplementation in RBCs (P=.011) and Hct (P=.003) at 1 month (Table 1). At 3 months, 1-α-OH-vitamin D3-administered groups had lower values for RBCs, Hct, and Hb compared with the non–1-α-OH-vitamin D3-administered groups. Similar to the findings for 1-α-OH-vitamin D3 administration, the GTPs supplementation also caused lower values for these parameters at 3 months. All these parameters were significantly reduced throughout the 3-month study period in a time-dependent manner, regardless of the treatment groups (L, LD, LG, and LGD groups).
Total lipid profiles
Throughout the study period, (1) there was no difference in any lipid profiles, including triglycerides, total cholesterol, low-density lipoprotein, and high-density lipoprotein, between the P and L groups (Table 2), (2) neither 1-α-OH-vitamin D3 administration nor GTPs supplementation influenced any lipid parameters, and (3) there was no interaction between 1-α-OH-vitamin D3 administration and GTPs supplementation affecting any lipid parameter (Table 2).
Results are expressed as mean±SEM values.
The difference between the P group and the L group was analyzed by t test to evaluate the effect of LPS administration. All the LPS-administered groups (L, LD, LG, and LGD groups) were analyzed by two-way ANOVA to evaluate the effect of GTP supplementation, D3 administration, or interaction. Significant interactions between GTP and D3 were tested using Fisher's Least Significant Difference tests to further define treatment effects (L, LD, LG, and LGD groups). The level of significance was set at P<.05 for all statistical tests. *Significantly different from the P group (between the L group and the P group), P<.05.
HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Discussion
In the present study, we successfully used an LPS-induced chronic systemic inflammation model to evaluate the effect of 1-α-OH-vitamin D3 administration plus GTPs supplementation on myocardial fibrosis. The present findings confirm that 3-month LPS administration significantly induced myocardial fibrosis in coronary vessels and surrounding myocardium. 18 The novel findings of this study were (1) 1-α-OH-vitamin D3 administration alone significantly mitigated myocardial fibrosis through a suppression of inflammation and innate immunity during chronic inflammation and (2) the impacts of 1-α-OH-vitamin D3 administration plus GTPs supplementation on myocardial fibrosis were individual effects.
The possible benefits of 1-α-OH-vitamin D3 5,9 and green tea 12 –16 on CVD have been documented. In a cohort of 242 patients with end-stage renal disease undergoing hemodialysis, the use of oral 1-α-OH-vitamin D3 was associated with reduced risk for cardiovascular death. 9 On the other hand, a population-based prospective cohort study showed that green tea consumption was associated with reduced CVD-caused mortality. 12 Our present results may provide, in part, a possible explanation for such cardioprotective roles of 1-α-OH-vitamin D3 and GTPs in humans.
In the present study, the inhibitory effects of treatment groups on myocardial fibrosis shown in histological staining seem to be equal (Fig. 1c, d, and e for the LD, LG, and LGD groups, respectively), indicating there is no additive or synergistic effect due to combined 1-α-OH-vitamin D3 and GTPs. We also observed similar inhibitory impacts of 1-α-OH-vitamin D3 and GTPs on the parameters of inflammation (e.g., COX-2 mRNA expression) and innate immunity (e.g., WBCs, leukocytes, neutrophils, and eosinophils), demonstrating no additive or synergistic effect. Our data show that 1-α-OH-vitamin D3 administration alone can significantly suppress both inflammation and innate immunity in this chronic inflammation model, resulting in almost the same response as that observed in the placebo group. Because the combined 1-α-OH-vitamin D3 and GTPs treatment cannot demonstrate a response exceeding the placebo group, this is why no additive or synergistic effect was observed as such a ceiling effect masks the additive or synergistic potential of GTPs supplementation. Another possible reason is that the short duration of treatment and higher dosage of 1-α-OH-vitamin D3 and GTP might have resulted in this nonsignificant effect.
One of the goals of the present study was to explore the molecular mechanism of 1-α-OH-vitamin D3 and GTPs in averting myocardial fibrosis and vascular deterioration in rats during chronic inflammation. Valen et al. 25 reported that certain stimuli, including reactive oxygen species, oxidants (i.e., oxidized low-density lipoprotein), and cytokines, induce the redox-sensitive molecule NF-κB and that such an activation of NF-κB plays an important role in the progression of atherosclerosis, myocardial infarction, and cardiac dysfunction. The activated NF-κB also induces transcription of COX-2, TNF-α, and inducible nitric oxide synthase. 25 In particular, COX-2 is a key enzyme catalyzing the production of PGE2 in response to inflammatory stimuli, and it plays a prominent role in myocardial infarction. 26 Therefore, the suppression of inflammatory responses may be an important therapeutic strategy for the treatment of chronic inflammation-induced CVD such as myocardial fibrosis.
The observation of the inhibitory effect of 1-α-OH-vitamin D3 on spleen COX-2 mRNA expression is supported by other findings in various inflammation models. For example, Giulietti et al. 11 reported that activated vitamin D suppressed the expression levels of COX-2, TNF-α, IL-6, and IL-8 in monocytes isolated from patients with type 2 diabetes compared with those from type 1 diabetes. Krishnan et al. 27 found that 1-α-OH-vitamin D3 inhibits the synthesis and actions of pro-inflammatory PGs in three ways: (1) by suppressing the expression of COX-2 (the enzyme that synthesizes PGs), (2) by inducing expression of 15-PG dehydrogenase (the enzyme that inactivates PGs), and (3) by inhibiting the expression of PGE and PGF receptors (the receptors that mediate PG signaling) in the progression of prostate cancer.
Similar to the impact of 1-α-OH-vitamin D3 on COX-2 mRNA expression, the finding that GTPs supplementation significantly down-regulated chronic inflammation-induced COX-2 mRNA expression in spleen supports our hypothesis that LPS-induced myocardial fibrosis in female rats can be mitigated by GTPs supplementation through a reduction of COX-2. The capacity of GTPs to suppress the LPS-induced COX-2 expression in rats agrees with the observation by Tipoe et al. 28 that epigallocatechin-3-gallate significantly reduced chronic CCl4-induced liver injury and fibrosis via reducing the pro-inflammatory response (mRNA expression of COX-2, TNF-α, and inducible nitric oxide synthase). In addition, other studies have also shown that (1) epigallocatechin-3-gallate significantly suppressed cellular PGE2 biosynthesis in LPS-stimulated human whole blood through an inhibition of the microsomal PGE2 synthase-1 mechanism, 29 (2) epigallocatechin-3-gallate significantly inhibited cigarette smoking-induced myocardial injury/dysfunction through a suppression of NF-κB, COX-2, TNF-α, and inducible nitric oxide synthase in the heart of cigarette smoke-exposed rats, 30 and (3) epigallocatechin-3-gallate decreased the level of COX-2 protein and PGE2 in IL-1β-induced inflammatory human chondrocytes. 31
The present study also demonstrates the inhibitory impact of 1-α-OH-vitamin D3 and GTPs on the innate immune response. Chronic release of LPS (33 μg/day for 3 months continuously) induced innate immune responses, as shown in an increase in WBCs, lymphocytes, neutrophils, and eosinophils, in the LPS-treated rats. 19 Such an elevation in innate immune response is detrimental to myocardium of the LPS only–treated rats, as demonstrated in myocardial fibrosis of the L group (Fig. 1b). Albelda et al. 32 reported that lymphocyte infiltration into the myocardium corresponded to the area of fibrosis and also up-regulation of pro-inflammatory mediators (i.e., COX-2 and TNF-α).
Our data show that 1-α-OH-vitamin D3, GTPs, and the combined treatment not only suppressed COX-2 mRNA expression, but also inhibited the circulating WBCs, lymphocytes, neturophils, and eosinophils (Fig. 3). These findings further confirm our hypothesis that LPS-induced myocardial fibrosis in the female rats can be mitigated by 1-α-OH-vitamin D3 administration and GTPs supplementation. Our observations of 1-α-OH-vitamin D3 administration on inhibition of the innate immune response are supported by McMahon et al., 33 who observed that treating human gingival epithelium with activated vitamin D suppressed the innate immune response in macrophages. A recent review article by Bartley 34 further addressed an emerging critical role of vitamin D in suppression of the innate immune system in respiratory tract, skin, and potentially intestinal health, through the production of antimicrobial peptides, especially cathelicidin. Additionally, such findings of the inhibitory effect of GTPs on the innate immune response agree with others. 35 –37 Raemsh et al. 35 reported that epigallocatechin-3-gallate significantly suppressed levels of C-reactive protein, WBCs, lymphocytes, and neutrophils in rats fed with an atherogenic diet. Dona et al. 36 found that oral green tea extract administration significantly decreased the intensity of fibrosis in a pulmonary inflammation model. Studies also show that green tea was involved in the suppression of neutrophil migration 38 and a reduction of monocyte adhesion on endothelial cells in cultured human endothelial monolayers. 37
During the inflammation response, the presence of damaged/dysfunctional RBCs has been linked to adverse clinical CVD effects. 39 Relative to the P group, the L group had a significantly higher circulating Hb concentration at 1 month. Such high levels of Hb may be released from the stressed RBC 40 with an increased fragility of erythrocyte members due to LPS administration, 41 although we did not observe a significant difference in RBC counts between the P group and the L group. In this study, both 1-α-OH-vitamin D3 administration and GTPs supplementation showed the same decreased trend on circulating RBCs, Hct, and Hb. Sih et al. 42 found that 18-month ingestion of a high concentration of vitamin D3 (cholecalciferol) by cats increased serum blood urea nitrogen and calcium levels but decreased RBC, serum total protein, albumin, and Hb concentrations. On the other hand, studies have demonstrated that epigallocatechin-3-gallate, rich in antioxidants, is capable of protecting erythrocyte membranes against oxidation-induced damage in vitro. 43,44
In addition to the main focus on myocardial fibrosis, we further assessed the effect of 1-α-OH-vitamin D3 and GTPs on lipid profiles in the same model. However, we were not able to observe any effects of 1-α-OH-vitamin D3 and GTPs on these serum lipid parameters. We speculate that the 3-month study length was probably too short to cause any abnormal lipid profile, as shown by no difference in any lipid parameters between the P group and the L group (Table 2). This is probably why the potential impact of 1-α-OH-vitamin D3 and GTPs on lipid profiles may be minimal and undetectable. Furthermore, we did not observe any plaque formation in this model (data not shown), probably also because of such a short study length. Fibrosis of the myocardium may take a shorter time than the development of atherosclerosis with evidence of plaque formation. Future studies may use the same LPS administration model with a longer study length in order to see the impact of treatments on abnormal lipid profiles and plaque formation.
Conclusions
The present study demonstrates the beneficial effects of 1-α-OH-vitamin D3 administration and GTPs supplementation on attenuating myocardial fibrosis in an LPS-induced chronic systemic inflammation animal model. Such protective roles of 1-α-OH-vitamin D3 and GTPs may be due to an inhibition of the pro-inflammatory cytokine mediator, COX-2, and to the innate immune response. The inhibitory effects of 1-α-OH-vitamin D3 and GTPs seem to be an individual effect, instead of any additive or synergistic effect.
Footnotes
Acknowledgments
This work was supported by the Laura W. Bush Institute for Women's Health.
Author Disclosure Statement
No competing financial interests exist.