
Abstract
Free radicals induced by cigarette smoking have been strongly linked to increased oxidative stress in vivo, contributing to the pathobiology of various diseases. This study was performed to investigate the effects of Haematococcus astaxanthin (ASX), which has been known to be a potent antioxidant, on oxidative stress in smokers. Thirty-nine heavy smokers (≥20 cigarettes/day) and 39 non-smokers were enrolled in this study. Smokers were randomly divided into three dosage groups to receive ASX at doses of 5, 20, or 40 mg (n=13, each) once daily for 3 weeks. Oxidative stress biomarkers such as malondialdehyde, isoprostane, superoxide dismutase, and total antioxidant capacity, and ASX levels in plasma were measured at baseline and after 1, 2, and 3 weeks of treatment. Compared with baseline, the plasma malondialdehyde and isoprostane levels decreased, whereas superoxide dismutase level and total antioxidant capacity increased in all ASX intervention groups over the 3-week period. In particular, isoprostane levels showed a significant dose-dependent decrease after ASX intake. The results suggest that ASX supplementation might prevent oxidative damage in smokers by suppressing lipid peroxidation and stimulating the activity of the antioxidant system in smokers.
Introduction
C
Recently, astaxanthin (ASX) (3,3′-dihydroxy-β,β′-carotene-4,4′-dione), a red carotenoid pigment with no pro-vitamin A activity, has attracted a great deal of attention due to its multiple functions and antioxidant potential, which have been reported to surpass those of β-carotene or even α-tocopherol. 6,7 The potent antioxidant properties of ASX are believed to have a key role in protection against a wide range of ailments, such as inflammation, cardiovascular diseases, cancer, and immunological disorders. 8,9
There have been several recent studies on the actual benefits of ASX as a dietary supplement, but these have been limited to in vitro assays or preclinical trials. 8,9 Moreover, to our knowledge, ASX has not been studied in healthy smokers who are under oxidative stress in daily life. Therefore, we conducted a clinical trial in heavy smokers to evaluate whether ASX supplementation can change several plasma biomarkers that are indicative of oxidative stress, as well as the antioxidant system. In addition, the absorption of ASX into the blood from a soft capsule and its safety were evaluated.
Materials and Methods
Subjects
Eligibility criteria included heavy smoking of ≥20 cigarettes/day for at least the past year and willingness to stop consuming vitamin supplements for the duration of the study. Exclusion criteria were as follows: reported consumption of four or more servings of fruit and vegetables per day, alcohol consumption, pregnancy or lactation, lipidemia, hyperglycemia, or the presence of chronic diseases. Non-smokers who had never smoked cigarettes, matched by sex and age, were also enrolled in the study as controls.
All subjects were considered healthy according to medical history, physical examination, and laboratory investigation. All subjects were asked to maintain their current lifestyle and smoking habit and to refrain from taking any vitamins or antioxidant supplements. We offered anti-smoking education after the study termination for ethical reasons. The protocols were approved by the Institutional Review Board of Seoul National University Hospital (Seoul, Korea), and written consent was obtained from all subjects prior to the study.
Study design
Smokers were randomly assigned to one of three doses of ASX—5, 20, or 40 mg—in a softgel capsule. The subjects were instructed to take a capsule once daily with a meal, based on the long half-life and lipophilic property of ASX, 10 from the baseline blood sampling to the day before their final blood sample was taken. Subjects visited Seoul National University Hospital at the time of baseline blood sampling and at 1, 2, and 3 weeks after ASX intake. Blood and urine samples were collected at each visit. At the final visit, the subjects were required to return their ASX capsule bottles, and the remaining capsules were counted to assess adherence. Adverse events were assessed by questionnaire and spontaneous reporting during the study days.
The natural source of ASX was homogenized, spray-dried cells of the unicellular microalga Haematococcus pluvialis (Algatechnologies Ltd., Kibbutz Ketura, MP Eilot Corridor, Israel). H. pluvialis is the richest source of natural ASX, as well as one of only a few sources of microbial origin that can compete economically with synthetic ASX. 9 The ASX in H. pluvialis occurs in the esterified and all SS (3S,3′S stereoisomer) form, which is more stable than the free form. The softgel capsules were manufactured and provided by Marine Product Tech. Inc. (Seongnam, Korea). The capsules were soybean oil-based, which could have increased oral bioavailability of ASX, 10 and were assayed to confirm their composition.
Blood sampling and laboratory tests
A 10-mL blood sample was taken via a cannula in the antecubital fossa between 8 and 9 a.m. after an overnight fast. The sample was placed in a tube containing EDTA and centrifuged at 4°C to minimize the effect of temperature on the plasma concentrations of oxidative stress markers. Urine samples were also collected at the same time. All samples were stored at −70°C until used for analysis. Repeated freeze–thaw cycles were avoided. The samples were kept in an ice bath and protected from light during the entire process.
As biomarkers of in vivo lipid peroxidation, the plasma free malondialdehyde (MDA) and free isoprostane (ISP) (also known as 15-isoprostane F2t) levels were measured by enzyme-linked immunosorbent assay (Oxford Biomedical Research Inc., Oxford, MI, USA). As biomarkers of the antioxidant system, superoxide dismutase (SOD) (Dojindo Laboratories Inc., Kumamoto, Japan) and total antioxidant capacity (TAC) (Oxford Biomedical Research Inc.) levels were measured by enzyme-linked immunosorbent assay. Plasma levels of ASX were determined by high-performance liquid chromatography. 10 We also measured the urinary concentrations of cotinine, which is a metabolic end-product of nicotine, by liquid chromatography–tandem mass spectrometry 11 (limit of quantification, 0.01 ng/mL) before and after treatment with ASX, to confirm smoking status.
All subjects completed a lifestyle and food frequency questionnaire that produced estimates of macro- and micronutrient intake. Other data obtained included smoking history, number of cigarettes smoked per day, and years of smoking (Table 1). All subjects underwent blood analysis, such as complete blood cell count and basic metabolic panel, which include determination of hemoglobin, lymphocytes, white blood cell count, red blood cell count, platelet, calcium, phosphorus, glucose, blood urea nitrogen, uric acid, total bilirubin, alkaline phosphate, alanine aminotransferase, aspartate aminotransferase, creatinine, Na, K, Cl, total CO2, serum albumin, C-reactive protein, erythrocyte sedimentation rate, total cholesterol, and triglycerides before and after ASX treatment. Those parameters were evaluated to determine biochemical status before and after treatment and test the safety of ASX.
Baseline data are from prior to astaxanthin (ASX) intervention. Results are reported as mean±SD or number (%).
Median (range).
Number of “yes” responses.
Percentage of Korean recommended dietary allowances.
No dose group differences in all data were statistically significant. Some differences were significantly different (* P<.05, ** P<.01) from non-smokers using the t test.
BMI, body mass index; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; NA, not applicable; TGs, triglycerides; TLC, total lymphocyte count (=white blood cell [WBC] count×lymphocytes [%]).
Statistical analysis
The sample size was estimated with two-sided 5% significance and 80% power. Data were tested for normality using the Kolmogorov–Smirnov test. ASX dosage groups were compared by independent-sample t test and one-way analysis of variance. Student's paired t test was used to assess the differences according to ASX intervention time within the same dosage group. A multivariate correlation analysis was used to evaluate the relationship between parameters using Pearson correlation coefficients. Results are presented as mean±SD values. SPSS version 15.0 software (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses, and P<.05 was taken to indicate statistical significance.
Results
Baseline characteristics
Baseline characteristics, including lifestyle and smoking history, are listed in Table 1. Thirty-nine smokers (38 men and one woman; median age, 24 years) and 39 non-smokers (38 men and 1 woman; median age, 26 years) were enrolled in this study. Smokers smoked 21±2 cigarettes/day for 7±4 years. Smoking history, including cigarettes smoked/day (r=0.350, P<.01) as well as years of smoking (r=0.464, P<.01), was significantly correlated with urinary levels of cotinine (data not shown). Duration of smoking was also significantly correlated with baseline plasma levels of triglycerides (r=0.449, P<.01) and MDA (r=0.399, P<.05) (data not shown).
Gender, age, and body mass index were comparable between smokers and non-smokers among the three ASX dosage groups. Nutrient intake, baseline plasma levels, and urinary levels of cotinine were also comparable among the three dosage groups (Table 1). The smokers were verified by measuring their urinary levels of cotinine, which is a known indicator of long-term exposure to tobacco smoke. 12 This excludes the possibility of misclassification due to self-reported information on smoking. In addition, no significant differences in urinary levels of cotinine before and after ASX intervention were observed. This suggests that the smokers did not change their smoking habit during the study and that possible changes in oxidative stress biomarkers were not due to changes in cigarette consumption.
Plasma levels of ASX
The plasma levels of ASX at baseline and during 1, 2, and 3 weeks of ASX administration are shown in Figure 1. In all three ASX dosage groups, the plasma levels of ASX were significantly higher than at baseline. Compared with the 5 mg ASX group, the plasma levels of ASX were significantly higher in the 20 and 40 mg groups at 1, 2, and 3 weeks. There was no significant difference between the 20 and 40 mg groups.
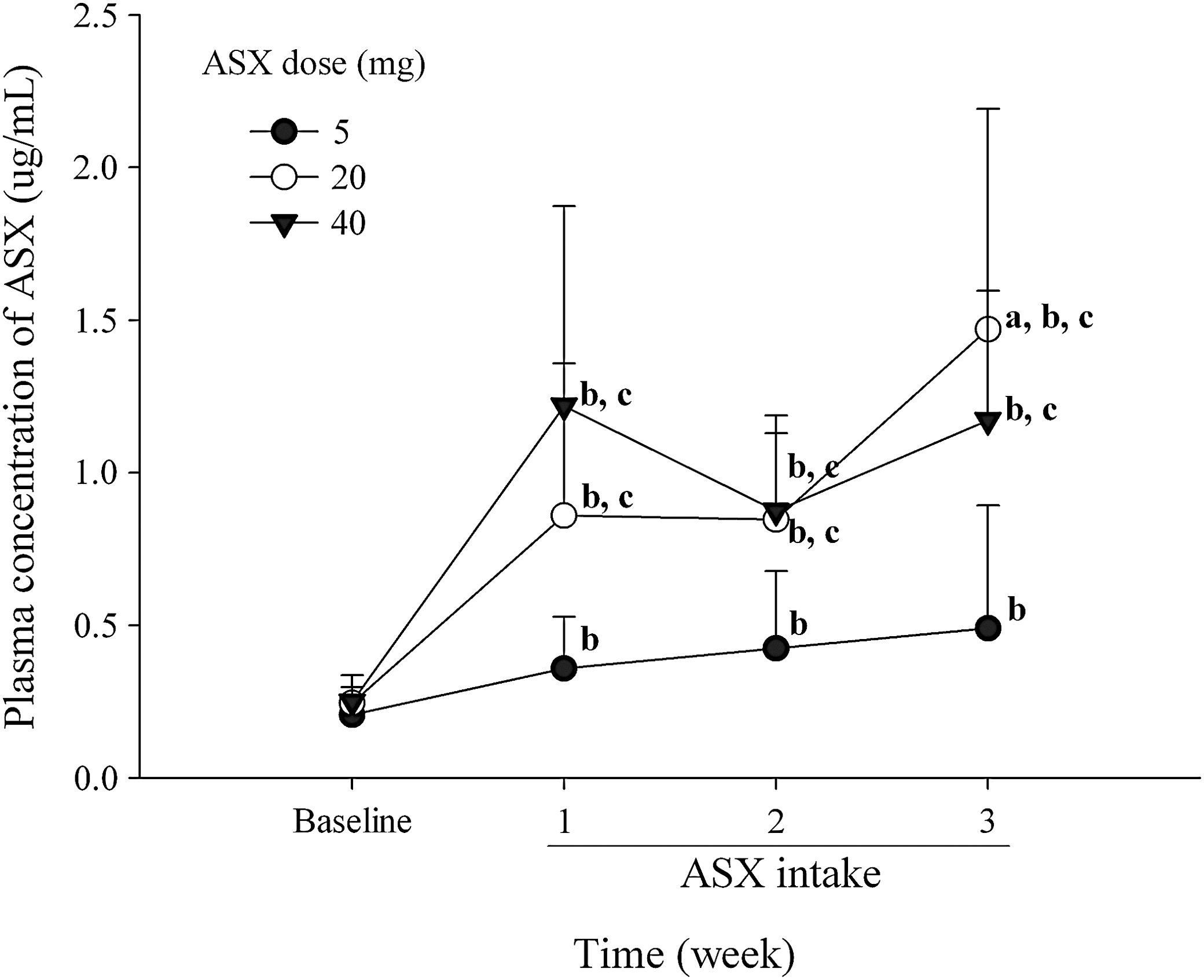
Mean plasma concentrations of ASX at baseline and 1, 2, and 3 weeks after daily oral administration of 5 mg (•), 20 mg (○), and 40 mg (▾) of ASX (n=13 each). Bars represent SD. abcValues significantly different (P<.05) from the previous week, baseline, and each dose, respectively.
Effects of ASX on plasma MDA and ISP levels
Plasma levels of MDA and ISP in the smokers and non-smokers are shown in Figure 2. Compared with the baseline values of non-smokers, the baseline plasma levels of MDA and ISP were significantly higher in all groups of smokers, except for ISP at 3 weeks. Compared with the baseline values of smokers, the plasma levels of MDA and ISP were significantly lower after ASX supplementation over the 3-week study period, except in the 5 mg group at 1 week. Although the plasma levels of MDA were comparable at 1, 2, and 3 weeks after ASX intervention, the plasma levels of ISP significantly decreased in a time-dependent manner, with increasing duration of ASX treatment. The baseline plasma levels of MDA and ISP did not differ significantly among the three dosage groups. Although the plasma levels of MDA were comparable among the 5, 20, and 40 mg ASX groups, the plasma levels of ISP were significantly decreased in the 20 and 40 mg groups compared with the 5 mg groups after 3 weeks. In addition, the plasma levels of ISP were negatively correlated with SOD activity after 3 weeks of ASX intake (r=−0.425, P<.01; data not shown). The baseline MDA and ISP levels were barely correlated with each other (r=−0.0520, P=.753; data not shown).

Mean plasma levels of (
Effects of ASX on plasma SOD and TAC levels
Plasma levels of SOD and TAC in the smokers and non-smokers are shown in Figure 3. Compared with baseline values of non-smokers, the baseline plasma levels of SOD and TAC were significantly lower in smokers, except for SOD in the 20 mg group at 3 weeks. Compared with baseline values of smokers, the levels of SOD and TAC were significantly higher for 3 weeks, except for TAC in the 40 mg group at 1 week. After 3 weeks of intervention, the plasma levels of SOD and TAC tended to increase with intervention time. There were no significant changes in the plasma levels of SOD and TAC among the three dosage groups for 3 weeks. The baseline TAC levels in smokers were positively correlated with serum albumin (r=0.353, P<.05) but negatively correlated with white blood cell counts counts (r=−0.336, P<.05) (data not shown). The baseline levels of SOD and TAC were barely correlated with each other (r=−0.0450, P=.784; data not shown).
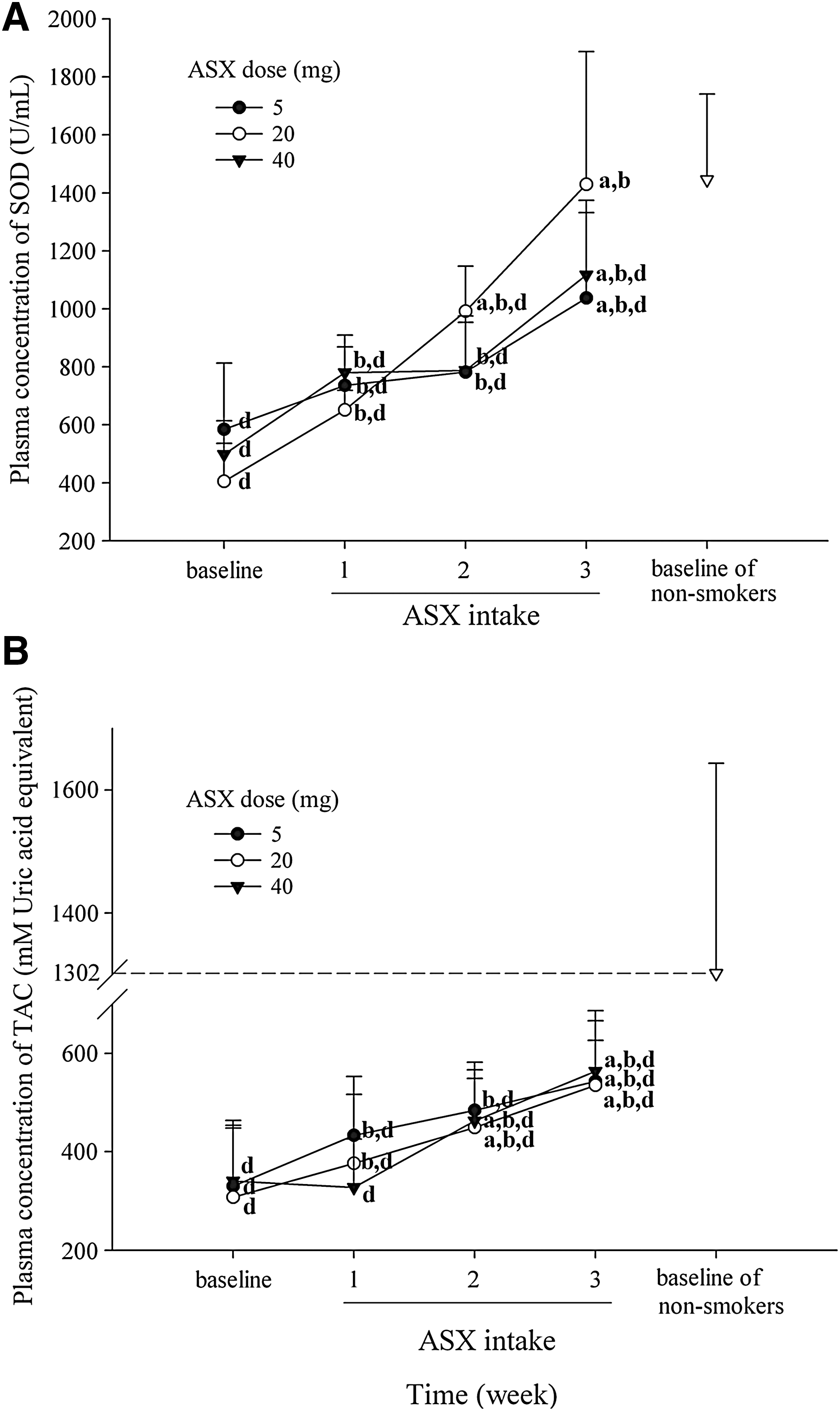
Mean plasma levels of (
Safety of ASX
The adherence rate as measured by ASX capsule count was 97.0%. Changes in the plasma levels of ASX (Fig. 1) also demonstrated that subject compliance was quite good. ASX was well absorbed and well tolerated by the subjects. A complete medical examination and blood tests after ASX intervention showed that there were no adverse effects or toxicity from ingestion of ASX, except for changes in fecal color to red (n=2, 5.13%), which could have been due to the reddish color of ASX itself.
The blood tests revealed no significant differences between before and after 3 weeks of intervention with ASX, except for white blood cell count, erythrocyte sedimentation rate, platelet count, phosphorus, glucose, alkaline phosphate, and total CO2 (P<.05, paired t test) (Table 2). Although the differences were statistically significant, they were very small, and all data were within normal ranges, so the differences seemed to be no clinical importance.
Data are mean±SD values.
Data prior to ASX intake.
Data after 3 weeks of ASX intake.
By paired t-test.
ALT, alanine transaminase; AST, aspartate transaminase; BUN, blood urea nitrogen; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; MPV, mean platelet volume; NS, not significant; PDW, platelet distribution width; RBCs, red blood cells; RDW, red blood cell distribution width; TCO2, total CO2; WBCs, white blood cells.
Discussion
To our knowledge, this is the first intervention study to determine the plasma levels of ASX in smokers and to show the in vivo relationship between biomarkers of oxidative stress and ASX supplementation. In smokers, increased oxidative stress markers, such as significantly higher plasma levels of MDA and ISP, and lower levels of SOD and TAC were observed compared with the non-smokers. In addition, smoking history was correlated with MDA, as described previously. 3 These results support the suggestion that smoking is, at least in part, responsible for the oxidative damage that is represented by increased lipid peroxidation and inhibition of antioxidant enzymes in smokers. We also evaluated variations in oxidative status among smokers after dietary supplementation with 5–40 mg of ASX. Daily supplementation with ASX for 3 weeks significantly decreased the plasma levels of MDA and ISP and increased the plasma levels of TAC and SOD in all dosage groups compared with the baseline levels before ASX intervention. This suggests that ASX is an effective antioxidant against oxidative stress, which can change the plasma levels of oxidative stress biomarkers in smokers.
The results of this study may be especially significant in the following situations. First, we detected multiple concomitant oxidative stress biomarkers in smokers—MDA and ISP, as biomarkers of lipid peroxidation, and SOD and TAC, as biomarkers of the antioxidant system—and proved that they are reliable markers of oxidative damage. Second, we determined the dose-related effect of ASX by dividing the subjects into three dosage groups.
The main aim of this study was to evaluate the protective effect of ASX as an antioxidant in smokers. After ASX intervention, consistent with the marked increase in plasma ASX level, we observed constant and significant decreases in the plasma levels of MDA and ISP. MDA is a decomposition product of peroxidized polyunsaturated fatty acids in membrane lipids, which are thought to be the most sensitive biological molecules in terms of susceptibility to reactive oxygen species. ISPs are eicosanoids that are produced by free radical–catalyzed oxidation of arachidonic acid. These are widely used and reliable biomarkers of in vivo lipid peroxidation and oxidative stress in a range of disease conditions. 13 Therefore, our study suggests that ASX may play a pivotal role in protecting membranous phospholipids and other lipids against peroxidation. 6,7
With regard to antioxidant biomarkers, we showed increased plasma levels of SOD and TAC with increasing duration of ASX intake. SOD is the main in vivo antioxidant enzyme that quenches superoxide anions, and TAC represents a full spectrum of antioxidant activity against various reactive radicals. In vitro studies have found that ASX has cellular effects by scavenging biologically produced free radicals and reactive oxygen species, including superoxide anions, which are known to be present in cigarette smoke. 2,8,9 In addition, TAC is positively correlated with albumin, which is a serum antioxidant agent and can be oxidized by the gas phase of smoking, 14 which was consistent with previous results. 15 Our changes in SOD and TAC clearly reveal that ASX raises overall antioxidant activity by its ability to increase the activities of radical scavenging enzymes 16,17 in smokers.
The 50% effective dose of ASX as a free radical scavenger has been reported to be 200 nM. 18 In the present study, the minimum concentration of ASX in plasma was 603 nM in the 5 mg group after 1 week of intake. This suggests that 5 mg/day ASX for 1 week can elevate its plasma concentration to an effective level and seems to be sufficient to have an antioxidant effect.
The recommended dose of ASX for healthy adults is reported to be 5–6 mg/day worldwide. 19 The dose range of 5–40 mg, which is within the safe dosage range already established in other studies, 10,19 was used without any adverse events in our study. The plasma concentrations of ASX were comparable between the 20 and 40 mg groups (Fig. 1), and this could have been due to the saturation of absorption of ASX at high doses. 20 ISP levels were also not significantly different between the 20 and 40 mg dosage groups, although they were significantly different between the 5 and 20 mg dosage groups. This can be explained by the properties of carotenoids, which can lose their effectiveness as antioxidants at high concentrations. 21 Given the complexity of the biological mechanisms of ASX, further studies are needed to clarify this issue.
As mentioned earlier, ASX has been considered a super-vitamin E becasue of its superior antioxidant properties compared with other antioxidants. 6,7 Nonetheless, direct comparison of the results of the present clinical intervention with other studies of ASX is difficult, as no precedent exists for similar evaluations, and most reports of the biological efficacy of ASX have been limited to in vitro and animal studies. Many animal studies have indicated the positive effect of ASX as an antioxidant in diverse pathological conditions, 16,17 and one study showed that ASX was not effective against lipid peroxidation in male chicks. 22 However, the biomarker of lipid peroxidation in that study was thiobarbituric acid–reactive substances, which is known to be nonspecific. In addition, the protective effect of ASX has been confirmed recently in a few human clinical studies of cardiovascular disease, 23 male infertility, 24 and Helicobacter pylori infection 25 and even in healthy non-smokers. 26
In conclusion, our study indicated that the increased level of oxidative stress seen in smokers can be reduced by the intake of ASX, and it can be safely consumed by healthy adults. A possible mechanism for the protective effect of ASX is the elevation of TAC by suppression of lipid peroxidation and activation of antioxidant enzymes. Our results suggest that, due to its well-documented safety profile, 25 ASX is one of the most potent preventive agents for smoking-induced oxidative stress and that ASX supplementation may be effective for reducing the risk of pathological conditions related to oxidative stress in general, as well smoking-induced oxidative stress. Further placebo-controlled studies in larger populations and for longer periods are required to confirm our preliminary findings.
Footnotes
Acknowledgments
This work was supported by grant A050376 of the Korea Health 21 R&D Project, Ministry of Health and Welfare, Korea. The authors would like to thank all subjects who participated in this study.
Author Disclosure Statement
No competing financial interests exist.