
Abstract
The objective of this systematic review was to assess the evidence from rigorous clinical trials evaluating the efficacy of mixed herbal medicine formulations used in traditional Oriental medicines for the treatment of obesity and to describe the safety and types of adverse events reported in such trials. To accomplish this, 14 databases were searched from inception to July 31, 2009. The search terms used were “obesity” or “obese” and “herb,” “herbal,” or “herbal medicine” without language restriction. All randomized clinical trials using mixed herbal medicines on obese or overweight subjects were considered for inclusion. Of the publications in the identified databases, 1144 results were searched and reviewed, and in total 12 studies were included. Their methodological quality was assessed using the Jadad score. The results of our review provide evidence suggesting that mixed Oriental herbal medicines may be safe and effective for the treatment of obesity when compared with conventional medicine, placebos, or lifestyle control. Many trials also reported improved concomitant conditions including impaired glucose tolerance, hypertension, and inflammation. Small numbers of adverse events were reported, but most were mild or not related to the intervention in itself. No significant mortality was observed in any of the trials. However, the evidence provided by the trials reviewed is not fully convincing because of their poor methodological quality. Therefore, more research and well-designed clinical trials are necessary to address these issues, as well as to assess the safety of mixed Oriental herbal medicines used to treat obesity.
Introduction
T
Accordingly, there is a tendency for individuals to use complementary and alternative medicine for the treatment of obesity. Herbal medicine is one of the most widely used therapies for the treatment of obesity among current modalities of complementary and alternative medicine. The growing popularity of these remedies is fueled by increasing scientific interest in herbal medicines. 6 However, there are still conflicting opinions regarding the efficacy of such treatments because of the lack of evidence of their effectiveness and safety. Herbal supplements are marketed as food supplements in many countries and are therefore subject to less stringent control than drugs. In the United States, some herbal weight loss supplements have been tested for effectiveness in clinical trials, but there is little evidence available for most supplements on the market. 7 Additionally, the use of some herbal supplements containing ephedrine has been controversial because of the possibility of adverse events. 8 For these reasons, there is a need to evaluate scientific evidence regarding the effectiveness of herbal medicines using rigorous clinical trials.
Herbal medicines are generally used as a mixture of various herbs based on traditional Oriental medical theory, which usually does not prescribe a single herb for the patients. The effects of mixed herbal medicines are influenced by the interaction of various herbs. 9 More specifically, in a mixed herbal formulation, the component herbs produce synergistic beneficial effects, while the adverse side effects of any individual component are attenuated by the others. Therefore, it is conceivable that the mode of action of a formulation of mixed herbal medicines is complex in nature, and the therapeutic efficacy of the formulation is not simply the sum of the effects of the individual component herbs. Accordingly, the clinical trials that were conducted to evaluate the treatment effects of mixed Oriental herbal medicines were evaluated in this study rather than the effects of single herbs.
The goal of this systematic review was to assess the evidence produced by rigorous randomized clinical trials (RCTs) conducted to evaluate the effectiveness of Oriental herbal medicines for obesity. In addition, the safety and types of adverse events reported in clinical trials are discussed, and future studies regarding the present subject are suggested.
Subjects and Methods
Data sources
The following databases were searched from inception to July 31, 2009: National Library of Medicine Medline (PubMed), EMBASE, Science Direct, the Cochrane Library, EBSCOhost, one Japanese database (CiNii [Scholarly and Academic Information Navigator]), one Chinese database (CAJ [China Academic Journal]), four Korean databases (DBPIA, National Assembly Library, Research Information Service System, and Korean Studies Information Service System), and four Korean medical journals relevant to obesity (Journal of Oriental Medicine, Journal of Oriental Physiology and Pathology, Journal of Oriental Rehabilitation Medicine, and Journal of Korean Oriental Association for Study of Obesity). The search terms used were “herb,” “herbal,” or “herbal medicine” and “obesity” or “obese.”
Study selection
RCTs were searched to assess the efficacy of mixed herbal medicines in traditional Oriental medicines for the treatment of obesity in human subjects. A study that stated the phrase “randomization” in its text was regarded as a randomized trial. Trials using mixed herbal medicines that were based on traditional Oriental medicine theory were included. Participants clearly defined as overweight or obese at baseline were included. Overweight or obesity definitions were either body mass index (BMI) cutoff points (≥25 kg/m2) or obesity degree cutoff points (≥110%). 10 Trials comparing herbal medicines with any type of control interventions were included, and the primary outcome measures were BMI, body weight, body fat percentage, and waist or hip circumference.
Studies utilizing herbal treatments that did not comply with Oriental medical theory were not included in this review. Accordingly, we excluded trials in which only a single herb or dietary supplement was used for treatment intervention. Trials that compared different forms of herbal medicines with each other or did not use a herbal medicine for the main treatment intervention were also excluded. In addition, trials with incorrect descriptions of herbal prescriptions or unavailable statistical analysis were excluded. No language restrictions were imposed, and only publications with available abstracts were reviewed. The search process is further detailed in Figure 1.
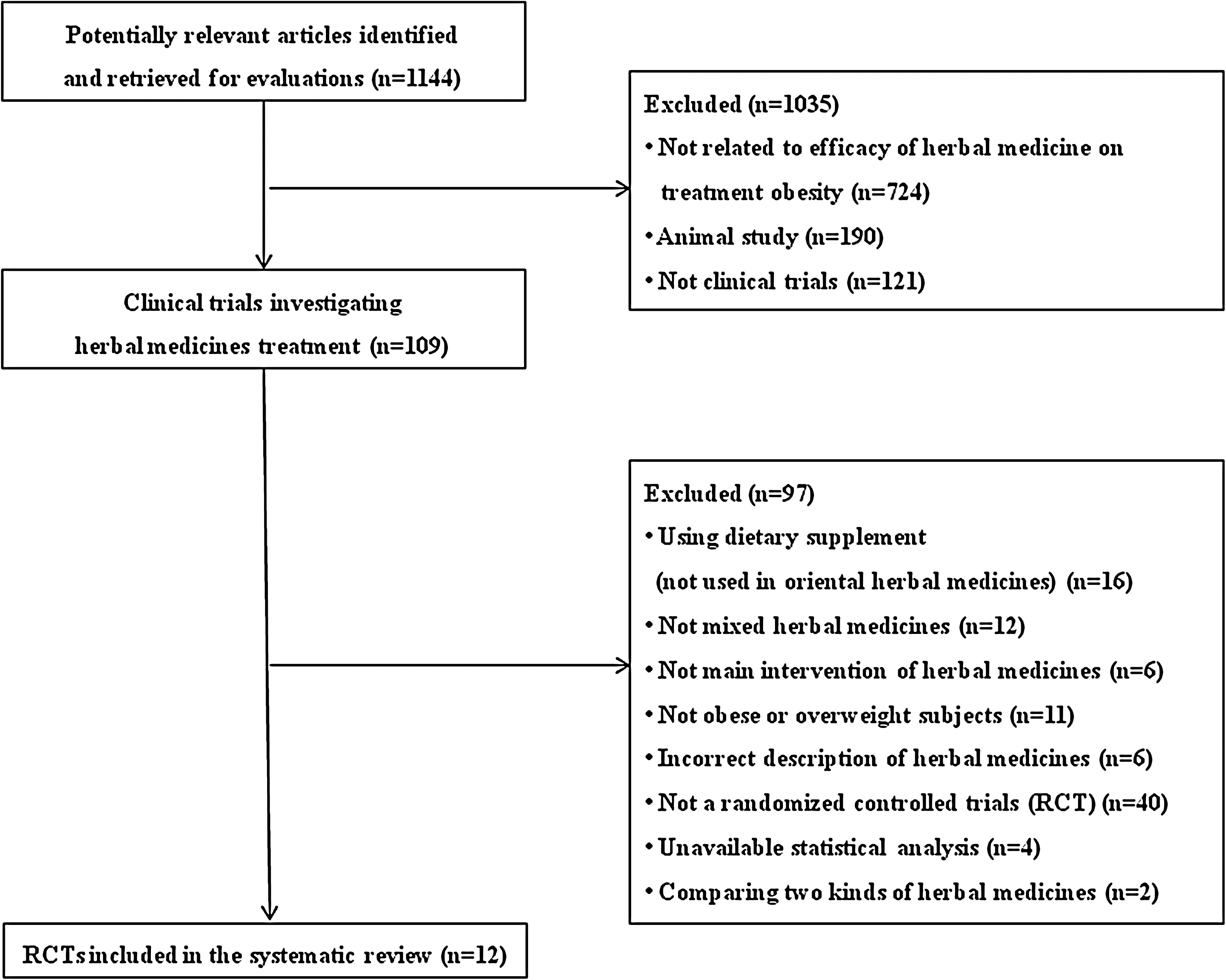
Flowchart of trials excluded versus selected for systematic review.
Results
Study description
An initial search identified 1144 potentially relevant articles, of which 12 met our inclusion criteria. Key data regarding the included RCTs are summarized in Table 1. All 12 RCTs were parallel two-arm design. Types of interventions considered in this review included herbal medicines, herbal medicines plus lifestyle control (such as dietary or exercise interventions), herbal medicines plus conventional medicines, and herbal medicines plus acupuncture treatment. The use of herbal medicines as the only intervention was used in six trials, and adjuvant interventions were used in six trials. Regarding types of control groups, a placebo procedure was used in five trials, conventional medicines were included in five trials, other treatments (e.g., acupuncture treatment) were used in one trial, and lifestyle control was used in one trial.
Showed positive effects similar to those observed in response to treatment with Western medicine.
Acu-Tx, acupuncture treatment; ASF, abdominal subcutaneous fat; AVF, abdominal visceral fat; BP, blood pressure; BMI, body mass index; CRP, C-reactive protein; DB, double-blind; FFA, free fat acid; HC, hip circumference; HOMA-IR, homeostasis model assessment of insulin resistance; IGT, impaired glucose tolerance; LDL-C, low density lipoprotein-cholesterol; NR, not reported; NS, not significant; PAI-1, plasminogen activator inhibitor-1; RMR, resting metabolic rate; t-PA, tissue plasminogen activator; TC, total cholesterol; TCM, traditional Chinese medicine; TG, triglycerides; WC, waist circumference; WHR, waist–hip ratio.
Study quality
Methodological quality was evaluated using the Jadad scoring system, and the highest possible score was 5 points. Trials with more than 3 points were considered to be of high quality. 23 The methodological quality of the trials was generally low. The average Jadad score was 1.5, and the range was from 1 to 4. Only two 12,14 of the 12 RCTs exhibited a Jadad score greater than 3. Only two trials 12,14 described the appropriate methods of randomization and double blinding. Sufficient details regarding dropouts and withdrawals were only given in two trials. 12,14 The average sample size was 74.8, and the range was from 24 to 156. We also considered whether a description of the ethical approval procedure was included and informed consent was obtained from the participants. Ethical approval procedures were mentioned in only two trials, 14,15 and informed consent was only obtained in five trials. 11,12,14,15,20
Outcomes
Herbal medicines versus placebo
All of the three trials 11 –13 in which the effects of herbal medicines for maintaining dietary habits or physical activity were compared with a placebo reported improved outcomes for obesity. The most rigorous trial 12 reported that the herbal medicine–only group showed significant improvement in indicators of obesity (body weight, body fat, BMI, etc.) when compared with a placebo group (P<.01).
Herbal medicines plus lifestyle control versus placebo plus lifestyle control
Two trials 14,15 compared the effectiveness of herbal medicines plus lifestyle controls such as dietary control or enhanced moderate exercise with the effects of placebo plus lifestyle control for obesity. One trial 14 reported that visceral fat area reduction was significantly greater in the herbal medicines plus lifestyle control group than in the placebo plus life style group (P<.01). In addition, the adjusted resting metabolic rate in the herbal medicines group was not decreased, whereas that in the placebo group showed a mild decrease. Body weight and body fat reduction in the herbal medicines group was greater after treatment (P<.01) compared with baseline than what occurred in the placebo group (P<.05). However, the differences between groups were not available in the article. The other trial 15 found no significant differences in body weight reduction or BMI between groups.
Herbal medicines versus conventional medicine
Three trials 16 –18 compared the effectiveness of herbal medicines with conventional medicines used as standard pharmacological treatments for obesity. One trial 18 reported significant body weight reductions for the herbal medicines group compared with the conventional medicine group (P<.01). The other two trials 16,17 reported that the herbal medicines group showed an improvement in obesity similar to that of the conventional medicine groups. Additionally, one trial 19 reported that the improvement in BMI and lipid metabolism was significantly greater in an herbal medicine plus conventional medicine group compared with a group that received conventional medicine alone (P<.01). Furthermore, one trial 20 showed an improvement in blood pressure, blood glucose, and lipid metabolism in a group that received herbal medicines plus conventional medicines and moderate exercise compared with a group that received conventional medicines plus moderate exercise (P<.01). However, there was no significant difference in terms of BMI between groups in that study.
Herbal medicines versus lifestyle control
One trial 21 compared herbal medicines with lifestyle controls such as diet and exercise and found that the group that received herbal medicines showed a significant reduction in body weight compared with the control group (P<.05).
Herbal medicines plus acupuncture treatment versus acupuncture treatment alone
One trial 22 reported that improvements in body weight and lipid profile were significantly greater in a group that received herbal medicines plus acupuncture and catgut embedment compared with a group that received acupuncture and embedment alone (P<.05).
Overall, the trials conducted to compare herbal medicines with other interventions revealed that there was greater improvement in BMI or body weight in groups that received herbal medicines than in the various control groups, except for two trials. 15,20 Although no significant reductions in BMI or body weight were observed in the trial by Wang et al., 20 the trial concluded that herbal medicines improved hypertension, blood glucose, and lipid metabolism.
Adverse events and safety
Six RCTs 12 –15,17,18 reported adverse events. Pan et al. 12 reported irritability and nausea in the treatment group; however, it did not appear to be related to the treatment. In addition, He et al. 13 reported vomiting in the treatment group, but the symptoms were not serious enough to discontinue the treatment. Hioki et al. 14 reported withdrawal due to the occurrence of loose stool, while improvement of constipation was also observed in the treatment group. Greenway et al. 15 also reported dose-related incidence of loose stools and other symptoms in the treatment group compared with the placebo group; therefore, they concluded that herbal medicines would not be an effective mode of treatment because of the possibility of causing gastrointestinal toxicity. Xie 17 reported diarrhea and abdominal discomfort in the treatment group, but dry mouth, loss of appetite, constipation, headache, and insomnia were observed in the control group. Wang 18 reported a significantly higher incidence of gastrointestinal problems and diarrhea in the treatment group than the control group (P<.01). Most of the reported adverse events appeared to be mild, except in the trial conducted to evaluate NT, 15 which caused adverse events that appeared to be related to the intervention, and in a trial conducted to evaluate Bofutsushosan, 14 which indicated that it caused loose bowel movements.
Five RCTs 12,14,15,18,20 assessed the effects of herbal medicine on the cardiovascular system and toxicity on renal and liver organs. However, significant changes were not observed after taking the herbal medicine. Despite this, Hioki et al. 14 reported improvements in blood pressure and urine analysis in the treatment group, and Wang et al. 20 reported improvement in blood pressure in the treatment group compared with the control group.
Discussion
To the best of our knowledge, this is the first systematic review of RCTs of mixed Oriental herbal medicines for the treatment of obesity. There was no restriction in terms of publication languages; therefore, the authors consider the present search strategy to have minimized bias. Recently, another similar systematic review that assessed the efficacy and safety of herbal medicines for obesity was published. The results of that study indicated that compounds containing Ephedra, Cissus quadrangularis, Ginseng, bitter melon, and Zingiber were found to be effective in the management of obesity. 24 That review included all human and animal studies conducted using all types of herbs and plant supplements, whereas our review was limited to RCTs that evaluated humans treated with mixed Oriental herbal medicines.
This systematic review provides evidence suggestive of the effectiveness of herbal medicines for treating obesity. Statistically significant reductions in BMI or body weight were reported in 83% of the included trials. However, the methodological limitations of the searched trials and the degree of evidence did not allow us to definitively conclude that herbal medicines improve obesity.
In this study, the standard Jadad scale was used to assess important criteria of methodological quality; however, many trials were of poor quality. Specifically, 83% of the trials (10 of 12 RCTs) scored 1 on the Jadad scale, and no RCTs achieved a full score of 5. In addition, most of the included trials lacked adequate allocation concealment. Such trials are likely to show exaggerated treatment effects. Additionally, only two 11,12 of the five trials evaluated in this study that used a placebo stated that they made the placebo drugs difficult to distinguish from the treatment medicine by adjusting the color or smell; therefore, it was difficult to assess the success of the blinding in the rest of the studies. Because each herb has its own color and smell, indistinguishable placebo medication should be made to ensure appropriate blinding.
Low-quality trials are more likely to overestimate the effects; 25 however, in our review, 80% of the low-quality RCTs generated positive results, whereas 100% of the high-quality trials generated positive results. Additionally, it is important to focus on both the methodological quality and the importance of ethical considerations in clinical trials. Ethical approval was reported in only two trials, 14,15 and informed consent was given in only five trials. 11,12,14,15,20 Considering the importance of protecting participants' rights, researchers should be aware of ethical issues.
Although six trials 16 –22 stated the rationale for the selection of herbal medicines, they did not address concrete diagnostic criteria, which might causes difficulties in diagnosis. Oriental medicine uses unique diagnostic tools that are based on the constitution or individuality of the patient rather than uniformity; therefore, clinicians should conduct trials based on clear diagnosis in future studies. However, standardization of diagnostic criteria for obesity has to be elucidated by further studies before this can be accomplished.
Small numbers of adverse events, primarily gastrointestinal irritation, were reported, and the vast majority of adverse events were mild or not related to the intervention. However, one trial 15 concluded that herbal medicines were not appropriate for treatment because of the possibility of adverse events such as diarrhea, even though the researchers used herbal medicines known to be effective in animal models without serious adverse events. This indicates that the results of clinical trials for humans might differ from those of animal studies; therefore, adverse events and safety should be checked through clinical trials conducted in human trials.
Five trials 12,14,15,18,20 assessed the safety of herbal medicines on the cardiovascular system and their toxicity on kidney and liver. The results of these trials found no significant changes after treatment with herbal medicines. However, in the other seven trials 11,13,16,17,19,21,22 there were no attempts to assess the safety of the compounds being tested; therefore, no definitive conclusion regarding safety could be made.
This study has some limitations. First, we attempted to identify all RCTs assessing the efficacy of mixed herbal Oriental medicines for the treatment of obesity, but the potential incompleteness of the citation tracking may have led to some relevant RCTs being overlooked. Additionally, many of the identified trials were of low quality and had methodological shortcomings such as there were no sample size estimations and an inadequate level of blinding, which may have influenced the results of our review. Moreover, most of the studies that have been conducted to date have been of short duration, varying from 4 to 24 weeks. Considering that obesity is a chronic condition, it is recommended that trials evaluate longer periods of treatment. Finally, because the occurrence of obesity may vary without treatments, a longer follow-up period with serial measurements of outcomes is suggested to determine the genuine effects of the herbal medicine being tested, as well as its long-term efficacy.
In conclusion, the present review provides suggestive evidence of the effectiveness of mixed herbal medicines in traditional Oriental medicines for treating obesity when compared with conventional medicines, placebos, or lifestyle control. Many trials have also reported an improvement in concomitant conditions such as impaired glucose tolerance, hypertension, lipid profiles, and inflammatory status. However, the results are of limited value because of the poor methodological quality of the included studies, which prevents us from drawing a definitive conclusion regarding the effectiveness of mixed herbal medicines. More research and well-designed clinical trials are necessary to address these issues and to assess the safety and adverse events associated with herbal medicines. Such trials should be randomized adequately, double-blinded, and controlled for placebo effects. In addition, future trials should adhere to rigorous trial designs that are suitable for the treatment of obesity based on Oriental medicine diagnosis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.