
Abstract
We evaluated the efficacy and safety of Ecklonia cava polyphenol (Seapolynol™, a polyphenol antioxidant and anti-inflammatory agent purified from E. cava) during a 12-week treatment period (400 mg orally once daily) in individuals with hypercholesterolemia and performed subgroup analysis for metabolic syndrome (MetS). As a noncomparative study, forty-six individuals (M:F=22:24, mean age=54±11 years) with fasting total cholesterol concentration >240 mg/dL or low-density lipoprotein cholesterol (LDL-C) concentration >130 mg/dL were enrolled. Hip circumference (100±7 cm vs. 98±7 cm, P<.01), total cholesterol (244±25 mg/dL vs. 225±37 mg/dL, P<.01), LDL-C (161±24 mg/dL vs. 146±34 mg/dL, P<.01), and C-reactive protein (2.51±3.55 mg/L vs. 1.37±1.32 mg/L, P<.05) were significantly decreased without significant adverse effect. A differential assessment according to the presence [MetS(+) group, n=18] and absence [MetS(−) group, n=28] of MetS showed that HbA1c decreased significantly following 12-week Seapolynol treatment in the MetS(+) compared with the MetS(−) group (−0.3%±0.5% vs. 0.1%±0.3%, P<.01). In conclusion, although our results showed that Seapolynol treatment is effective and safe without significant adverse events or abnormal laboratory findings during a 12-week period in individuals with hypercholesterolemia, more research in a larger population with a longer-term follow-up period in a randomized placebo-controlled study is needed to confirm the results.
Introduction
S
Brown algae have long been used traditionally as foodstuffs and folk medicines in Asian countries. Among the many brown algae, Ecklonia cava produces unique polyphenols called “eckols.” Although E. cava also produces other potentially medicinal polysaccharides and lipids, such as fucoidan, laminaran, fucoxanthin, and fucosterol, an increasing number of reports indicate that many of the medicinal properties of this brown alga derive from eckol and its derivatives. 9,10 Recently, eckols have been shown to have broad bioactivities, such as radical scavenging activity, 11 matrix metalloproteinase inhibitory activity, 12 protease inhibitory activity, 13 cytoprotective activity, 14,15 and anti-inflammatory activity, 16 in various in vitro and in vivo model studies. However, its cardiovascular and metabolic effects in humans remain poorly understood. Since Seapolynol™, a commercially available E. cava extract that was approved as a new dietary ingredient (NDI) by the U.S. Food and Drug Administration (FDA) in 2008 (FDA-1995-S-0039-0176), is a rich source of eckol derivatives, we have evaluated the efficacy and safety of a 12-week treatment with Seapolynol in individuals with hypercholesterolemia.
Materials and Methods
Test material
Tablets containing 200 mg of a polyphenol extract from the leaves of E. cava (Seapolynol) as the active ingredient were used for the study. Seapolynol was kindly supplied by Livechem, Inc. (Jeju, Korea) and was manufactured into 600 mg tablets using inactive ingredients, such as crystalline cellulose, lactose, silicone oxide, and magnesium stearate by a GMP manufacturer (Iljin Pharmaceutical, Hwasung, Korea). The total polyphenol content of Seapolynol as phloroglucinol equivalent was 98.5%. The notable compounds in Seapolynol identified by HPLC were dieckol (8.1%), 8,8′-bieckol (2.9%), 2-O-(2,4,6-trihydroxyphenyl)-6,6′-bieckol (2.2%), 6,6′-bieckol (1.6%), phlorofurofucoeckol A (1.5%), eckol (0.8%), 2-phloroeckol (0.5%), 7-phloroeckol (0.4%), and phlorotannin A (0.4%) [Waters, column: CAPCELL PAK ODScolumn (4.6 mm×250 mm); eluent: 30% aqueous MeOH; flow rate: 0.8 mL/min].
Subjects
Fifty-two Korean subjects were recruited from the patients who visited the outpatient cardiology clinics at Uijeongbu St. Mary's Hospital (The Catholic University, Uijeongbu, Korea) between July 2009 and December 2009. Basic information and medical screening data for inclusion in the trial were collected at recruitment. Inclusion criteria were as follows: (1) between 18 and 80 years of age; (2) fasting triglyceride concentration <400 mg/dL; and (3) fasting total cholesterol concentration >240 mg/dL or fasting LDL-C concentration >130 mg/dL. Exclusion criteria were as follows: (1) current use of cholesterol-lowering medications (HMG-CoA reductase inhibitors or fibrates) or nonsteroidal anti-inflammatory drugs; (2) a history of significant cardiovascular disease (myocardial infarction, unstable angina pectoris, heart failure, or serious arrhythmia) within the last 3 months; (3) a history of stroke within the last 3 months; (4) a presence of other underlying diseases, such as chronic renal disease, chronic liver disease, and malignancies; (5) use of drugs that might interact with the treatment protocol, such as diltiazem HCl, digoxin, cimetidine, rifampicin, erythromycin, ketoconazole, itraconazole, nitrate, cyclosporine, and grapefruit juice; (6) having aspartate aminotransferase (ALAT) or alanine aminotransferase (ASAT) level >3 times upper normal limit; (7) with hemoglobin level <10 g/dL, neutrophil count <1500/mm3, platelet count <100,000/mm3, or creatinine level >2.0 mg/dL. Pregnant and lactating women were excluded, as were those seeking to become pregnant.
Subjects who were participating in other clinical trials or who were legally or mentally considered unsuitable for participation in clinical trials were excluded. All participants gave written informed consents to participate in the study. The protocol was approved by the institutional review at the Catholic University of Korea (Uijeongbu, Korea) and conducted in agreement with the Declaration of Helsinki, and performed in accordance with the International Conference on Harmonization (ICH) guidelines.
Experimental methods
This was a single-center trial consisting of a 2-week run-in period and a 12-week treatment period. All subjects were orally administrated two tablets (200 mg of Seapolynol/tablet) daily for 12 weeks. The time of ingestion of the test tablet was not limited, but it was recommended that the subjects ingest the test capsule between meals to maintain compliance. The subjects were instructed to maintain their usual dietary intake and physical activity, but supplemental food products or medications known to influence lipid or carbohydrate metabolism were prohibited. Anthropometric parameters were measured at baseline, week 4, and week 12. Fasting blood sampling for biochemical and hematologic parameters was performed at baseline and at week 12. Physical conditions and potential adverse effects were assessed by a physician during each visit. The study design is shown in Figure 1.
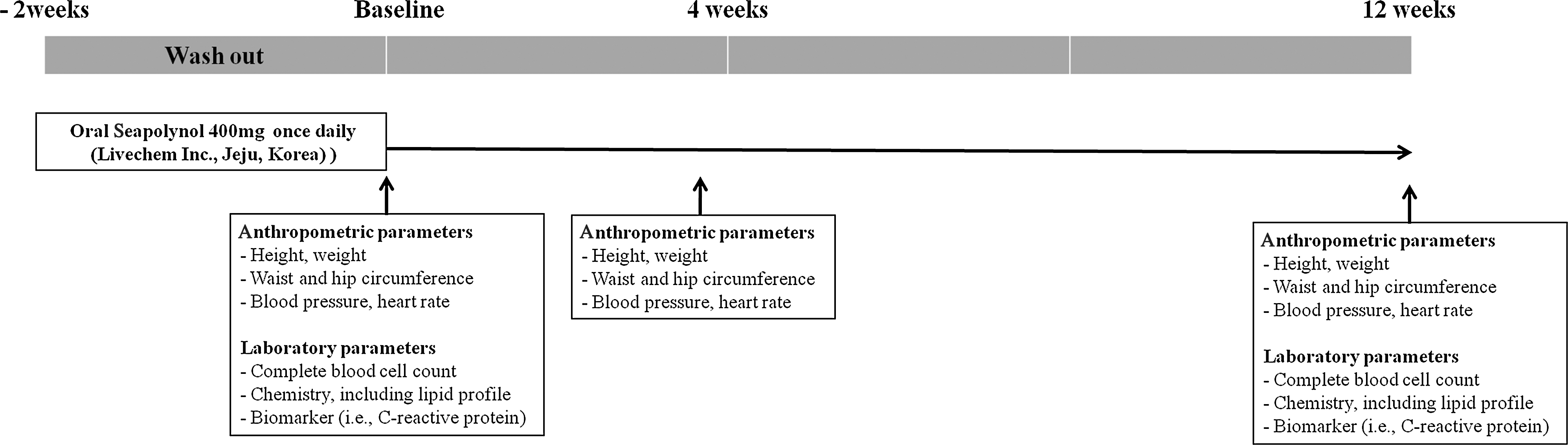
Study design.
Anthropometric parameter measurement
The heights were measured to the nearest 0.1 cm with a portable stadiometer (InBody 720; Biospace Ltd., Seoul, Korea) at baseline. Body weights were measured to the nearest 0.1 kg using a digital scale wearing a standard hospital gown. Body mass index (BMI) was calculated as the weight in kilograms, divided by the height in meters squared. Waist and hip circumferences were measured using a standardized tape by the same well-trained staff. The tape was calibrated before use. The waist circumference was measured 1 inch above the umbilicus in the standing position. The hip circumference was measured at the site of the largest circumference between the waist and thighs. Systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure, pulse pressure, and heart rate were measured using an automatic blood pressure monitor with subjects in a seated position after resting quietly for 10 min.
Biochemical and hematologic parameter analysis
Blood samples were taken at baseline and week 12. A fasted blood sample of 10 mL was taken and mixed with ethylenediaminetetraacetic acid to prevent clotting. Plasma was obtained by centrifugation, frozen in liquid nitrogen, and stored at −80°C until further analysis.
The serum total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C), and triglyceride levels were measured using an automatic analyzer (7600-110; Hitachi Ltd., Tokyo, Japan). The serum glucose levels were measured by the hexokinase method using the same instrument. The complete blood count, such as white blood cells, hemoglobin, hematocrit, and platelet, was measured by a hematology analyzer (Sysmex XE-2100; Sysmex Corporation, Kobe, Japan). HbA1c was measured by G7 HbA1c analyzer (Tosoh Corporation, Tokyo, Japan). The biochemistry, including ALAT, ASAT, gamma-glutamyl transpeptidase, total bilirubin, direct bilirubin, albumin, blood urea nitrogen, creatinine, serum sodium, serum potassium, lactic dehydrogenase, creatine kinase, uric acid, alkaline phosphatase, apolipoprotein B, apolipoprotein A1, glucose, and C-reactive protein from blood samples, was measured by a biochemistry analyzer (7600-110; Hitachi Ltd., Tokyo, Japan).
Differential evaluation of 12-week intervention effect with Seapolynol according to the presence of metabolic syndrome
After the 12-week intervention period, differential evaluation of the effects of Seapolynol compared subjects with metabolic syndrome (MetS) to those without MetS.
For this purpose, eligible participants who completed the study were divided into metabolic syndrome negative [MetS(−)] and positive [MetS(+)] groups according to the criteria by the National Cholesterol Education Program in Adult Treatment Panel III (NCEP-ATP III), 17 and were comparatively evaluated for changes in anthropometric and biochemical parameters. The participants who had at least three of the following five metabolic risk factors were placed in the MetS(+) group and otherwise placed in the MetS(−) group: (1) waist circumference ≥90 cm for men and ≥80 cm for women (according to the modified definition of central obesity for Asians) 18 ; (2) triglyceride level ≥150 mg/dL; (3) HDL-C level <40 mg/dL for men and <50 mg/dL for women; (4) SBP ≥130 or DBP ≥85 mm Hg; (5) fasting blood glucose ≥110 mg/dL.
Statistical analysis
The values of all test parameters are presented as mean±standard deviation. Differences between measurements performed at baseline and week 12 were assessed using parametric (Student's t-test for paired observations) or nonparametric (Wilcoxon signed rank test) test as appropriate. Multivariate logistic regression was performed to identify independent risk factors for the presence of MetS using components of MetS. 17,18 P<.05 was considered to be statistically significant. Statistical analyses were performed using SAS for Windows version 9.1 (SAS Institute, Cary, NC).
Results
Of the 52 eligible subjects initially selected for the study, 3 subjects dropped out of the study due to the failure of follow-up visits, and 3 others were also excluded due to noncompliance and subsequent switching to other medications (HMG-CoA reductase inhibitors). Finally, 46 patients completed the study according to the protocol. Their mean age was 54±11 years, and the prevalence of hypertension, diabetes mellitus, and current smoking status was 23.4%, 8.7%, and 4.3%, respectively.
Effect on anthropometric parameters
Effects of 4- and 12-week intervention with Seapolynol on anthropometric parameters are summarized (Table 1). After 12 weeks, hip circumference (−2.0%, P<.01) significantly decreased. Other anthropometric parameters, such as BMI, weight, waist/hip ratio, waist circumference, blood pressure, mean arterial pressure, pulse pressure, and heart rate, did not change throughout the intervention period.
Data values are mean±SD of 46 patients. P-values were analyzed using Wilcoxon signed rank test.
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
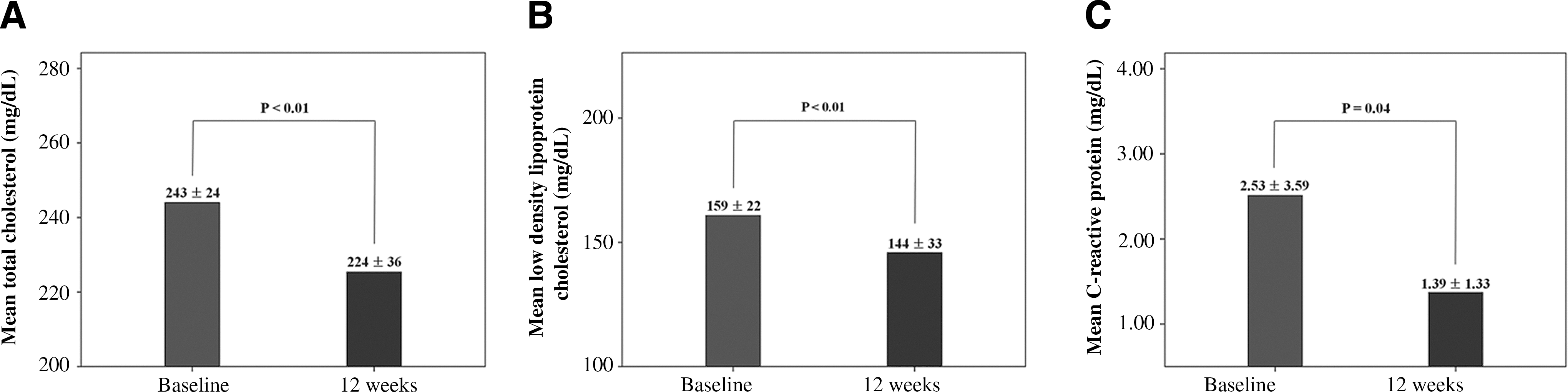
Effect on lipid profile and C-reactive protein
The blood lipid parameters and C-reactive protein of the subjects at baseline and after 12-week intervention with Seapolynol are summarized (Table 1). The level of total cholesterol (−7.8%, P<.01) and LDL-C (−9.4%, P<.01) decreased significantly. The changes in triglyceride (−5.5%, P=.25) and HDL-C (+4.1%, P=.11) concentrations after 12 weeks were not statistically significant. C-reactive protein, and indicator of inflammatory status, was significantly decreased after 12 weeks (−45.1%, P<.05) (Figure 2).
Changes in levels of
Differential assessment according to the presence of MetS
To assess the differential response to Seapolynol according to the presence of MetS, the entire group (n=46) was divided into two categories, that is, MetS(−) group (n=28) and MetS(+) group (n=18), according to the criteria set by the NCEP-ATP III and the modified definition of central obesity for Asians. 17,18 The baseline difference between MetS(−) and MetS(+) groups was shown in BMI (P<.01), waist circumference (P<.01), hip circumference (P<.01), waist–hip ratio (P<.05), SBP (P<.05), DBP (P<.05), fasting blood sugar (P<.05), HbA1C (P<.05), triglyceride (P<.01), HDL-C, and apolipoprotein B (P<.01). During the 12-week Seapolynol treatment period, the magnitude of decrease in the level of HbA1c (ΔHbA1c) was significantly greater in the MetS(+) group than in the MetS(−) group (−0.3% to −0.5% vs. −0.1% to −0.3%, P<.01) (Table 2 and Fig. 3).
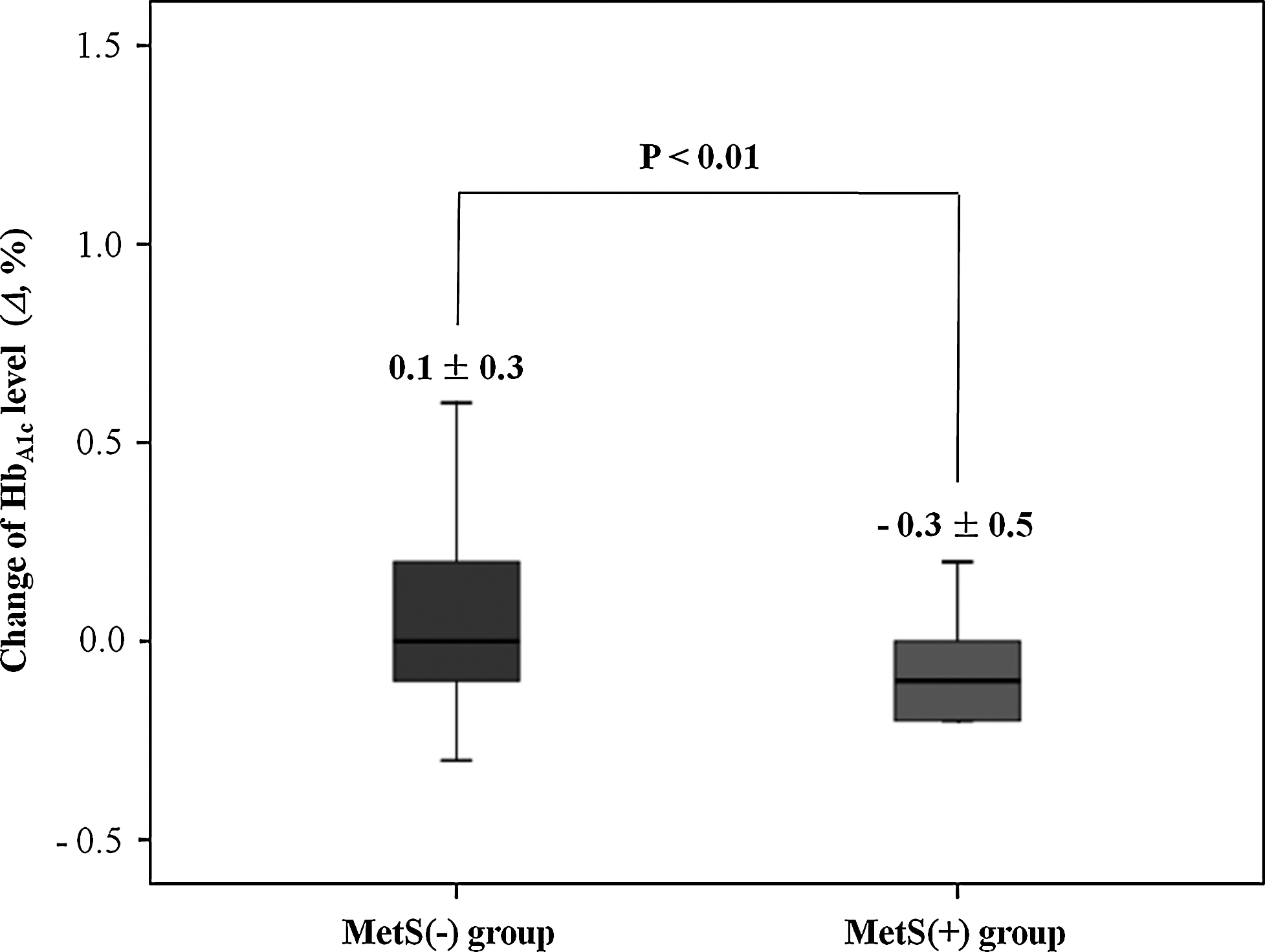
Change in HbA1c level during the 12-week Seapolynol treatment period according to the presence of metabolic syndrome.
P-values were analyzed using Student's t-test for paired observations.
MetS, metabolic syndrome; MetS(−), MetS-negative group (n=28); MetS(+), MetS-positive group (n=18); Δ, change during 12-week Seapolynol intervention.
Safety assessment
Liver and kidney biochemical markers, including levels of ALAT, ASAT, creatine kinase, and lactic dehydrogenase, all remained within the normal range during the study (Table 1). Observations of side effects were performed by assessment of nausea, vomiting, dyspepsia, abdominal pain, constipation, diarrhea, and alopecia during the study. There was one case (2.2%) each of nausea, dyspepsia, diarrhea, and alopecia (Table 3). However, there were no significant adverse events or abnormal laboratory findings.
Evaluated for the whole group (n=46).
Discussion
This is the first study to evaluate the cardiovascular effects of a polyphenolic extract from E. cava (Seapolynol) on hypercholesterolemic patients.
During the 12-week Seapolynol treatment period, there was significant decreases in both LDL-C and C-reactive protein levels, a serum inflammatory marker, which demonstrates that Seapolynol, as is the case with statins, improves lipid profile and reduces vascular inflammation, which plays a key role in the initiation, development, and progression of early atherosclerosis. This indicates that Seapolynol has the potential to improve cardiovascular risk profile in humans. In a recent cholesterol-fed rat hyperlipidemic model study, treatment with polyphenol-rich extracts of Ecklonia stolonifera and isolated polyphenols, eckol and dieckol, significantly improved lipid profiles, suggesting their clinical potential for prevention of hyperlipidemic atherosclerosis. 19 E. stolonifera and E. cava are closely related brown algae species known to produce the same type of compounds, including eckol, dieckol, 6,6′-bieckol, 8,8′-bioeckol, and phlorofurofucoeckol, as major polyphenolic components. 20
Although it is not clear, several reports suggest that the anti-dyslipidemic mechanism of E. cava polyphenols may include radical scavenging activity, matrix metalloproteinase inhibitory activity, protease inhibitory activity, and anti-inflammatory activity. 11 –16 However, it is necessary that this uncontrolled study followed up with controlled trials to exclude the possibility of time-related bias (i.e., consequence of these lifestyle changes).
Obesity, as a parameter of MetS, is a serious public health problem that predisposes affected individuals to a variety of pathological disorders, such as hyperglycemia, hypertension, and cardiovascular diseases. 21 –23 Based on the recent report, 24 7-phloroeckol, a polyphenolic compound isolated from E. cava and present as one of the major components in Seapolynol, inhibited lipid accumulation and adipocyte differentiation with downregulation of the genes involved in lipogenesis and adipogenesis. Further, Shin et al. 25 reported that Seapolynol decreased body fat by suppressing adipogenesis and lipogenesis in a double-blind randomized study in overweight Korean individuals. Similarly, our results showed that Seapolynol contributes to decreased hip circumference among the anthropometric parameters. Further studies involving in vivo models are needed to explain this effect in greater detail.
In the present report, ΔHbA1c significantly decreased in the MetS(+) group relative to MetS(−) group during the 12-week Seapolynol treatment period. In a murine noninsulin-dependent diabetes model, Iwai 26 showed that polyphenol-rich extracts of E. stolonifera have strong antidiabetic and antioxidant effects. Further, the extract was also shown to suppress the progression of insulin resistance and lipid peroxidation in plasma of mice during the intervention. In an in vitro study, the same extract inhibited α-glucosidase (IC50=22 μg/mL), and another in vitro study of three components (7-phloroeckol, eckol, and dieckol) present in Seapolynol demonstrated their anti-glycation effect. 27 Therefore, the present study together with those in in vitro and animal model studies supports the possibility of using Seapolynol as an antidiabetic pharmaceutical or functional food. However, further studies are needed to better elucidate the mechanism of Seapolynol treatment in subjects with MetS.
There are several limitations in our present study. First, this study was performed without comparison with placebo or statin group. Further analysis of Seapolynol treatment under a double-blinded, placebo (or statin)–controlled randomized protocol is warranted. Second, the study population was too small to assess an achievement of therapeutic target levels of total cholesterol and LDL-C, and the intervention period (12 weeks) was too short to adequately evaluate potential side effects. Therefore, further investigations employing larger population in multicenter trials together with longer-term follow-up studies are required.
In summary, Seapolynol treatment showed beneficial effect on blood lipid parameters, such as total cholesterol and LDL-C levels, as well as anthropometric parameters, such as hip circumference, and on the blood inflammatory marker C-reactive protein in hypercholesterolemic patients without significant adverse effect during a 12-week period. Additionally, in a post hoc differential analysis of the same patients according to the presence of MetS, HbA1c level significantly decreased in the MetS(+) group relative to the MetS(−) group. In conclusion, although our results in this study showed that Seapolynol treatment is effective and safe without significant adverse events or abnormal laboratory findings during a 12-week period in individuals with hypercholesterolemia, more research including a larger population, longer-term follow-up period, and a randomized controlled protocol should be considered.
Footnotes
Acknowledgment
The authors thank the men and women who participated in this investigation.
Author Disclosure Statement
No competing financial interests exist.