
Abstract
Nursing home residents have severe vitamin D deficiency and increased risk of falls and fractures. These individuals may need 125 μg of vitamin D3 to achieve desirable 25-hydroxyvitamin D [25(OH)D] concentrations to improve overall health. We evaluated health-related quality of life (HRQoL) in 45 nursing home residents (28 women and 17 men, aged 58–89 years) with 25(OH)D concentrations <50 nM who consumed daily one bun that had been fortified with 125 μg vitamin D3. The Romanian version of Questionnaire of the European Foundation for Osteoporosis (QUALEFFO-41) was applied at baseline and after 12 months. Data were analyzed using repeated measures analyses of variance (ANOVA). After one year supplementation, serum 25(OH)D reached optimal status (>75 nM) and bone health has improved significantly. Nursing home residents who consumed daily bread fortified with 125 μg vitamin D3 reported significant (P=.02 for the effect of time) improvement in HRQoL (total score of QUALEFFO-41). The interaction time x treatment was also statistically significant on pain (P=.04), daily activities (P=.02), and locomotion (P=.04). To ensure the serum concentrations of 25(OH)D recommended by medical groups for bone- and general-health in the older nursing residents, the practical experience shows that much higher amounts of vitamin D3 are required. Fortification of bread and cereals is a feasible way to improve vitamin D nutrition.
Introduction
V
Achievement of adequate vitamin D status is crucial for bone health. Serum 25(OH)D concentrations ≤30 nM (12 ng/mL) were associated with sarcopenia 4 and an increased fracture risk in persons aged 65–75 years. 3 In seniors, treatment with vitamin D should lead to the recommended blood concentration; ideally, the target range for serum 25(OH)D should be >30 ng/mL (75 nM), 5 which may need 125 μg (5000 IU) vitamin D3 supplementation in individuals with severe vitamin D deficiency. 6,7,8
A substantial percentage of nursing home residents show an inadequate vitamin D status, but poor adherence appears to be a major factor limiting the efficacy of vitamin D and calcium supplementation in clinical practice. This could be remedied by the consumption of vitamin D-fortified foods and/or vitamin D supplements. 9 Bread is very widely consumed in nursing homes, and may serve as an ideal vehicle for fortification. 7,10 Vitamin D3 is stable in bread, and is effective in raising serum 25(OH)D concentrations in adults. 6,11 –13
We previously reported on a single-arm clinical trial in nursing home residents (NCT00789503) the efficiency and safety of daily consumption of bread fortified with 125 μg (5000 IU) of vitamin D3 to raise serum 25(OH)D of at least 75 nmol/L in virtually all the adults. 7 Here, we report the effects on quality of life when bread fortified with vitamin D and calcium is given for one year to nursing home patients with or without osteoporotic vertebral fracture. To our knowledge, this is the first study to evaluate the long-term effects of daily consumption of 125 μg (5000 IU) of vitamin D3 as fortified bread on quality of life in older adults living in nursing home.
Materials and Methods
Participants
We prospectively evaluated the effects of vitamin D supplementation on quality of life in 45 patients (28 women and 17 men) aged 58–89 years living in a nursing home for older people in Iasi, Romania, between November 2003 and December 2004. Exclusion criteria were malignant disease; renal, hepatic, or gastrointestinal disorders, endocrine disease associated with abnormal calcium metabolism that required therapy; alcohol consumption of four or more drinks per day; or treatment with estrogen, progesterone, glucocorticoids, anticonvulsivants, vitamin D supplements, or other medications known to affect calcium or bone metabolism during the previous 12 months. At the beginning, bone mineral density (BMD) was measured and vertebral fractures were identified by X-rays of the thoracic and lumbar spine. Patients were divided into two groups: with vertebral fractures (VF) and without vertebral fractures (VFX).
Study protocol
The study was a longitudinal prospective study approved by the University's Human Ethics Committee according to the declaration of Helsinki. After agreeing to participate and giving informed consent, fasting blood and urine samples were collected at baseline and after 12 months. Urine was collected for 24 hours to measure calcium and creatinine. Calcium and intact parathyroid hormone were measured in serum. At the beginning and at the end of the study, bone mineral density (BMD) was measured by dual-energy X-ray absorptiometry and vertebral fractures were identified by X-rays of the thoracic and lumbar spine. All patients received one bread bun (100 g) daily, fortified with 800 mg calcium carbonate (320 mg elemental calcium) and 125 μg (5000 IU) vitamin D3 for one year. Adherence to the study protocol was assessed by questionnaire 14 at the end of the study, and by measurement of the plasma 25(OH)D concentration.
Questionnaires
Monitoring changes in quality of life was done through Romanian validated versions of EuroQoL EQ-5D (EQ-5D; a weighted index of health and EuroQoL health status thermometer) 15 and Questionnaire of the European Foundation for Osteoporosis (QUALEFFO-41). 16 Patients completed the EQ-5D and QUALEFO-41 questionnaires before starting vitamin D supplementation and after 6 months and 12 months of supplementation. Participants completed the questionnaires during an interview with the principal investigator (A.R.C.).
The EuroQoL EQ-5D is a self-administered, two-part questionnaire on health-related quality of life. The first part of EQ-5D includes single item measures of five health dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Responses were recorded as a 5-digit code, which was then converted to a score from −0.59 to 1. In addition, the second part of EQ-5D includes a global rating of current health using a visual analog scale (EuroQoL Health Thermometer) ranging from 0 (worst imaginable) to 100 (best imaginable).
QUALEFFO-41 consists of 41 questions in five domains: pain, physical function, social function, general health perception, and mental function. Domain scores and total score were calculated by averaging all answers and transforming them to a 0–100 scale (0 represents best health).
The outcome for each item was categorized as follows: Improvement: • EQ-5D questionnaire: Having the final score 10% higher (better) than baseline. • QUALEFFO-41: Having the final score 10% lower (better) than baseline Deterioration: • EQ-5D questionnaire: Having the final score 10% lower (worse) than baseline. • QUALEFFO-41: Having the final score 10% higher (worse) than baseline. Stable: • Stable was defined for symptoms assessed by the EQ-5D questionnaire as well as by the QUALEFFO-41 as having met neither the criteria for improvement nor for deterioration at the end of the supplementation period.
Fortification of food
Each day, all subjects received one bread bun fortified with 800 mg calcium carbonate (320 mg of elemental calcium) and 125 μg (5000 IU) vitamin D3/day. The vitamin D3 in samples of the bread was measured by solvent extraction followed by high-performance liquid chromatography and ultraviolet detection. Mean value of vitamin D3 in bread was 5062.2+459.7 IU/bun. 7
Analytical methods
Serum and urinary calcium were measured by using standard laboratory methods. Serum 25(OH)D was measured by immunoassay (Liaison Analyzer, DiaSorin, Stillwater, Minnesota, USA). Serum intact parathyroid hormone (PTH) was measured by an enzyme-amplified ‘‘2-step’’ sandwich-type immunoassay (DSL, Webster, Texas, USA). The BMD of the lumbar spine, femoral neck, and trochanter were measured by dual-energy X-ray absorptiometry (Delfi A, Hologic, Waltham, Massachusetts, USA).
Statistical Analysis
Statistical analysis was performed with SPSS v. 13.0 for Windows (SPSS Inc., Chicago, Illinois, USA). Values are expressed as mean±standard deviation or as percentages. Baseline values for the VFX and VF groups were compared using an independent samples t-test or Pearson's chi-square test, as appropriate. Data were analyzed by repeated-measures analyses of variance (ANOVA) using the general linear model. To investigate how the effect of vitamin D on wellbeing would differ by baseline presence of vertebral fractures, the main effect of interaction time×vertebral fracture was assessed; an interaction between sex and vertebral fractures was added to the model above. Pearson coefficient was used for determining the significance of the relationship between quality of life and vitamin D status. Statistical significance was based on P<.05.
Results
Of the 45 patients enrolled, 40 completed the study (1 left for personal reasons, 1 left the nursing home, and the other 3 died). Table 1 shows the population characteristics (n=40). There were no significant differences in age, BMI, calcemia, PTH, lumbar and hip BMD, or percentage of patients who suffer osteoporosis between VFX (14 women and 6 men) and VF (13 women and 7 men) groups.
Data expressed as mean±standard deviation.
P-value for comparison between groups by Student's t test for continuous variables and Pearson's chi-square for categorical variables.
VFX, no fractures (n=20); VF, fractures (n=20); 25(OH)D3, 25-hydroxyvitamin D; BMI, body mass index; PTH, parathyroid hormone; BMD, bone mineral density.
Table 2 displays the changes in calcium, vitamin D, and bone parameters after 12 months of vitamin D bread intervention in VFX and VF groups. Basal serum concentrations of 25(OH)D were very low in both groups (28.1±9.4 nM in VFX group vs. 28.9±12 nM in VF group, P=.82). Vitamin D deficiency [25(OH)D<30 nM] was found in 56% of patients in VFX group (14 of 25) and in 53% of patients in VF group (9 of 17). The one-year supplementation with bread fortified with 125 μg (5000 IU) vitamin D3 IU/day increased serum 25(OH)D concentrations more than 75 nmol/L (123.5±38.1 nM in VFX group vs. 128.5±41.1 nM in VF group). Repeated measures ANOVA analysis showed a significant effect of time (interaction time×treatment) on serum 25(OH)D (P<.001), serum PTH (P<.001), lumbar T-score (P=.03), hip BMD (P<.001), and hip T-score (P<.001) at 12 months of vitamin D3 and calcium supplementation. The interaction effect between time and vertebral fracture was statistically significant (P<.05) on lumbar BMD and hip T-score.
Data expressed as mean±standard deviation. P-values determined by repeated-measures ANOVA. The interaction effect between sex and vertebral fracture was statistically significant (P<.05) on serum 25(OH)D.
P-value assesses the effect of vitamin D bread on variables.
P-value assesses the main effect of vertebral fracture on variables.
Vitamin D sufficiency level.
25(OH)D, 25-hydroxyvitamin D.
Table 3 shows the changes on EQ-5D or QUALEFFO-41 outcomes from baseline to 12 months. The consumption of bread fortified with 125 μg vitamin D3 during 12 months improved in several subscales of QUALEFFO-41 score. Based on the results of ANOVA, the total score for QUALEFFO-41 improved significantly (for the interaction between time and treatment, f=5.43, P=.02, partial η2=0.131). The interaction time×treatment was also statistically significant on pain (f=4.57, P=.04, partial η2=0.105), daily activities (f=5.91, P=.02, partial η2=0.138), and locomotion (f=4.40, P=.04, partial η2=0.115). The main effect of vertebral fracture was statistically significant on domestic jobs (f=7.36, P=.01, partial η2=0.178) and locomotion (f=4.86, P=.03, partial η2=0.122). The main effect of sex was statistically significant on domestic jobs (f=3.48, P=.05, partial η2=0.93). The interaction effect between sex and vertebral fracture was statistically significant (P<.05) on total score, daily activities, domestic jobs, and locomotion (additional data, not shown in Table 3).
Data expressed as mean±standard deviation. P-values determined by repeated-measures ANOVA. The interaction effect between sex and vertebral fracture was statistically significant (P<.05) on total score, daily activities, domestic jobs, and locomotion.
P-value assesses the effect of vitamin D bread on variables.
P-value assesses the main effect of vertebral fracture on variables.
A score of 1 represents best health.
A score of 0 represents best health.
EQ-5D, EuroQoL EQ-5D, a weighted index of health; QUALEFFO-41, Questionnaire of the European Foundation for Osteoporosis.
Table 4 displays the outcome of nursing home residents measured with EQ-5D or QUALEFFO-41 recorded as improvement, stable, or deterioration. After the supplementation period, EQ-5D questionnaire indicated an improvement in 41% of patients in VF group and 48% of patients in VFX group. EuroQoL Health Thermometer, which marks the individual's perception of their health, showed an improvement in 24% of patients in VF group and in 28% of patients in VFX group. QUALEFFO-41 test indicated an improvement in 22% of patients in VF group and in 8% of patients in VFX group. Among domains of the QUALEFFO-41 questionnaire, the most important improvement was recorded for pain (in 50% of patients with fracture and 28% of patients without fracture) at the end of the study. There were no significant differencs between groups based on chi-squared test.
P-value for comparison between groups determined by Pearson's chi-squared.
The results from the correlational analyses demonstrated a significant correlation at baseline and after vitamin D bread protocol between the total score of QUALEFFO-41 and scores of EQ-5D (r=−0.75, P<.001 vs. r=−0.62, P<.001) and EuroQoL Health Thermometer questionnaires (r=−0.54, P<.001 vs. r=−0.40, P=.02).
At baseline, a significant correlation was found between scores of the EQ-5D questionnaire and EuroQoL Health Thermometer and plasma concentrations of 25(OH)D (r=0.36, P<.05 and r=0.34, P<.05, respectively). The Pearson's analyses demonstrated a significant negative correlation between the total QUALEFFO-41 score and plasma concentrations of 25(OH)D at baseline (r=−0.49, P<.01; Fig. 1A) and at the end of supplementation with vitamin D3 (r=−0.59, P<.001; Fig. 1B).
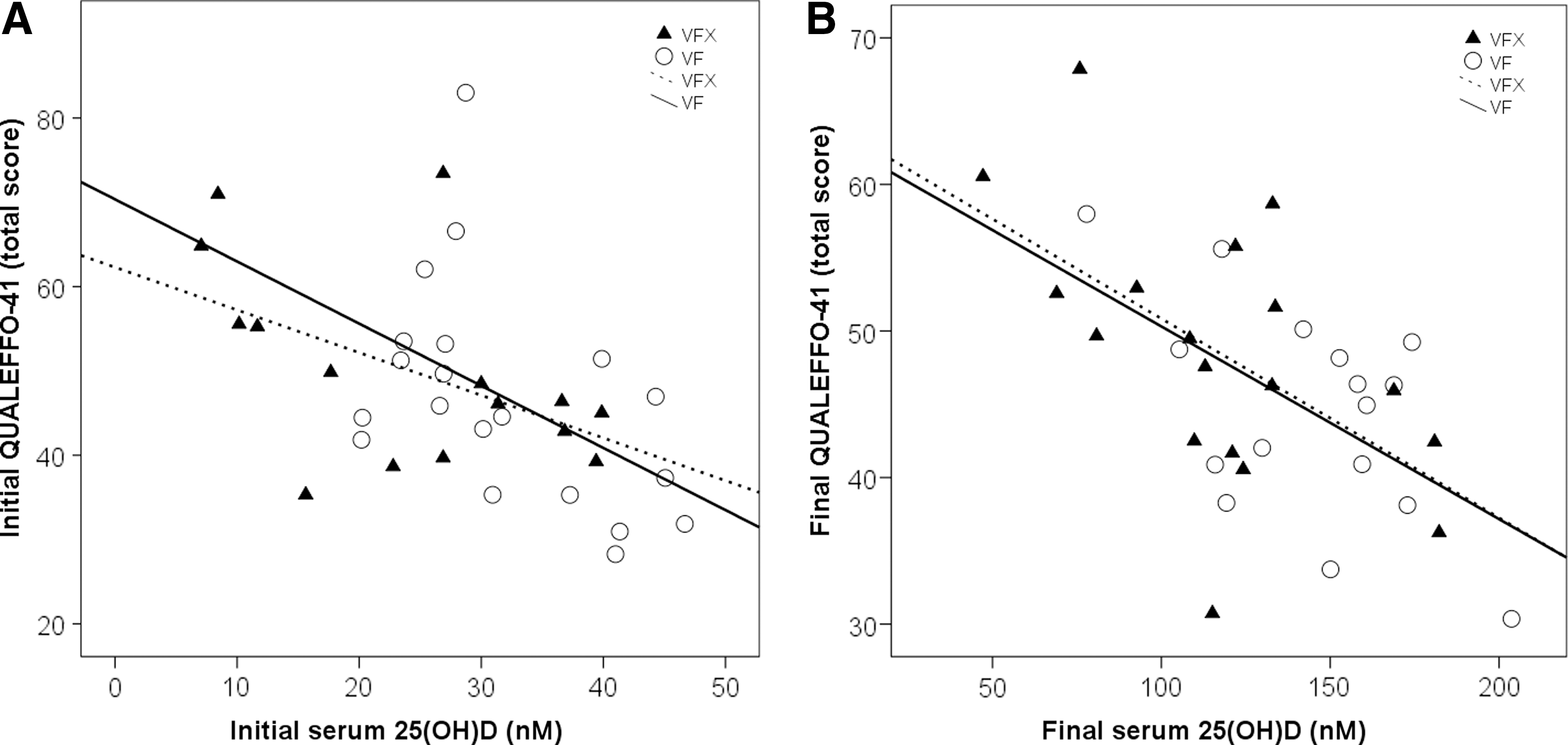
Negative association between serum concentrations of 25(OH)D and total score on the QUALLEFO-41 measured
Discussion
Vitamin D deficiency in older people has been associated with osteomalacia and high risk of falls and fracture. Vertebral fracture, especially, could be associated with significant morbidity in terms of physical and psychosocial functioning, and reduce health related quality of life. Consequently, the improvement of the quality of life becomes a domain of great interest.
Treatment with vitamin D should lead to optimal 25(OH)D blood concentrations to prevent fracture. Bischoff-Ferrari and Dawson-Hughes 5 concluded that, in order to prevent fractures, serum 25(OH)D concentration should exceed 75 nM. Some data suggest that for most older people (who are likely to have baseline 25(OH)D concentrations of <50 nM), a dose between 50 and 125 μg (2000–5000 IU) per day of oral vitamin D3 is sufficient to raise 25(OH)D concentrations to >75 nM. 17 For these reasons, we focused on evaluating the impact on the quality of life of the normalization of vitamin D concentrations in the older nursing home residents with or without vertebral fractures, using as a vehicle bread fortified with 125 μg vitamin D3 (5000 IU).
In a previous study 7 we reported that the consumption of bread fortified with 125 μg vitamin D3 during 12 months led to achieve and maintain the optimal concentrations (>75 nM). The adherence to fortified bread intake was monitored by questionnaire. The rate of compliance was as follows: 91% of patients reported that they consumed the fortified bread every day and 76% of patients consumed the whole bun. 7
In this study, we reported a significant effect of interaction treatment×time on total score (P=.02) for QUALEFFO-41 questionnaire during the interaction period. Also, we found significant correlations between serum concentrations of 25(OH)D and total score of QUALEFFO-41 questionnaire before and after vitamin D supplementation. The consumption of vitamin D bread for one year led to an improvement of HRQoL. Using the qualitative evaluation (improvement, stable, or deterioration), more than 40% of the patients in both groups showed an improvement of HRQoL measured by EQ-5D test at the end of supplementation period. Some studies conducted on the association between optimal status of vitamin D and wellbeing showed conflicting results even when high doses of vitamin D were administrated. Vieth et al., reported that the 100 mg (4000 IU)/day dose of vitamin D3 resulted in statistically significant improvement in well-being of adult patients. 18 Another study reported that annual dose of 500,000 IU vitamin D3 failed to improve the well-being outcomes in women aged 70 years or older. 19
We also reported a significant effect of interaction treatment×time on pain (P=.04). The effect of vitamin D bread consumption on pain (diminished perception in 50% of patients with fracture and in 28% of patients without fracture) could be related to amelioration in osteomalacia and fracture risk reduction. There is a well-established link between low vitamin D and pain. 20,21 The nursing home residents participating to this study showed a significant increase in hip BMD, lumbar, and hip T-score after 12 months of supplementation with high dose of vitamin D and calcium. 7 However, the main effect of vertebral fracture on pain was not significant in our study. This could suggest that vitamin D effect to diminish chronic pain experienced by the older adults could be explained not only by the well-established role of vitamin D in bone health, but other mechanisms could be also involved. The vitamin D receptors have been identified in skeletal muscle. Myopathy presenting as a gradual but continuous decrease in muscle strength, usually in lower limbs, is also part of the osteomalacic symptom complex and may appear before any pain. 22
In nursing home residents there was a significant interaction time×treatment observed on the physical functions scores of QUALEFFO-41: daily activities (P=.02) and locomotor functions (P=.04). The reduction of pain probably contributed to greater improvement in HRQoL, mainly related to physical activities. Previous studies reported that vitamin D deficiency may result in proximal muscle weakness, which could limit a person's capacity to maintain levels of physical activity and/or performance. There is evidence that vitamin D concentrations below 50 nM (20 ng/mL) caused an increased body sway and concentrations below 30 nM (12 ng/mL) decrease muscle strength. 4 Frail older adults may spend fewer hours outdoors than more physically able older adults, and the conversion of 7-dehydrocholesterol to cholecalciferol by ultraviolet B radiation could be reduced. Because frailty and chronic diseases are specific for the third age, prophylactic supplementation with vitamin D may protect or restore physical functioning in frail people. 23 In our study, the locomotor functions domain was improved in more than 20% of patients from both groups. A meta-analysis confirmed that vitamin D supplementation have reduced falls by 20%. 24
There was no evidence of a significant interaction between time and treatment on general health perception and mental functions. However, recent studies noted strong associations amongst 25(OH)D deficiency, mortality and a variety of morbidities. It has been demonstrated that vitamin D insufficiency can increase the risk of aging-related diseases such as respiratory infections, autoimmune diseases, diabetes, hypertension, cardiovascular diseases, multiple sclerosis, seasonal affective disorder, Parkinson's disease, and Alzheimer's disease. 25 In addition to the association between vitamin D deficiency and chronic disease, the 25(OH)D concentrations are connected to frailty. 23,26 Even if vitamin D deficiency has been associated with depression and anxiety, the efficacy of vitamin D treatment on depression remains controversial. 27,28 In our study, the high dose of vitamin D supplementation and the optimal vitamin D status (>75 nM) failed to improve mood. This result could be explained by the fact that the elderly studied came from a nursing home. There is evidence that depression is more often found in institutionalized older adults than in community-dwelling ones. 20 Living in nursing homes was suggested in early studies to be negatively correlated to the level of physical activity and this contributed to depressive symptoms and deterioration of health related quality of life in institutionalized older adults. 29
Our study had certain limitations: lack of a placebo control (a group of older adults in a nursing home not receiving the fortified bread [VFX+VF] as well as controls in non-institutionalized environments); small number of patients (increased the risk of type 2 statistical error, failing to show significance when effect is highly significant); and short time of surveillance. Other limitations: HRQoL evaluations during the cold season; physiologic particularity of the institutionalized older adults; and advancing age, which could have had a negative influence on the results. Due to these limitations, the present study should be regarded as a pilot project paving the way for a more in-depth, large-scale study on the physical and psychological effects of vitamin D supplementation on the elderly.
Conclusions
In nursing home residents, daily consumption of bread fortified with 125 μg vitamin D3 was efficient and safe to raise serum 25(OH)D concentrations to >75 nmol/L and to induce significant improvement of the total score of QUALEFFO-41. Vitamin D supplementation also significantly diminished pain perception and ameliorated physical functions.
The benefit of a vitamin D-enriched diet is a topic of great interest to researchers. Further studies are necessary for a better understanding of the effects of long-term vitamin D supplementation through fortified food in older adults.
Footnotes
Acknowledgments
This research was supported by Nutrigroup Association, Iasi, Romania. The authors express their gratitude to Professor Reinhold Vieth for research assistance and vitamin D assessment in Bone and Mineral Laboratory, Department of Pathology and Laboratory Medicine, University of Toronto, Mount Sinai Hospital, Toronto, Canada.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.