
Abstract
Angiotensin-1-converting enzyme (ACE) inhibitors are widely used in the treatment of cardiovascular diseases. This study sought to investigate the inhibitory effect of two varieties of ginger (Zingiber officinale) commonly consumed in Nigeria on ACE activity in rats fed a high cholesterol diet. The inhibition of ACE activity of two varieties of ginger (Z. officinale) was investigated in a high cholesterol (2%) diet fed to rats for 3 days. Feeding high cholesterol diets to rats caused a significant (P<.05) increase in the ACE activity. However, there was a significant (P<.05) inhibition of ACE activity as a result of supplementation with the ginger varieties. Rats that were fed 4% white ginger had the greatest inhibitory effect as compared with a control diet. Furthermore, there was a significant (P<.05) increase in the plasma lipid profile with a concomitant increase in malondialdehyde (MDA) content in rat liver and heart tissues. However, supplementing the diet with red and white ginger (either 2% or 4%) caused a significant (P<.05) decrease in the plasma total cholesterol, triglyceride, very low density lipoprotein-cholesterol, and low-density lipoprotein-cholesterol levels, and in MDA content in the tissues. Conversely, supplementation caused a significant (P<.05) increase in plasma high-density lipoprotein-cholesterol level when compared with the control diet. Nevertheless, rats fed 4% red ginger had the greatest reduction as compared with control diet. In conclusion, both ginger varieties exhibited anti-hypercholesterolemic properties in a high cholesterol diet fed to rats. This activity of the gingers may be attributed to its ACE inhibitory activity. However, white ginger inhibited ACE better in a high cholesterol diet fed to rats than red ginger. Therefore, both gingers could serve as good functional foods/nutraceuticals in the management/treatment of hypertension and other cardiovascular diseases.
Introduction
C
Experimental and clinical studies have shown that the amount of cholesterol transported in the very low density lipoprotein (VLDL) and low density lipoprotein (LDL) classes of lipoproteins, known as pro-atherogenic cholesterol, is a risk factor for the occurrence of cardiovascular disease. 4 In contrast, cholesterol transported in high-density lipoprotein (HDL) particles, known as anti-atherogenic cholesterol, has a protective effect on cardiovascular disease. 4 The control of cholesterol levels through therapeutic drugs has significantly reduced the risk for developing atherosclerosis and its associated cardiovascular diseases. 5 Notably, statins, a class of cholesterol-lowering drugs inhibiting cholesterol synthesis, have been most widely prescribed for treating hypercholesterolemia and reducing cardiovascular diseases. 6,7 However, the adverse effects associated with therapeutic drugs, such as myopathy, liver damage, and potential drug–drug interaction, have been reported. 8,9 Therefore, development of additional therapies for controlling cholesterol levels is warranted, especially for those with a better safety profile.
The renin–angiotensin–aldosterone system is a major endocrine/paracrine system that is involved in the regulation of a myriad of cardiovascular processes. 10 Its role in the pathogenesis of hypertension, cardiac hypertrophy, and atherosclerosis is well established. Since angiotensin-1 converting-enzyme (ACE) inhibitors exhibit cardioprotective, vasculoprotective, antiatherogenic effects and contribute to tissue protection, they are widely used in the therapy of cardiovascular disease. 11,12 ACE is a zinc-metallopeptidase that converts angiotensin I to the potent vasoconstrictor angiotensin II by removing His-Leu from C-terminal. ACE also degrades bradykinin, a powerful vasodilator that plays critical roles in the regulation of vascular tone and cardiac functions. 13 Angiotensin II has been suggested to be involved in diabetic cardiovascular pathogenesis and nephropathy. 14 An increase in ACE activity has been reported in diabetic patients and animal models. 15,16 It has also been shown that ACE activity increased in serum and some tissues such as aorta and lung in STZ-induced diabetic rats. 17 The increase in ACE activity is believed to influence the development of hypertension. Furthermore, reports have shown that hypercholesterolemia favors the progression of hypertension via a number of mechanisms, which include enhanced activity of the renin–angiotensin-system (RAS), 18 and hypertension, on the other hand, could increase the accumulation of atherogenic lipoproteins in the arterial wall. 19 Therefore, to control the development of cardiovascular complications in dyslipidemia, treatment strategies should be directed at controlling both hypertension and hypercholesterolemia.
Angiotensin II, an important oxidant, alters the binding of LDL-C to its receptors and increases endothelial uptake of LDL-C. Therapy with ACE inhibitors appears to eliminate these untoward effects and may ameliorate the tendency for myocardial infarction that is associated with elevated plasma levels of angiotensin II. 20 Ginger (Zingiber officinale Roscoe, Zingiberaceae) is widely used around the world in foods as a spice. For centuries, it has been an important ingredient in Chinese, Ayurvedic, and Tibb-Unani herbal medicines for the treatment of catarrh, rheumatism, nervous diseases, gingivitis, toothache, asthma, stroke, constipation, hypertension, and diabetes. 21 –23 The active ingredients in ginger root include volatile oils and pungent phenol compounds known as gingerols, sesquiterpenoids, and shogaols, whereas red ginger has been shown to contain anthocyanin and tannin besides having gingerols and shogaols. 24 Ginger has been listed in “Generally Recognized as Safe” documentation of the U.S. FDA. A dose of 1–5 g of ginger powder ingested 2–3 times for periods ranging from 3 months to 2.5 years did not cause any adverse effects. 25 Recently, Oboh and colleagues 26 reported that two varieties of ginger inhibit ACE activity in vitro. Although ginger has been reportedly used in folklore for the management/prevention of hypertension and other cardiovascular diseases, there is dearth of information on the possible mechanism of action by which they exert this effect. Hence, the objective of this study is to investigate the inhibitory effect of 2% and 4% (a dosage generally safe for rat) of two commonly consumed varieties of ginger (Z. officinale) in Nigeria on ACE in a high cholesterol diet fed to rats for 3 days in order to provide information as to whether they will exert antihypercholesterolemic properties with a short-term treatment.
Materials and Methods
Materials
Sample collection
Fresh samples of white ginger (Z. officinale Roscoe) and red ginger (Z. officinale var. Rubra) were purchased from the local market (Akure metropolis, Nigeria). Authentication of the plants was carried out by K. Oladunjoye at the Department of Biology, Federal University of Technology, where voucher specimens (no. 2360a and 2360b) were deposited at the Herbarium.
Chemicals and reagents
Chemicals and reagents used such as Hippuryl-histidyl-leucine substrate, thiobarbituric acid (TBA), and acetic acid reagent were procured from Sigma-Aldrich, Inc., (St. Louis, MO, USA); Tris-HCl buffer, sodium dodecyl sulphate (SDS), and malondialdehyde (MDA) were of analytical grade, while the water was glass distilled. All the kits used for the bioassay were sourced from Randox Laboratories Ltd. (Crumlin, Northern Ireland, United Kingdom).
Diet composition
Diets containing 2% and 4% Z. officinale and basal diet for control animals were formulated in consultation with the Department of Animal Production and Health, Federal University of Technology (Table 1).
Basal, without cholesterol and test samples; control, 2% cholesterol without test samples; 2% RG, 2% red ginger; 4% RG, 4% red ginger; 2% WG, 2% white ginger; 4% WG, 4% white ginger.
Grouping of animals and study design
The bioassay was carried out according to the method described by Bjorkhem and Akerlund, 3 where the hypercholesterolemia rat model was achieved by feeding rats with a 2% cholesterol-supplement diet for 3 days. Wistar strain albino rat weighing 75–183 g from the Department of Animal Production and Health, Federal University of Technology were acclimatized for 2 weeks and placed ad libitum on a commercial diet. The handling of animals was carried out in accordance with the recommended international standard. The rats were subsequently divided into six different groups: Group 1 was placed on a basal diet (without cholesterol and test samples); Group 2 served as the control and was placed on a diet that contained 2% cholesterol without test samples; Groups 3 and 4 were fed a diet supplemented with 2% and 4% red ginger and 2% cholesterol inclusion, respectively, while Groups 5 and 6 were fed a diet supplemented with 2% and 4% white ginger and 2% cholesterol inclusion, respectively. After the end of the experiment (3 days), the rats were killed by cervical dislocation and blood was withdrawn by heart puncture, after which the plasma was prepared.
Preparation of plasma
Animals were dissected, and blood from the inferior venacava of the heart was collected into ethylenediaminetetraaceticacid-containing tubes without any protease inhibitors and centrifuged at 3000 g for 15 min in an MSC bench centrifuge (Beckman Coulter, Fullerton, CA, USA). The clear supernatant obtained (plasma) was used in estimation of the lipid profile of the animals.
Assay Methods
Determination of ACE activity
The plasma ACE activity was determined as described by Cushman and Cheung. 27 The substrate [hippuryl-histidyl-leucine (Bz-Gly-His-Leu)] were purchased from Sigma-Aldrich. The amount of cleaved hippuric acid from hippuryl-histidyl-leucine was measured by the enzymatic method. Fifty microliters of plasma and 150 μL of 8.33 mM of hippuryl-histidylleucine (Bz-Gly-His-Leu) in 125 mM Tris-HCl buffer (pH 8.3) were incubated at 37°C for 30 min. After incubation, the reaction was arrested by adding 250 μL of 1 M HCl. The Gly–His bond was then cleaved, and the hippuric acid produced by the reaction was extracted with 1.5 mL ethyl acetate. Next, the mixture was centrifuged to separate the ethyl acetate layer; then, 1 mL of the ethyl acetate layer was transferred to a clean test tube and evaporated. The residue was re-dissolved in distilled water, and its absorbance was measured at 228 nm. The ACE activity was expressed as mmol/min/mg protein.
Determination of triglyceride and cholesterol levels
Plasma triglyceride (TG) and cholesterol levels were assayed using commercial diagnostic kits (Randox Labs).
Determination of HDL level
The VLDL and LDL lipoproteins were precipitated by addition of phosphotungstic acid and magnesium chloride. After centrifugation, the supernatant containing the HDL fraction was assayed for cholesterol with commercial diagnostic kits (Randox Labs).
Determination of LDL cholesterol level
The LDL cholesterol was calculated using the formula of Friedewald et al. 28
Determination of lipid peroxidation level
The liver and heart lipid peroxidation levels were assessed by measuring the TBA-reacting substances formed as described by Ohkawa et al. 29 The color reaction was developed by adding 300 μL 8.1% SDS to the reaction mixture containing 300 μL of tissue homogenate, and this was subsequently followed by the addition of 600 μL of acetic acid/HCl (pH 3.4) mixture and 600 μL of 0.8% TBA. This mixture was incubated at 100°C for 1 h. TBA reactive species produced were measured at 532 nm and expressed as nmol/g protein.
Data analysis
All experiments were carried out in triplicate. Data were expressed as mean±standard deviation. Differences were evaluated by one-way analysis of variance followed by Duncan's multiple range test. Significance was accepted at P<.05. 30
Results
The results as shown in Figure 1 revealed that there was a significant increase (P<.05) in the ACE activity in rats fed a 2% cholesterol diet (control) when compared with the basal group (without cholesterol). However, there was a significant (P<.05) inhibitory effect of ACE activity as a result of supplementation with 2% and 4% red and white ginger. Nevertheless, rats fed 4% white ginger had the greatest inhibitory effect as compared with the control diet.
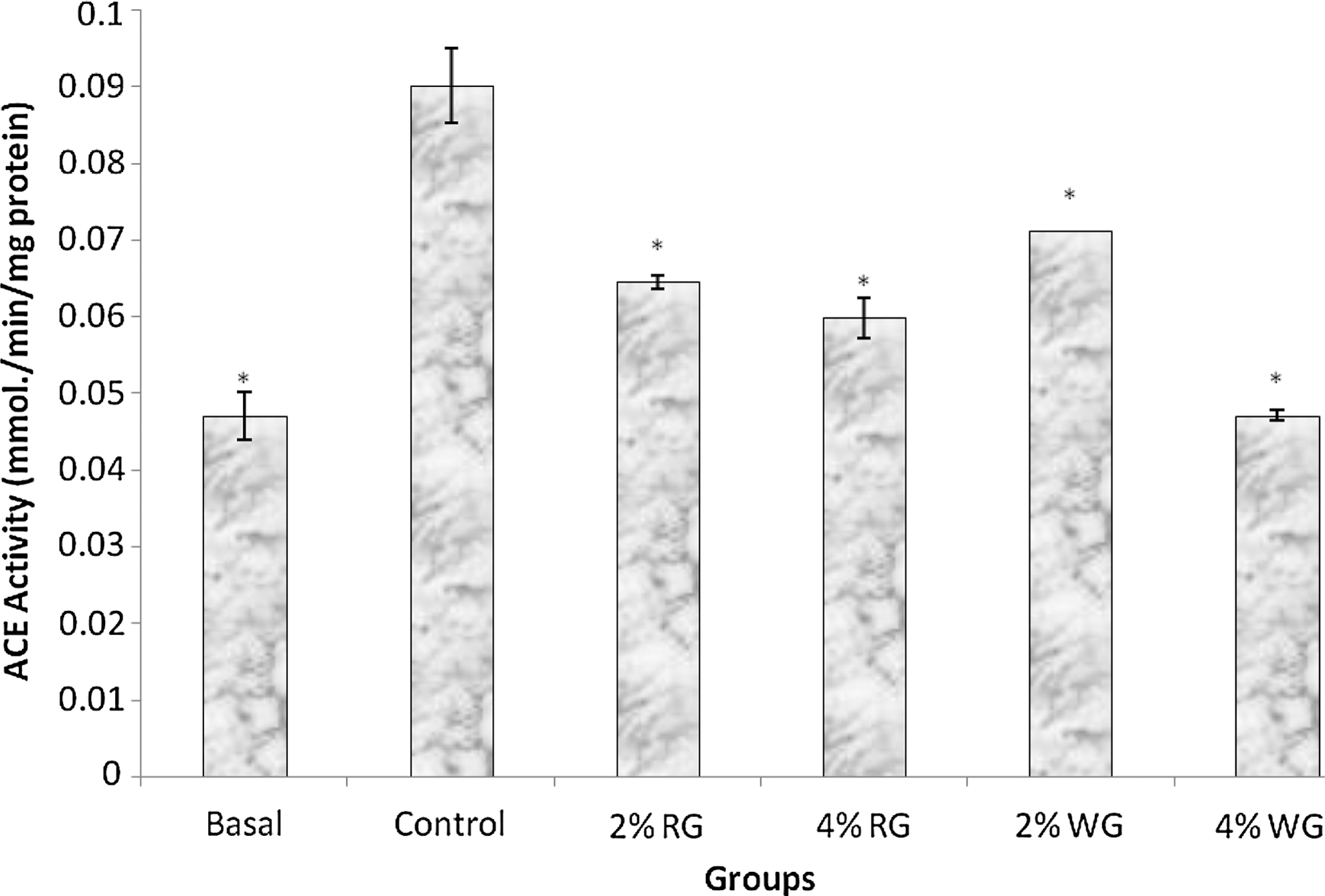
Inhibition of angiotensin-1-converting enzyme (ACE) activity by supplementation of red and white ginger (2% and 4%) in high cholesterol diet fed to rats. n=6. *Significantly different from control group at P<.05. Basal, without cholesterol and test samples; control, 2% cholesterol without test samples; 2% RG, 2% red ginger; 4% RG, 4% red ginger; 2% WG, 2% white ginger; 4% WG, 4% white ginger.
Furthermore, there was a significant (P<.05) increase in the total cholesterol (TC) level of the plasma. However, at both 2% and 4% inclusion of the gingers, there was a remarkable decrease in the TC level, with rats fed a 4% red ginger having the greatest reduction as compared with the control diet (Fig. 2).
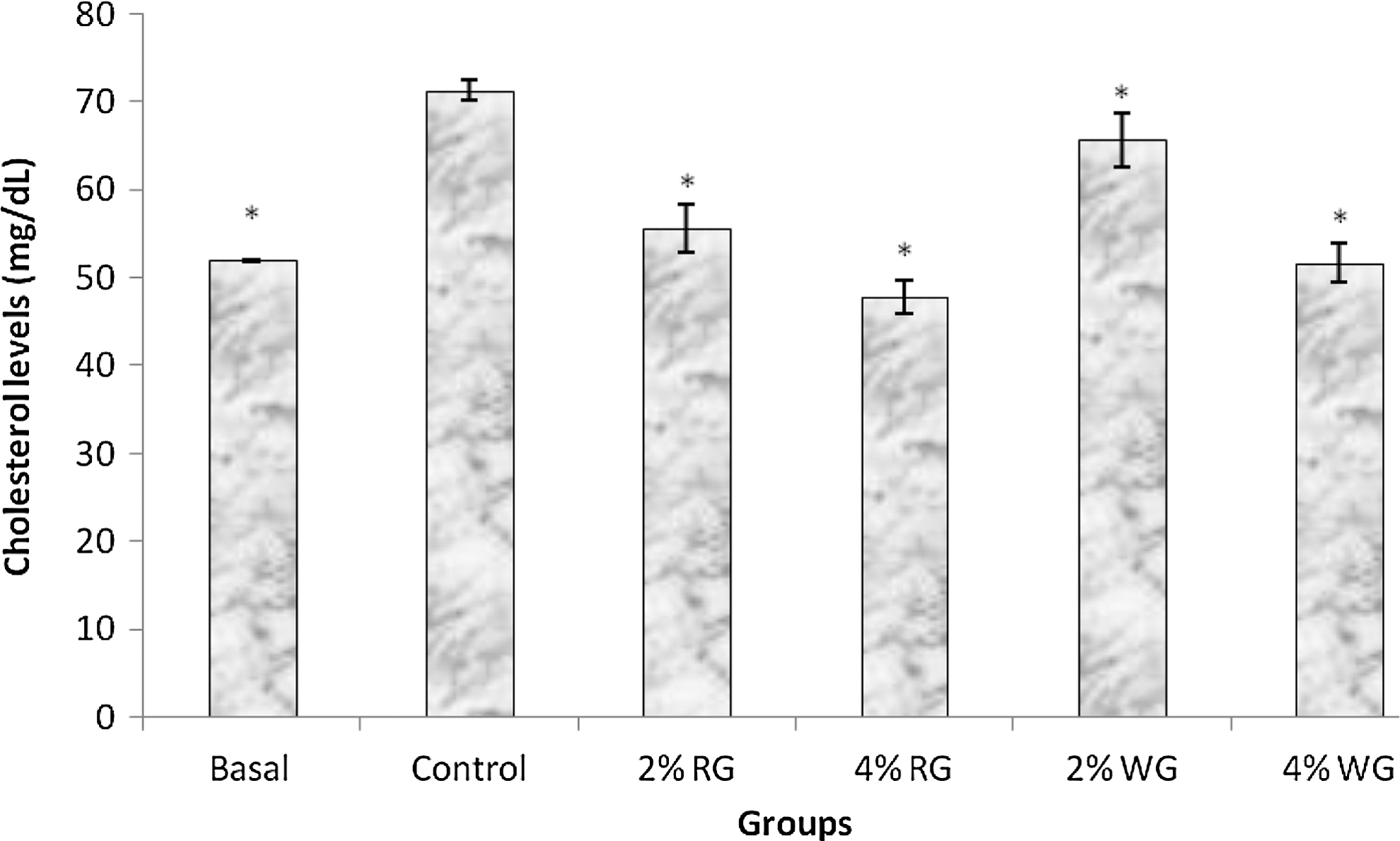
Effect of supplementation of red and white ginger (2% and 4%) on total cholesterol levels in high cholesterol diet fed to rats. n=6. *Significantly different from control group at P<.05.
In addition, there was a significant (P<.05) increase in the TG level in rats fed a 2% cholesterol diet (control) as shown in Figure 3. However, at both 2% and 4% inclusion of the gingers, there was a remarkable decrease in the TG level, with rats fed 4% red ginger having the greatest reduction as compared with the control diet.
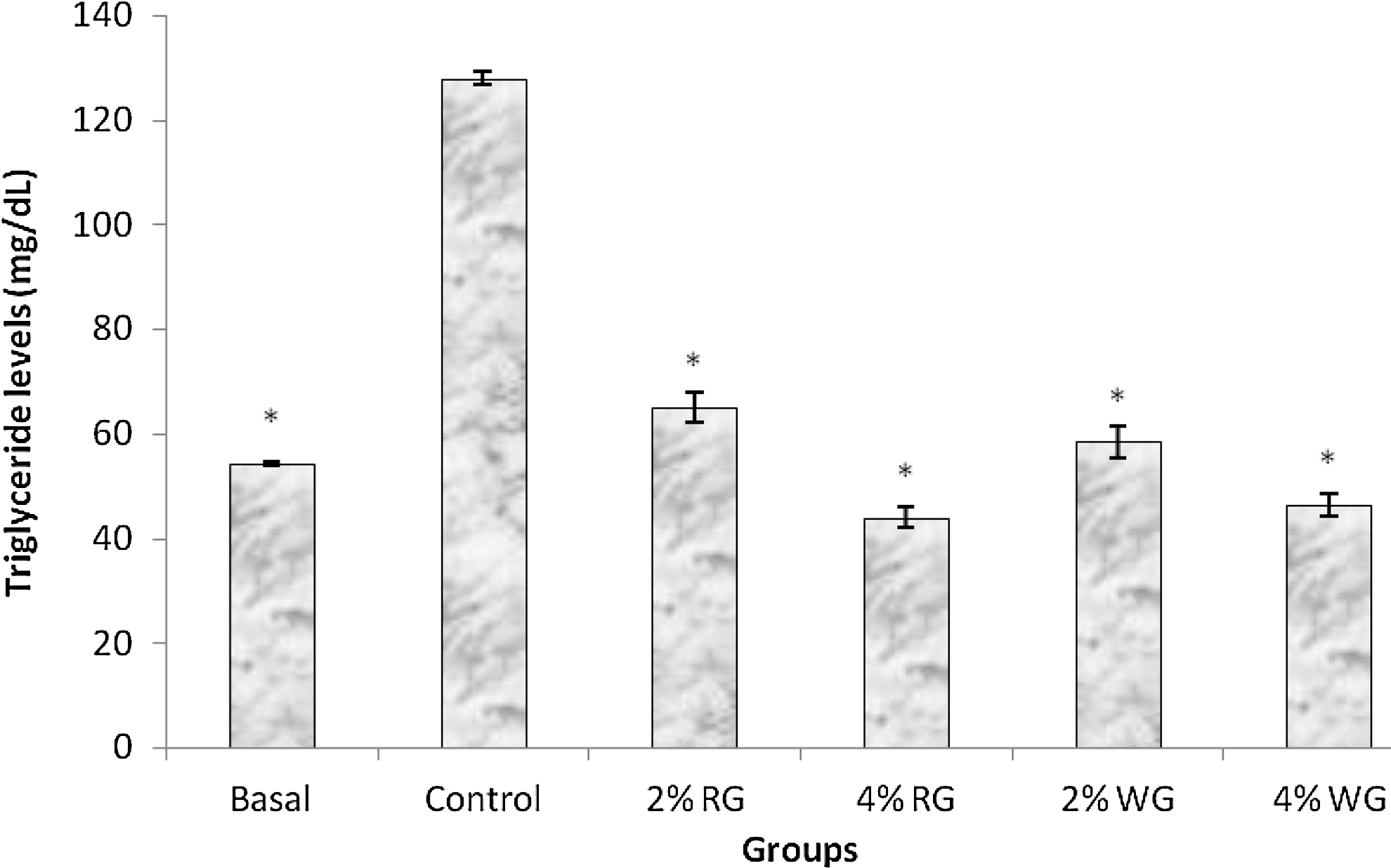
Effect of supplementation of red and white ginger (2% and 4%) on triglyceride levels in high cholesterol diet fed to rats. n=6. *Significantly different from control group at P<.05.
In addition, as shown in Figures 4 and 5, respectively, feeding 2% cholesterol to rats revealed that there was a significant (P<.05) increase in the VLDL-cholesterol (VLDL-C) and LDL-C levels, respectively. However, supplementation with both 2% and 4% red and white ginger caused a remarkable decrease in the VLDL-C and LDL-C levels, with rats fed 4% red ginger having the highest lowering effect as compared with the control diet.

Effect of supplementation of red and white ginger (2% and 4%) on VLDL-cholesterol levels in high cholesterol diet fed to rats. n=6. *Significantly different from control group at P<.05.

Effect of supplementation of red and white ginger (2% and 4%) on low-density lipoprotein-cholesterol (LDL-C) levels in high cholesterol diet fed to rats. n=6. *Significantly different from control group at P<.05.
Conversely, there was a significant (P<.05) increase in the HDL-cholesterol (HDL-C) levels of animals fed supplemented diets when compared with the control diet (Fig. 6). However, there was no significant difference in the HDL-C levels among the treated groups.
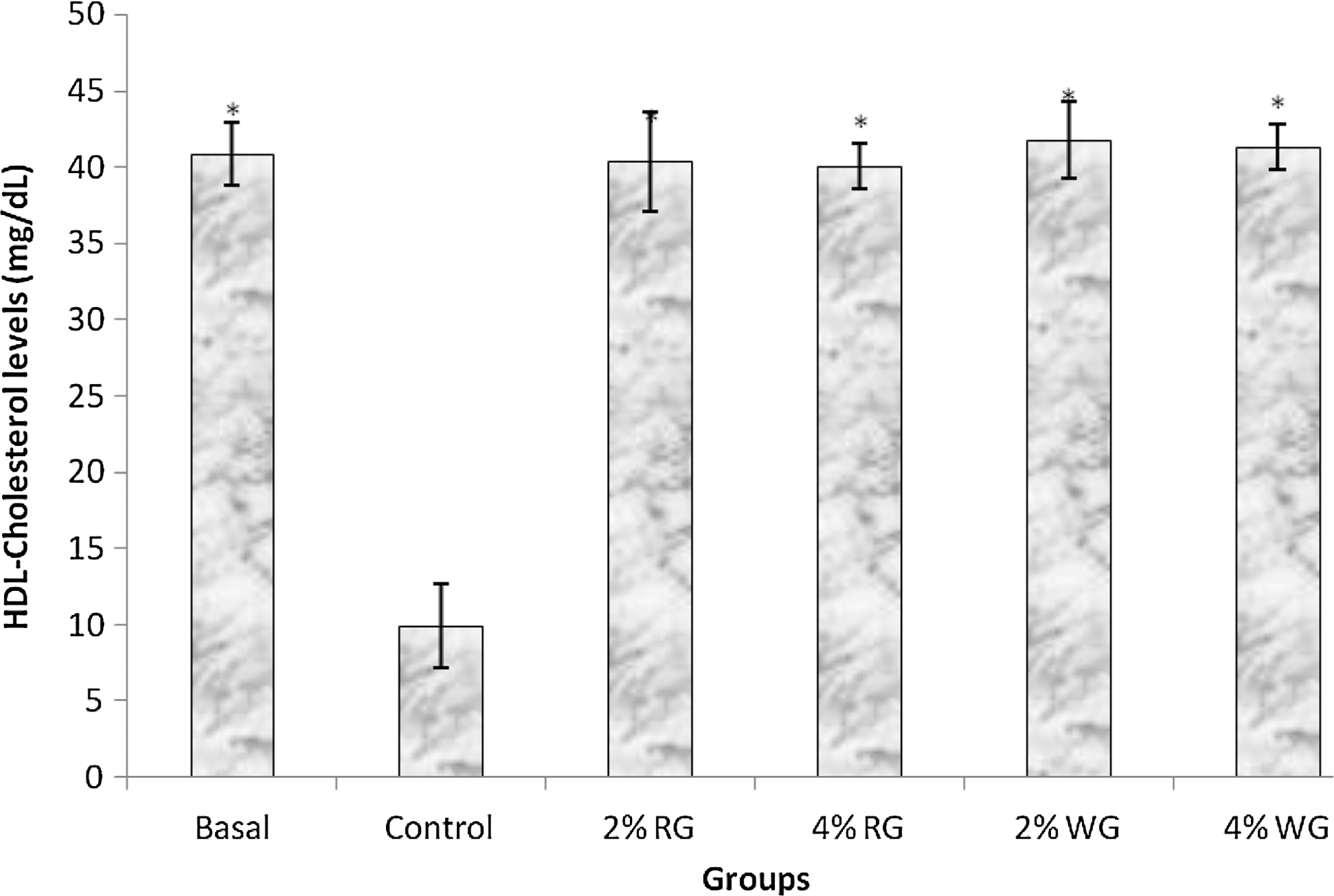
Effect of supplementation of red and white ginger (2% and 4%) on high-density lipoprotein-cholesterol (HDL-C) levels in high cholesterol diet fed to rats. n=6. *Significantly different from control group at P<.05.
The result shown in Figure 7 revealed that feeding 2% cholesterol to rats caused a significant (P<.05) increase in the MDA content of the heart and liver tissue when compared with the basal group (without cholesterol). However, supplementation with 2% and 4% red and white ginger, respectively, caused a remarkable decrease in the MDA content of the heart and liver tissue when compared with the control diet.
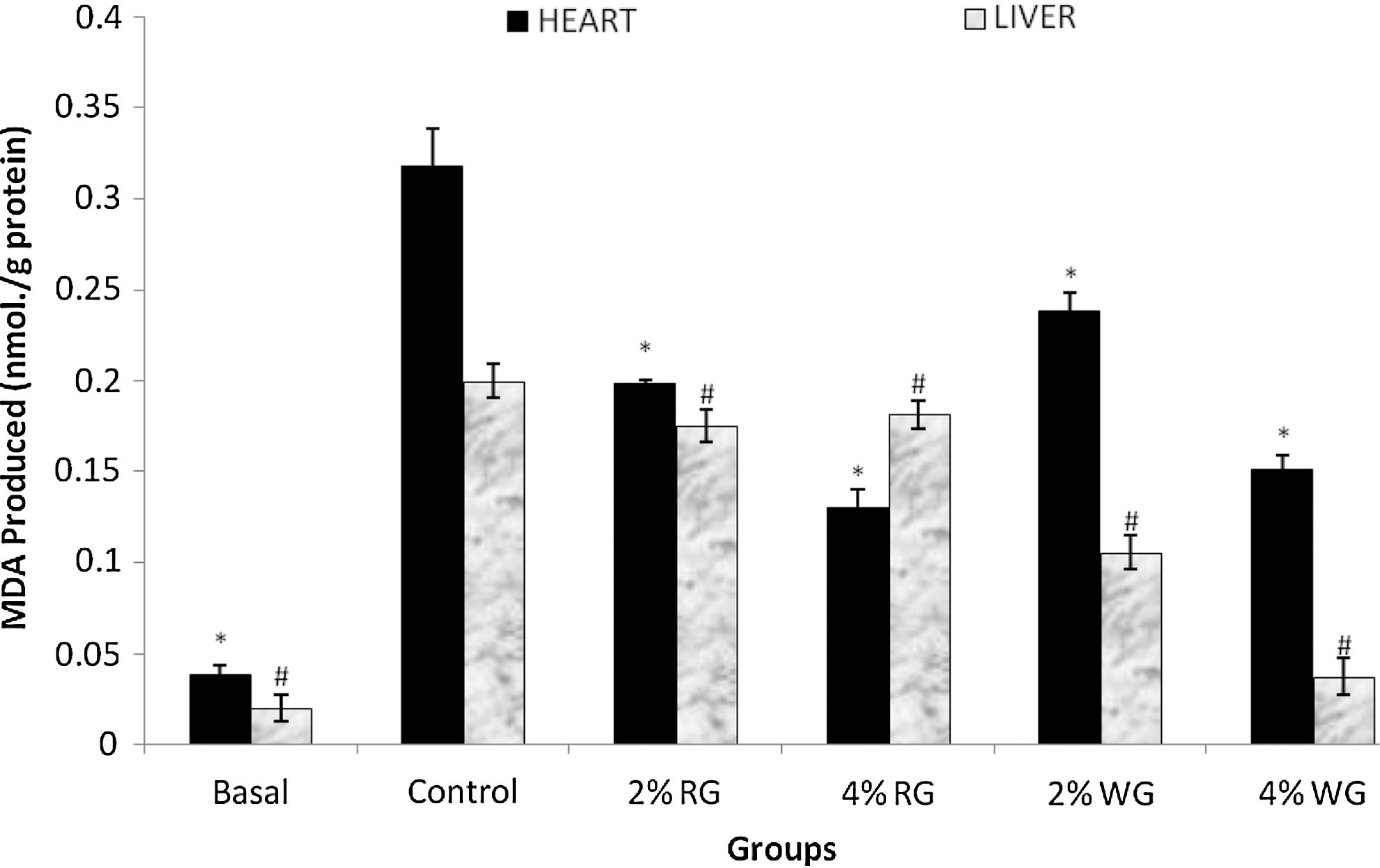
Inhibition of liver and heart malondialdehyde (MDA) level by supplementation of red and white ginger (2% and 4%) in high cholesterol diet fed to rats. n=6. *,#Significantly different from control group at P<.05.
Table 2 depicts the atherogenic indices as affected by supplementation with 2% and 4% red and white ginger in a high cholesterol diet fed to rats. The result revealed that the control group had a significantly (P<.05) increased atherogenic index as compared with the basal group. However, both 2% and 4% red and white ginger diets fed to the groups exhibited significantly (P<.05) reduced atherogenic indices when compared with the control group.
Values represent mean±standard deviation (n=6).
Significantly different from control group at P<.05.
AIP, atherogenic index=log (TG/HDL-cholesterol); TG, triglyceride; HDL, high-density lipoprotein.
Discussion
Hypercholesterolemia is regarded a major risk factor for cardiovascular disease, which is a common cause of morbidity and mortality in diabetes. 31 A 3 day's experimental hypercholesterolemic rat was used to evaluate the effect of short-term administration of the gingers on ACE activity in vivo. The increase in the plasma ACE activity in the control group might be associated with their high plasma cholesterol level. Recent findings have shown that hypercholesterolemia stimulates angiotensin peptide synthesis and contributes to atherosclerosis through the AT1A receptor. 32 However, the reduced ACE activity observed in the groups supplemented with red and white ginger, respectively, for 3 days may be due to the bioavailability of their polyphenolic phytoconstituents with potent ACE inhibitory property (Fig. 1). Nevertheless, groups supplemented with white ginger showed stronger inhibition of ACE than the red ginger. The ACE inhibitory action of the gingers in vivo agreed with a recent work by Emanueli et al., 33 where ACE inhibitor ramipril inhibited ACE activity in ischemic muscles at 1 and 3 days. It also agrees with earlier studies on plant food such as garlic. 16 Enzyme inhibitory activities of plant foods have been attributed to their phenol content; therefore, the decrease in ACE activity by two varieties of gingers could be due to the anti-oxidants (phenolics) present in the ginger as already reported by Oboh and colleagues 26 ACE converts angiotensin I to angiotensin II, a powerful vasoconstrictor that has been identified as a major factor in hypertension. As a result, ACE inhibitors have been widely developed to prevent angiotensin II production in cardiovascular diseases. Angiotensin II, an important oxidant, alters the binding of LDL-C to its receptors and increases endothelial uptake of LDL-C. Therapy with ACE inhibitors appears to eliminate this untoward effect. 20
Atherogenic index is a predictor for the development of atherosclerosis and underscores the progression of cardiovascular disease. This present study revealed an agreement between the atherogenic index and the in vivo ACE inhibitory activity in the experimental animals with groups supplemented with white ginger showing stronger inhibition of ACE activity. RAS is well recognized as a complex and relevant cellular pathway that is capable of affecting many mechanisms related to the development of atherosclerosis. 34 Experimental atherosclerosis has been reported to be attenuated through RAS blockade by ACE inhibitors. 35 Hence, the lower atherogenic index in the supplementation of ginger diet-treated groups might be due, in part, to their ACE inhibitory activity. Phytochemicals such as polyphenols have been reported to inhibit the activities of ACE (key enzyme linked to hypertension) in vitro. 36,37
Furthermore, it has also been documented that lowering circulating cholesterol levels can reduce the risk of cardiovascular diseases. 31 This study revealed that a high cholesterol diet (2% diet inclusion) caused a significant (P<.05) increase in the rats' plasma TC, LDL-C, VLDL-C, and TG levels. This is in agreement with earlier findings that a high cholesterol diet caused markedly elevated plasma TC and TG levels in rats. 38 In addition, Kabiri et al. 39 revealed that a high cholesterol diet caused a significant increase in TC, TG, VLDL-C, and LDL-C in rabbits. However, supplementing the diets with red and white ginger (2% and 4%), respectively, caused a significant (P<.05) decrease in all these plasma metabolites compared with the control diet group (Figs. 2 –5); a diet containing 4% red ginger appears the most potent. The hypocholesterolemic effect of the two varieties of ginger is in agreement with earlier reports where legume condiments are shown to possess some cholesterol-lowering agents. 40 However, the mechanism by which these gingers lower plasma cholesterol remains unclear; the high polyphenols 26,41 and anthocyanin 24 of these spices may have influenced this favorable cholesterol metabolism. It is well known that plasma cholesterol concentration can be regulated by cholesterol biosynthesis, cholesterol removal from the circulatory system, the absorption of dietary cholesterol, and its excretion via bile and feces. 42 Phytochemicals such as polyphenols have been reported to inhibit the activities of 3-hydroxyl-3-methylglutaryl CoA reductase; the rate-limiting enzyme in the cholesterol biosynthesis in the liver 43 and also intestinal acyl CoA:cholesterol acyltransferase, which plays a key role in the absorption of cholesterol by esterification of cholesterol before absorption, 38 suggesting that the inhibition of absorption of dietary cholesterol may, at least, be partly responsible for the hypocholesterolemic activities of the spices.
The ginger varieties counteracted hypercholesterolemia by improving plasma lipid profile. Ginger supplementation resulted in a marked increase in the plasma HDL-C levels compared with the control group (Fig. 6). These findings suggest that both red and white ginger could improve the body cholesterol homeostasis. Circulating HDL-C is regarded “good cholesterol” that carries cholesterol from peripheral cells to the liver where the cholesterol is metabolized into bile acids. 44 This pathway is crucial for maintaining cholesterol homeostasis between blood and peripheral tissues.
Hypercholesterolemia has been reported to be related to enhanced oxidative stress and increased lipid peroxidation, 45 and an increase in oxidized LDL generation was identified as a major contributor to the vascular damage induced by high cholesterol levels. 46 Therefore, inhibiting oxidative stress in hypercholesterolemic state is considered an important therapeutic approach. Polyphenol are plant phytochemicals that are reported to possess strong antioxidant properties and an increase in the consumption of food which is rich in polyphenols has been inversely linked to the occurrence of cardiovascular diseases. Polyphenols are capable of scavenging free radicals, chelating transition metals, preventing the oxidation of LDL-C, and inhibiting lipid peroxidation. 47 A report has shown an inverse correlation between polyphenol (flavonoid) intake and total plasma cholesterol concentrations. 48
In the present study, the effect of high cholesterol (2%) diets on liver and heart MDA contents was investigated (Fig. 7). The result showed that there was a significant (P<.05) increase in the liver and heart MDA contents of the group fed with high cholesterol (2%) diets. The tissue MDA levels (a primary product of lipid peroxidation) for all the groups agree with the plasma LDL-C level. However, the spices-supplemented groups showed a significant (P<.05) decrease in the tissues MDA level when compared with the control group. This clearly indicates a marked improvement in the in vivo antioxidant status with supplementation of the diets with regard to the spices that are rich in antioxidant phytochemicals such as polyphenols. 41
Conclusion
Ginger exhibited antihypercholesterolemic properties in a high cholesterol diet fed to rats. This activity of the gingers may be attributed to its ACE inhibitory activity. However, white ginger inhibited ACE better in vivo in a high cholesterol diet fed to rats. Therefore, both gingers could serve as good functional foods/nutraceuticals in the management/treatment of hypertension and other cardiovascular diseases. Further work on the use of a hypertensive animal model is in progress in our laboratory.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.