
Abstract
We evaluated the effects of Brassica rapa ethanol extract (BREE) on body composition and plasma lipid profiles through a randomized, double-blind, and placebo-controlled trial in overweight subjects. Fifty-eight overweight participants (age 20–50 years, body mass index23.0–24.9) were randomly assigned to two groups and served BREE (2 g/day) or placebo (starch, 2 g/day) for 10 weeks. Body compositions, nutrients intake, plasma lipids, adipocytokines, and hepatotoxicity biomarkers were assessed in all subjects at baseline and after 10 weeks of supplementation. The plasma total cholesterol (total-C) concentration was significantly increased after 10 weeks compared to the baseline in both groups. However, BREE supplementation significantly increased the high-density lipoprotein cholesterol (HDL-C) concentration and significantly reduced the total-C/HDL-C ratio, free fatty acid, and adipsin levels after 10 weeks. No significant differences were observed in body compositions, fasting blood glucose, plasma adipocytokines except adipsin, and aspartate aminotransferase and alanine aminotransferase activities between before and after trial within groups as well as between the two groups. The supplementation of BREE partially improves plasma lipid metabolism in overweight subjects without adverse effects.
Introduction
O
A westernization of diet and less physical activity have rapidly increased obesity or overweight in most Asian nations, including South Korea. 4 Throughout the world, more than a billion people are overweight, more than 300 million are obese, and one-third of the Koreans are overweight.
Turnip or Brassica rapa L. has been traditionally used to treat some diseases, such as hepatitis, jaundice, sore throats, and some cancer 5 as well as to make Kimchi, a Korean traditional fermented vegetable food. Several researches reported that B. rapa ethanol extract (BREE) protects against some cancers and cisplatin-induced nephrotoxicity 6,7 as well as exerts antidiabetic effects, 8 and arvelexin, an active component of BREE, has anti-inflammatory effects. 9 However, the effectiveness of BREE has been mainly demonstrated from animal studies. Therefore, randomized, double-blind, and placebo-controlled trials are essential to determine its effectiveness and validity as a natural food supplement.
The present study was conducted to determine the biological usefulness of the turnip (B. rapa) root, on weight loss and improvement of lipid metabolism, in overweight subjects consuming their habitual diet.
Materials and Methods
Study participants and design
Fifty-eight volunteers aged 20–50 years were recruited from the local community. BMI was based on the new standard for overweight in Asians (BMI 23.0–24.9) revised by IOTF of IASO. 1 All selected participants had no chronic diseases, infectious diseases, pregnancy, or recent surgery. The study was performed in accordance with the Declaration of Helsinki. All subjects provided written informed consent before participating in this study. The study protocol was approved by the Kyungpook National University Human Research Committee (Trial No. KNU-2010-2).
Study protocols
Subjects were randomly divided into two nutritional intervention groups: BREE (n=29) and placebo (n=29). Both subjects and investigators were blinded to the nutritional intervention allocated. Subjects were instructed to maintain their routine food intake and physical activity throughout the course of this study.
At baseline and after the 10-week nutritional intervention, height, weight, and other body compositions were measured using the X-Scan plus II body composition analyzer (Jawon Medical Co.), and the BMI and waist-to-hip ratio (WHR) were calculated according to the respective formula. Blood pressure (BP) was measured using an automatic BP monitor (Omron). We collected the blood after fasting for 12 h, and blood samples were centrifuged at 3000 g, 4°C for 15 min after heparinization and stored at −70°C. Fasting blood glucose (FBG) was measured by GlucoDoctor (allmedicus).
Food intake was recorded before and during the nutritional intervention trial using a 24-h dietary recall. Nutritional analysis was performed using CAN-Pro 3.0 software (The Korean Nutrition Society), which provides a comprehensive database of the nutritional content of general foods and specialty Korean foods.
Nutritional intervention
Subjects consumed either four capsules containing BREE (2000 mg/day, 500 mg/capsule; Yuyu Health Care Co.), or four capsules, which contained cornstarch (2000 mg/day, 500 mg/capsule; Yuyu Health Care Co.) in the morning and evening daily for 10 weeks. The compliance of subjects to the nutritional intervention and capsule consumption were regularly monitored every second day by telephone during the 10 weeks.
Preparation of BREE
The fresh roots from the GangHwa County Agricultural Technology Center (Incheon, Republic of Korea) were cut and extracted three times with 95% ethanol at room temperature. The combined BREE were evaporated in vacuo to obtain 10.6 g per 100 g of fresh root material. A voucher specimen (No. 051575) has been deposited at the Laboratory of Natural Product Chemistry, Kyung Hee University, Suwon, Korea.
Plasma lipid analyses
Plasma total cholesterol (total-C), triglyceride (TG), high-density lipoprotein (HDL)–cholesterol (HDL-C), and free fatty acid (FFA) concentrations were determined using commercial kits (Asan Pharm. Co.). The total-C/HDL-C ratio (THR) and non-HDL-C were calculated according to the respective formula.
Plasma adipocytokines and hepatotoxicity analyses
Plasma adiponectin, adipsin, leptin, resistin, tumor necrosis factor-α (TNF-α), and interleukin-6 (IL-6) were measured using multiplex detection kits (Bio-Rad). Data analyses were performed using the Bio-Plex Manager software version 4.1.1 (Bio-Rad).
Plasma aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were determined using commercial kits (Asan Pharm. Co.).
Statistical analysis
All data are presented as mean±SEM. Statistical analysis was performed using SPSS software (version 11.5). Significant changes in respective parameters within group and between baseline and 10 weeks were assessed using a paired-samples t-test. Significant differences between BREE and placebo groups at baseline and at 10 weeks were analyzed using an independent-samples t-test. Statistically significant differences were accepted at P<.05.
Results
Baseline clinical characteristics
There were no dropouts during the experimental periods in either group. There were no significant differences in any baseline characteristics between subjects in BREE and placebo groups. FBG and BP of all subjects were within the normal range, and BMI of overweight was within the new standard (23.0–24.9) revised by WHO, IASO, and IOTF (Table 1). 1
Values are mean±SEM.
Starch.
BREE, Brassica rapa ethanol extract; FBG, fasting blood glucose; BP, blood pressure; BMI, body mass index; WHR, waist-to-hip ratio=waist/hip; BFP, body fat percentage; LBM, lean body mass=weight (kg)−body fat mass (kg).
Nutrients intake
Baseline nutrient intakes of the two groups were not significantly different in 24-h diet recalls (Table 2). At 0 weeks, the daily energy intake, the protein:fat:carbohydrate (PFC) ratio, and nutrients intakes were within the currently recommended guidelines of the Dietary Reference Intakes for Koreans from The Korean Nutrition Society. The total energy intake was increased by a higher carbohydrate and fat intake than at baseline without changing the PFC ratio in both groups. The cholesterol intake was significantly increased (P<.001) in both the placebo and BREE groups, compared to before trial. Nevertheless, there was no significant difference in other nutrient intakes between the two groups during the trial.
Values are mean±SEM.
Starch.
P<.001: Data are compared before and after 10 weeks by a paired-samples t-test.
Body compositions
BREE supplementation for 10 weeks did not affect any indices, including body weight, BMI, WHR, body fat percentage, internal fat, lean body mass, and muscle mass (Table 1). Similar results were found in the placebo group. There were no significant differences between groups after the trial (Table 1).
Plasma lipid profiles
At the baseline, the levels of total-C and TG were within normal range, and there were no significant differences in any plasma biomarkers between the placebo and BREE groups (Fig. 1). However, the plasma total-C concentration was significantly higher after 10 weeks than before the trial in both the placebo (P<.001) and BREE (P<.01) groups (Fig. 1A) without difference between the two groups. A non-HDL-C concentration significantly increased after the 10-week trial in the placebo group only (P<.01; Fig. 1A). BREE supplementation significantly increased the plasma HDL-C concentration (P<.01; Fig. 1B) and significantly decreased THR and plasma FFA levels (P<.05; Fig. 1C) after the 10-week trial when compared to baseline values. Both THR and plasma FFA levels were significantly lower in the BREE group than in the placebo group after 10 weeks (Fig. 1C). The placebo group did not show any changes in any plasma parameters except total-C and non-HDL-C levels (Fig. 1A). BREE supplementation for 10 weeks did not affect TG and non-HDL-C levels. There were no significant differences in plasma total-C, non-HDL-C, TG, and HDL-C concentrations between the placebo and BREE groups either before or after trial (Fig. 1A, B).
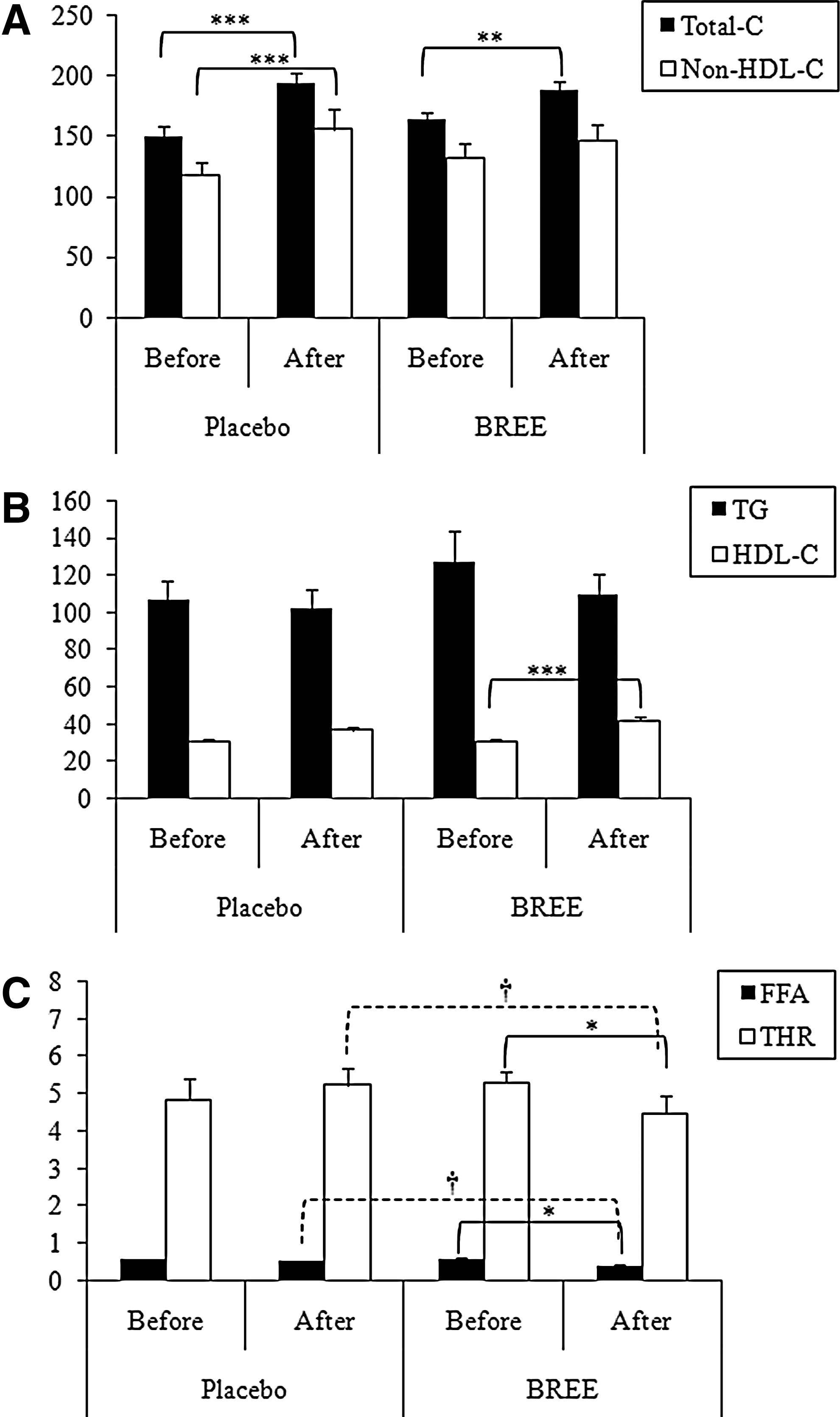
Effect of 10-week Brassica rapa ethanol extract (BREE) supplementation compared to placebo in overweight subjects on
Adipocytokines and hepatotoxicity markers
The plasma adipsin concentration was significantly decreased after 10 weeks in the BREE group (Table 3), whereas the placebo group was significantly higher in the plasma leptin level after the 10-week trial compared to the baseline level. There were no statistical differences in other plasma adipocytokine levels both between before and after trial and between the placebo and BREE groups.
Values are mean±SEM.
Starch.
P<.05: Data are compared before and after 10 weeks by a paired-samples t-test.
BREE, Brassica rapa ethanol extract; TNF-α, tumor necrosis factor-α; IL-6, interleukin-6; AST, aspartate aminotransferase; ALT, alanine aminotransferase.
Plasma AST and ALT levels were within the normal range and were not significantly influenced by starch or BREE supplements during the 10 weeks (Table 3).
Discussion
In the present study, we attempted to examine the effectiveness of BREE in overweight subjects for the first time. BREE supplementation was not effective for improving body compositions in overweight participants with BMI 23.0–25.0.
The change in the PFC ratio serves to illustrate a broad picture of the nutrition transition in South Korea. The PFC ratio was 13:6:81 in 1940, indicating that the energy intake was mainly from carbohydrate, and the ratio has now shifted to 16:19:64, closer to the recommended ideal ratio after 55 years. 10 The present data showed that all participants had consumed carbohydrate, protein, and fat in proper ratios according to a recommended dietary allowance. Interestingly, the increase of cholesterol intake during the trial period affected the plasma total-C concentration in both the placebo and BREE groups. This was, partly, due to the seasonal preference of subjects consuming cow's intestines in Daegu city.
The prevalence of low HDL-C has increased due to industrialization and almost one-half of the Korean population now has a low HDL-C. 11 Multivariate analysis of the Framingham Heart study and physician's health study demonstrated that the THR is independently related to coronary heart disease in elderly men and women 12,13 and some experts suggest that the goal for the ratio is a value <4.5. 14 The National Cholesterol Education Program Expert Panel has recently suggested that non-HDL-C may be a better predictor of cardiovascular risk than low-density lipoprotein–cholesterol. 15 Based on data presented, all subjects had low plasma HDL-C concentrations below the normal range, without abdominal obesity, hyperglycemia, hypertension, or high TG levels at baseline. However, BREE supplementation significantly elevated HDL-C levels above 40 mg/dL after 10 weeks. For this reason, THR was significantly decreased to <4.5 in the BREE group only, despite the significant increase (P<.01) in the plasma total-C level and no change in non-HDL-C (Fig. 1).
According to several studies, FFA levels are a strong independent predictor of sudden cardiac death and other cardiovascular deaths. 16,17 The significant reduction in the plasma FFA concentration by BREE supplementation, partly, corresponded with previous studies that the BREE supplement significantly reduced total-C and FFA concentrations in the db/db mice. 8
Adipocytes secrete many adipocytokines that contribute to energy homeostasis, regulate the inflammatory responses, and are related to the obesity, diabetes, cardiovascular disease, in both obese animals and humans. 18,19 Leptin is categorized as a proinflammatory substance and is correlated with adiposity and insulin resistance along with TNF-α, IL-6, and resistin. 20,21 For people who are chronically overweight or obese, leptin does not reduce appetite and stimulate fat metabolism due to leptin resistance. 22 On the contrary, adiponectin possesses anti-atherogenic, insulin-sensitizing, and vasodilatory activities. 23,24 Adipsin is primarily synthesized by adipocytes, and the circulating concentration of adipsin tends to correlate positively with the degree of adiposity. 25 As indicated in the results, BREE may be effective for preventing leptin resistance and for increasing adipsin in overweight subjects.
The plasma AST and ALT levels are generally used as an indirect indicator of hepatotoxicity. Overweight or obese individuals have an elevated risk of nonalcoholic fatty liver disease. 26 Overdose and/or misuse of nutritional supplements may also induce hepatotoxicity by increasing the plasma AST and ALT levels. No hepatic side effects were observed in the BREE or placebo group, since AST and ALT were within the normal range.
In summary, BREE supplementation for 10 summa partially improved the lipid profiles, but failed to provide any clinically significant body fat and weight loss in overweight subjects consuming their habitual diet. Further studies will, however, be needed to validate the optimal dose of BREE for plasma lipid-lowering and the body fat reduction effects in obese subjects.
Footnotes
Acknowledgments
This research was supported by a grant from the GangHwa Agricultural Technology Service Center and partly by the Science Research Center program (2011-0000920) of the National Research Foundation of Korea funded by the Ministry of Education, Science and Technology.
Author Disclosure Statement
No competing financial interests exist.