
Abstract
Polycalcium is a mixture of Polycan and calcium lactate–gluconate 1:9 (w/w) with demonstrated antiosteoporosis activity in vitro and in vivo studies. These studies were a 4-week open-label, single-center trial to evaluate the efficacy of oral Polycalcium on bone metabolism and safety. In total, 30 healthy women (range 40–60 years) were administered 400 mg of Polycalcium for 4 weeks. The primary efficacy parameter was urinary deoxypyridinoline (DPYR) levels, and serum osteocalcin (OSC), bone-specific alkaline phosphatase (BALP), urinary cross-linked C-telopeptide of type-1 collagen (CTx), urinary cross-linked N-telopeptide of type-1 collagen (NTx), calcium (Ca), and phosphorus (P) levels, which were evaluated for comparison before and after administration of Polycalcium. After 4 weeks of Polycalcium administration, 27 subjects completed the test plan. Three subjects withdrew their consent to participate. The values of blood OSC, BALP, serum Ca, and serum P from baseline to 4 weeks of treatment were changed by −28.44%, 14.37%, 6.11%, and 1.42%, respectively. Biomarkers of bone resorption: urinary DPYR, serum CTx, serum NTx, urinary Ca, and urinary P, at baseline after 4 weeks of treatment were changed by −13.40%, 6.67%, −5.13%, −22.43%, and −3.04%, respectively. Additionally, when considering the subjects' adverse effects and the results of the blood and urine tests over the 4-week trial period, the dose of 400 mg Polycalcium showed efficacy for improving bone metabolism and was well tolerated and safe. Polycalcium was apparently safe and efficacious.
O
Maintaining a balance between bone formation and resorption is a key to normal bone metabolism, and this process is regulated by osteoblasts and osteoclasts. When the balance is tilted, osteoporosis, the most common bone disease in postmenopausal woman, can occur. Several treatments for osteoporosis, such as hormone replacement therapy (HRT), bone anabolic agents, and antiresorptive agents, have been widely used. 2,3 In postmenopausal osteoporosis, preventing bone loss by inhibiting bone resorption is the conventional approach. 4 Although the current antiresorptive agents are used extensively, there have been many attempts at developing new agents capable of preventing and/or treating bone diseases for many years. 2 There have also been reports on the synergistic effects of these osteoporotic agents. 5,6 It has been reported that various calcium (Ca) salts have preventive or therapeutic benefits for osteoporosis. 7 Ca supplements are important alternative sources of Ca that have positive effects in minimizing bone loss during aging in some patients. 8,9
Polycan is a commercial β-glucan from Aureobasidium pullulans SM-2001, and comprises mostly β-1,3/1,6-glucan and other organic materials, such as amino acids, mono- or di-unsaturated fatty acids (linoleic and linolenic acids), and fibrous polysaccharide. 10 Recently, it has been reported that Polycan has antiosteoporotic effects; it inhibited bone loss and accelerated bone formation, 11 and had fracture-healing–promoting 12 and anti-inflammatory effects. 13 The bioavailability of Ca varies in Ca supplements and can be affected by factors such as disintegration, solubility, chelate formation, and food–drug interactions. 14,15 Polycalcium, a mixed formula consisting of water-soluble Ca salts and Polycan, is regarded as an alternative agent, improving solubility and chelate formation, compared with previous Ca supplements. Additionally, Polycalcium was shown to have synergistic antiosteoporotic effects in vitro, 16 and Polycan was shown to have an antiosteoporotic effect in vivo, 11 demonstrating its potential as a new preventative or therapeutic agent against osteoporosis. However, to our knowledge, there has been no report about whether it has synergistic antiosteoporotic effects in healthy perimenopausal women.
Thus, in the present study, the effects and safety of Polycalcium on markers of bone turnover were evaluated in healthy perimenopausal women. It is expected that the results of this open-label trial can provide basic clinical information about changes in the biochemical markers after Polycalcium treatment.
Thirty healthy woman volunteers, aged 40–60 years, were recruited and enrolled. Written informed consents were obtained from all volunteers before the study, and these women were examined in terms of health status based on clinical history, physical examination, and clinical laboratory testing, including osteocalcin (OSC) and deoxypyridinoline (DPYR; Table 1). Exclusion criteria included a history of treatment with HRT, calcitonin, or bisphosphonates within 6 months; a history of use of β-adrenergic receptor blockers, any hormone product, or a soybean-containing dietary supplement; treatment for hyperlipidemia or an endocrine disorder within 2 months; administration of any medication, including vitamin D or K, or Ca supplements within a month, current use of steroids or herbal medicines known to influence bone metabolism; a history of cancer (e.g., breast, ovarian, endometrial, cervical, and bone) or diagnosed with any disease known to affect bone metabolism (i.e., hepatic, renal, and cardiovascular disease); a history of neurological or psychiatric disease; pregnant or lactating women; women of reproductive age not using a medically accepted method of contraception; and drug addiction. The study was approved by the Daegu Oriental Hospital Institutional Review Board, and the study was conducted in the Daegu Oriental Hospital Clinical Center (Daegu Haany University, Daegu, South Korea). All procedures were conducted in accordance with the ethics standards of the Declaration of Helsinki and Good Clinical Practice Guidelines. This was a 4-week open-label clinical trial to investigate the effects and safety of Polycalcium on bone biochemical markers in healthy woman.
Data are means±SD.
BMI, body–mass index; OSC, osteocalcin; DPYR, deoxypyridinoline; SD, standard deviation.
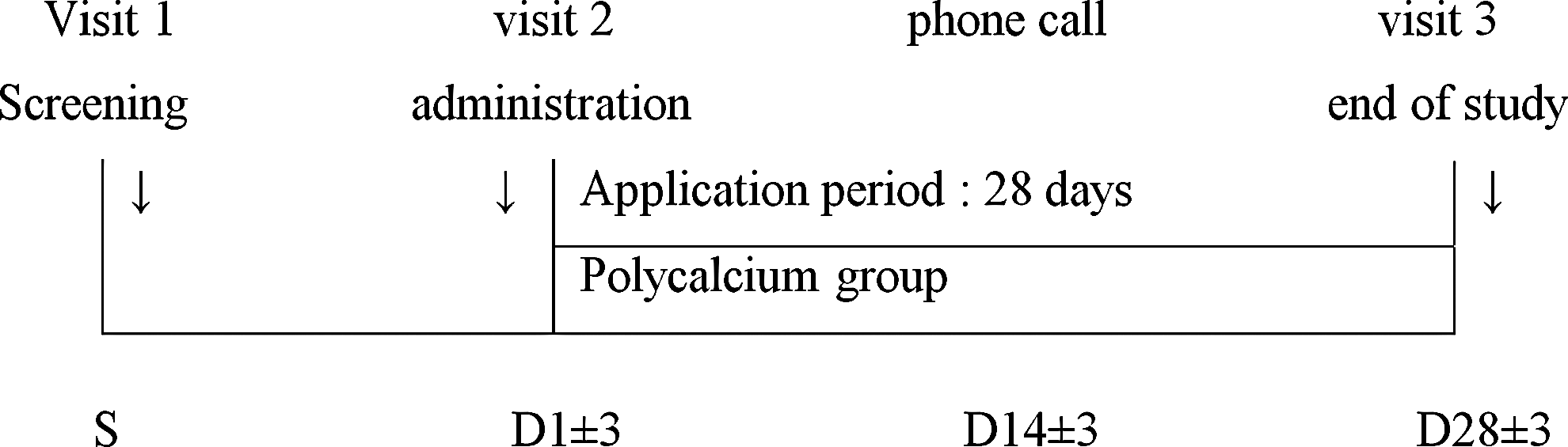
The study consisted of three site visits (screening, baseline, and 4 weeks from baseline) and one telephone contact at 2 weeks from baseline (Fig. 1). All subjects who were confirmed eligible at screening were enrolled and entered the open-label Polycalcium treatment group in the order of enrollment. At the baseline visit, subjects were given a plastic bottle containing a 35-day supply (plus 7 days of surplus tablets) of Polycalcium. They were instructed to take two Polycalcium tablets once a day (total 400 mg/day), 30 min after breakfast with a cup of tap water. The Polycalcium tablets were manufactured by the Silla University Industry-Academic Cooperation Foundation (GMP Certification No. 2008-013; Busan, South Korea), and each Polycalcium tablet contained Polycalcium (Ca:Polycan=9:1) 44.4% and excipients, such as microcrystalline cellulose. To ensure compliance and check for adverse effects (AEs), the subjects received a telephone call from the research staff after 2 weeks. Subjects were asked to bring their bottle to assess treatment compliance at the end of study, and the remaining tablets were counted by staff. Restricted drugs and food during the study included any antiosteoporosis agent, treatment for hyperlipidemia or endocrine disorders, hormone products, antithyroid agents, adrenocortical agents, soybean-containing dietary supplements, vitamins D and K, Ca supplements, and bone-and-joint health supplements.
Flow chart of subjects. Of the 30 women who enrolled, 27 completed the study visits and intervention. Three women were excluded from the efficacy analysis due to poor compliance (<80%).
At each site visit, all subjects were asked to visit at the same time in the morning. Physical examinations, including measurements of the vital signs, were performed, and fasting blood and single midstream spot-urine samples were collected to measure biochemical markers of bone turnover and to assess the laboratory abnormalities at baseline and after 4 weeks. All laboratory tests were performed at the Daegu Oriental Hospital Laboratory (Daegu Haany University), except bone biochemical markers, which were performed at the SungYoon Reference Lab (Daegu, South Korea; Korean Laboratory Accreditation Program certified). Serum OSC and bone-specific alkaline phosphatase (BALP) were measured with a human immunoradiometric assay, serum cross-linked C- and N-telopeptides of type-I collagen (CTx and NTx, respectively) with a two-site enzyme-linked immune sorbent assay, and urinary DPYR with an enzyme immunoassay. Polycalcium safety was evaluated throughout the study, based on laboratory data, self-reported symptoms by subjects, and abnormal signs observed by the clinical investigators. AEs were recorded according to the WHO Adverse Reaction Terminology and evaluated for a causal relationship to the treatment. Data are expressed as means±standard deviation. Differences between baseline and 4-week results were assessed using Student's t-test. Results were considered to be statistically significant when P<0.05.
This study took place between December 2010 and March 2011. Among the 52 women who were screened for the study, 30 subjects participated, and three withdrew after the baseline visit due to adverse events. The baseline characteristics of subjects (mean±SD) are as follows: age 46.79±4.55 years, height 158.35±4.080 cm, weight 58.65±6.567 kg, body-mass index (BMI) 23.39±2.497 kg/m2, OSC 6.69±2.899 ng/mL, and DPYR 5.94±1.510 nM DPYR/mM creatinine (Table 1). The remaining 27 subjects completed the study, and three were excluded from the efficacy analyses due to poor compliance (<80%). Data from 27 subjects were included in the efficacy analyses, and all subjects who took at least one treatment were included in the safety analysis (Fig. 1). The overall compliance was 92.07%±7.05% for 30 subjects, and for the 27 subjects included in the efficacy analyses, the compliance was 93.34%±5.34%.
After 4 weeks of Polycalcium administration, compared with baseline, the primary outcome was the change in the value of serum OSC, and the secondary outcomes were changes in: serum BALP; urinary CTx; urinary NTx, Ca, and phosphorus (P); and urinary DPYR, Ca, and P. Biomarkers of bone formation changed as follows: blood OSC, −28.44%; BALP, +14.37%; serum Ca, +6.11%; and serum P, +1.42% (Table 2). Changes observed in biomarkers of bone resorption were: urinary DPYR, −13.40%; serum CTx, +6.67%; serum NTx, −5.13%; urinary Ca, −22.43%; and urinary P, −3.04% (Table 3). Values of vital signs, body weight, body height, and BMI, red blood cell count (RBC), white blood cell count (WBC), platelet count, hemoglobin, hematocrit, mean corpuscular hemoglobin, mean corpuscular hemoglobin concentration, mean corpuscular volume, aspartate transaminase, alanine transaminase, total protein, albumin, bilirubin (total and direct), uric acid, γ-glutamyl transpeptidase, alkaline phosphatase, glucose, total cholesterol, blood urine nitrogen, creatinine, Na, K, Cl, specific gravity, pH, protein, glucose, ketone bodies, occult blood, bilirubin, urobilinogen, WBC in urine, and RBC in urine at baseline and after 4 weeks of treatment were all within the normal ranges (data not shown), and there was no significant difference between baseline and after 4 weeks of treatment (data not shown). The average compliance of the 27 subjects was 90.0%.
Data are means±SD. n=27.
Result of paired Student t-test with a difference of baseline and after 4 weeks of Polycalcium treatment.
ALP, alkaline phosphatase.
Data are means±SD. n=27.
Result of paired Student t-test with a difference between baseline and after 4 weeks of Polycalcium treatment.
CTx, urinary cross-linked C-telopeptide of type-1 collagen; NTx, urinary cross-linked N-telopeptide of type-1 collagen.
A safety assessment was performed on the 30 subjects who received the treatment at least once. In total, 14 subjects experienced 18 AEs during study, and no event was considered to be related to treatment. There was one case each of abdominal dilation, chronic cough, cold, high fever, cough, coughing cold, diarrhea, dry mouth, fatigue cold, headache, high fever, nausea, periodontitis, and stomach pain, two of brash and phlegm, four of common cold, and six of constipation. There were also some minor laboratory abnormalities of no clinical significance that resolved with no specific intervention (data not shown).
There have been many studies aimed at finding the potential agents for the prevention and treatment of osteoporosis. Long-term use of bisphosphonates is of concern with respect to the accumulation of microdamage to the organic matrix and possible atypical fractures resulting from oversuppresion of bone remodeling. 17 There are two categories of biochemical markers of bone turnover. One consists of markers of bone resorption, reflecting osteoclast activity and other degradation markers, including those of type I collagen. The second category is the markers of bone formation, reflecting osteoblast activity, and includes byproducts of collagen synthesis, matrix proteins, or osteoblastic enzymes. These markers reflect the changes in bone turnover in most situations because bone resorption and formation are interconnected. 18 The most sensitive markers include serum OSC and BALP for bone formation, and DPYR, CTx, and NTx for bone resorption. 19 A specific and responsive bone resorption marker would be helpful for monitoring and establishing the short-term effectiveness of an antiresorptive therapy in patients. 20 In the present study, the effects and safety of Polycalcium were tested in healthy perimenopausal women, based on the changes in bone biomarkers. Among the outcomes in biomarkers of bone formation, a marked change was observed in serum BALP levels, and there was a tendency to suppress the decrease in BALP, serum Ca, and serum P after 4 weeks of Polycalcium treatment, compared with baseline.
To maintain a balance between bone formation and resorption, if bone resorption is reduced, bone formation should also be reduced, resulting in bone homeostasis. However, if excessive bone resorption has already occurred, even though bone resorption activities are suppressed, bone formation activities should increase. As reported previously, 21 OSC is traditionally viewed as a marker of bone formation, but a review of recent literature demonstrates its greater utility as a marker of bone turnover. According to the results of Hozuki et al., 22 increases in the concentrations of carboxylated and under-carboxylated OSC were observed in corticosteroid-treated patients receiving treatment with resedronate with or without vitamin K2 supplementation over 1 year. However, for 1 month after treatment with resedronate with or without vitamin K2 supplementation, the concentrations of both carboxylated and under-carboxylated OSC were decreased. Additionally, when treated with parathyroid hormone or resedronate in a glucocorticoid-induced bone loss mouse model, at 56 days after treatment, osteoclast activity (TRAP5b, serum levels of type-5b tartrate-resistant acid phosphatase, and CTx-1) was increased, and OSC levels were decreased in glucocorticoid-treated mice. Also, both CTx-1 and OSC levels were decreased in resedronate-treated mice. 23 In this study, a significant decrease in OSC was observed after 4 weeks of Polycalcium treatment. This result is consistent with both a previous Polycalcium study 11 and a Polycan animal study, 11 which demonstrated dose-dependent decreases in OSC levels, but somewhat different to a previous clinical trial result, 24 which showed increased OSC levels after 12 weeks of Polycan treatment (150 mg). The differing OSC patterns are probably the result of the differences in the studies (perimenopausal women vs. osteoporotic patients) and the lower dose of Polycan. On the basis of these results, long-term treatment with Polycalcium is thought to provide a protective effect against bone loss.
On the other hand, significant increases in serum BALP were observed in this study. It is known that in postmenopausal osteoporosis, one of the most sensitive markers of bone formation currently available is BALP. 19 This result is consistent with a previous Polycan clinical study. 25 In the development of new drugs, DPYR is an important marker of bone resorption. 19 Because of its inhibiting abilities against bone resorption, substances that decrease DPYR are regarded as bone-healing drugs. 26 In this study, urinary DPYR decreased significantly, compared with baseline. This result is consistent with a previous Polycan clinical study 25 and the effects of pyridinyl bisphosphonates. 26 NTx and CTx are known to be specific and responsive markers among the various bone resorption markers. 26 It has been found that these markers start to increase in the perimenopausal period. 27 One study demonstrated that menopause induced an increase in resorption markers by 79%–97%. The NTx and CTx levels remain elevated for 40 years after menopause. 20 In another study, CTx increased sharply to a level 60% above the premenopausal mean values at menopause. 27 The subjects in the present study were perimenopausal-age women, so their bone biochemical markers probably increased during the study. Among the outcomes in biomarkers for bone resorption, a marked change was observed in urinary DPYR levels, and there was a tendency to suppress the increase in urinary DPYR, serum NTx, urinary Ca, and urinary P after 4 weeks of Polycalcium treatment. These observations tend to suggest that Polycalcium administration resulted in a reduction in bone resorption. After 4 weeks of Polycalcium treatment, CTx showed a slight increase, but it was not significant compared with the baseline value. Indeed, the difference was within the normal range of CTx and the deviation range of the detection kit.
In the safety test of Polycalcium, one person showed multiple symptoms, which were due to influenza. Two subjects who showed brash and phlegm already suffered from gastritis. Four women came down with the common cold. The six cases of constipation occurred in two subjects with gastritis and four with common colds. These minor abnormalities were shown not to be related to Polycalcium, so the safety of Polycalcium is confirmed.
Compared with previous supplements, it is expected that Polycalcium may be a helpful agent for the prevention of osteoporosis. Additionally, Polycalcium was generally well tolerated. 24 The results of this study provide basic clinical information from an open-label trial about changes in the biochemical markers after Polycalcium treatment. However, the present study is a pilot study with some limitations that should be considered, including the small sample size, the short duration of treatment, the lack of hard end points, such as bone mineral density and bone mineral content, large variability in some bone biomarkers, and data gathered from healthy perimenopausal subjects. Further studies, including randomized, double-blind placebo-controlled trials with a longer period of treatment, and larger sample-size patient populations are needed to confirm the present results.
In the present study, we examined the effects and safety of Polycalcium on bone metabolism biomarkers in healthy perimenopausal women. Polycalcium treatment for 4 weeks resulted in improvements in bone metabolism, as indicated by increased biochemical markers of bone formation (BALP, serum Ca, and serum P) and reduced levels of biochemical marker of bone resorption (DPYR, NTx, urinary Ca, and urinary P). Additionally, there was no significant AE with Polycalcium administration for 4 weeks. These results suggest that Polycalcium has the potential to be a clinically useful supplement for treating osteoporosis with a good safety profile.
Footnotes
Acknowledgments
This work was supported by a grant (No. 70007205) from the Ministry of Knowledge Economy, Republic of Korea. J.-S.C. and I.S.C. were also supported by the Global Healthcare Industry RIS Center from the Ministry of Knowledge Economy, Republic of Korea.
Author Disclosure Statement
No competing financial interests exist.