
Abstract
Auraptene is the most abundant naturally occurring geranyloxycoumarin. It is primarily isolated from plants in the Rutaceae family, many of which, like citrus fruits, are used as food in many countries. Auraptene is a biologically active secondary metabolite with valuable properties. The aim of our study was to identify novel properties of auraptene with potential for managing periodontal diseases, an inflammatory disease of bacterial origin affecting the tissues surrounding and supporting the teeth. In vitro assays showed that auraptene decreased, in a dose-dependent manner, the secretion of matrix metalloproteinase 2 as well as key inflammatory mediators, including interleukin-6 (IL-6), IL-8, and chemokine (C-C motif) ligand-5 secreted by Aggregatibacter actinomycetemcomitans lipopolysaccharide-stimulated oral epithelial cells. Using gingival fibroblasts, auraptene showed a significant (P<.05) wound healing effect by its capacity to increase cell migration. In conclusion, auraptene shows promise for promoting wound healing and controlling periodontal diseases through its capacity to interfere with inflammatory mediator secretion.
P
Several groups of investigators have evaluated phytochemicals for their potential for managing periodontal infections. 10 –12 Since the tissue destruction observed in periodontitis involves both pathogenic bacteria and an exaggerated inflammatory response, these two components of the disease process are promising targets for therapeutic management by natural phytochemicals. Auraptene (Fig. 1) is the most abundant naturally occurring geranyloxycoumarin and is mainly isolated from plants belonging to genera of the Rutaceae family, which contains edible fruits and vegetables such as citrus fruits, carrots, and celery. 13 While auraptene has been known for a long time, it has only been in the past 15 years that it has been shown to have promising pharmacological properties as an orally active cancer chemopreventive, antibacterial, antiprotozoal, antifungal, and antioxidant agent. 13 We recently reported that auraptene can inhibit the growth and adherence properties of Porphyromonas gingivalis, 14 a major pathogen associated with the chronic form of periodontitis. 5,15 The present study was undertaken to identify novel properties of auraptene that would provide further support for the potential use of this geranyloxycoumarin in managing periodontal diseases. More specifically, the effects of auraptene on the secretion of MMP-2 and inflammatory mediators such as IL-6, IL-8, and chemokine (C-C motif) ligand (CCL)-5 by lipopolysaccharide (LPS)-stimulated oral epithelial cells were investigated. In addition, the activity of auraptene as a wound healing agent was studied using a gingival fibroblast model.

Structure of auraptene.
Auraptene was synthesized as previously reported. 16 The analytical results were identical to those obtained with a pure commercial product (Sigma-Aldrich Canada, Oakville, ON, Canada). The purity of the synthesized preparation as assessed by gas chromatography–mass spectrometry analysis was greater than 98.6%.
The oral epithelial cell line GMSM-K, which was kindly provided by Dr. Valerie Murrah (Department of Diagnostics Sciences and General Dentistry, University of North Carolina, Chapel Hill, NC, USA), was cultured in the Dulbecco's modified Eagle's medium (DMEM) supplemented with 10% heat-inactivated fetal bovine serum (FBS) and 100 μg/mL of penicillin G/streptomycin at 37°C in a 5% CO2 atmosphere. The epithelial cells were harvested by gentle trypsinization (0.05% trypsin-EDTA; Gibco-BRL, Grand Island, NY, USA), washed once in DMEM-FBS, and suspended at a density of 4×105 cells/mL in the DMEM with 1% heat-inactivated FBS. The cells were seeded in 12-well plates (4×105 cells/well in 1 mL) and were cultured overnight at 37°C in a 5% CO2 atmosphere to allow cell adhesion before stimulation. The cells were pretreated for 2 h with increasing concentrations of auraptene (0, 0.2, 1, 5, and 20 μM), and then stimulated with 1 μg/mL of Aggregatibacter actinomycetemcomitans LPS for 24 h at 37°C in a 5% CO2 atmosphere. The cell-free supernatants were collected and stored at −20°C until used.
Commercial enzyme-linked immunosorbent assay (ELISA) kits (R&D Systems, Minneapolis, MN, USA) were used to quantify IL-6, IL-8, CCL-5, and MMP-2 concentrations in the samples according to the manufacturer's protocols. The absorbance at 450 nm was read using a microplate reader with the wavelength correction set at 550 nm. The rated sensitivities of the commercial ELISA kits were 9.3 pg/mL for IL-6, 31.2 pg/mL for IL-8, 15.6 pg/mL for CCL-5, and 47 pg/mL for MMP-2.
Gingival fibroblasts of human origin (HGF-1, ATCC CRL-2014; American Type Culture Collection, Manassas, VA, USA) were cultured in a 5% CO2 atmosphere at 37°C in the DMEM supplemented with 10% heat-inactivated FBS and 100 μg/mL of penicillin–streptomycin. Wound healing was assessed using Oris™ Pro Cell Migration Assay kits according to the manufacturer's protocol (Platypus Technologies, Madison, WI, USA). Briefly, 5×103 fibroblasts in DMEM-0.5% FBS (200 μL) were seeded in the wells of 96-well plates. The wells were previously coated with type I collagen and were equipped with in-place stoppers to create a migration area on the bottom of each well. The stoppers were removed after an overnight incubation, the medium was aspirated, and fresh DMEM-0.5% FBS with different concentrations of auraptene (0, 1, 2.5, and 5 μM) was added. After a 3-day incubation, the cells were washed twice with sterile PBS and were stained with 5 μM calcein acetoxymethyl ester. Cell migration was quantified using a fluorescence microplate reader (485 nm/528 nm: excitation/emission wavelengths) with a black bottom mask installed on the plate.
Following the treatment of the oral epithelial cells and fibroblasts with auraptene for 24 h, an MTT (3-[4, 5-diethylthiazol-2-yl]-2,5-diphenyltetrazolium bromide) assay was performed according to the manufacturer's protocol (Roche Diagnostics, Mannheim, Germany) to determine the effect of the compound on cell viability.
All experiments were carried out in triplicate, and the means±standard deviations were calculated. Data were analyzed using the Student's t-test with the level of significance set at P<.05.
Auraptene was chemically synthesized from commercially available umbelliferone (7-hydroxycoumarin) and geranyl bromide using an environmentally friendly, easy-to-handle, high yielding (98.6%) protocol without the need for a chromatographic step to purify the desired adduct. 16
We first examined the ability of auraptene to attenuate the LPS-induced inflammatory response of oral epithelial cells. The epithelial cells were pre-exposed for 2 h to different doses of auraptene before being stimulated for 24 h with A. actinomycetemcomitans LPS to determine the effect of auraptene on cytokine (IL-6) and chemokine (IL-8, CCL-5) secretion. The viability of epithelial cells was not affected by auraptene even at the highest concentration tested (20 μM=94%±7% viability), as determined by an MTT assay. LPS (1 μg/mL) markedly increased the secretion of IL-6 (2.2-fold) (Fig. 2A), IL-8 (6.5-fold) (Fig. 2B), and CCL5 (4-fold) (Fig. 2C). While 0.2 to 1 μM auraptene had no appreciable effect on IL-6 and IL-8 secretion, 5 to 20 μM had a significant (P<.05) inhibitory effect, reducing IL-6 and IL-8 levels to those observed with the untreated controls. Auraptene had a marked inhibitory effect on CCL-5 secretion, with the lowest dose tested (0.2 μM) reducing the level of CCL-5 to below that observed with the untreated controls (Fig. 2C).
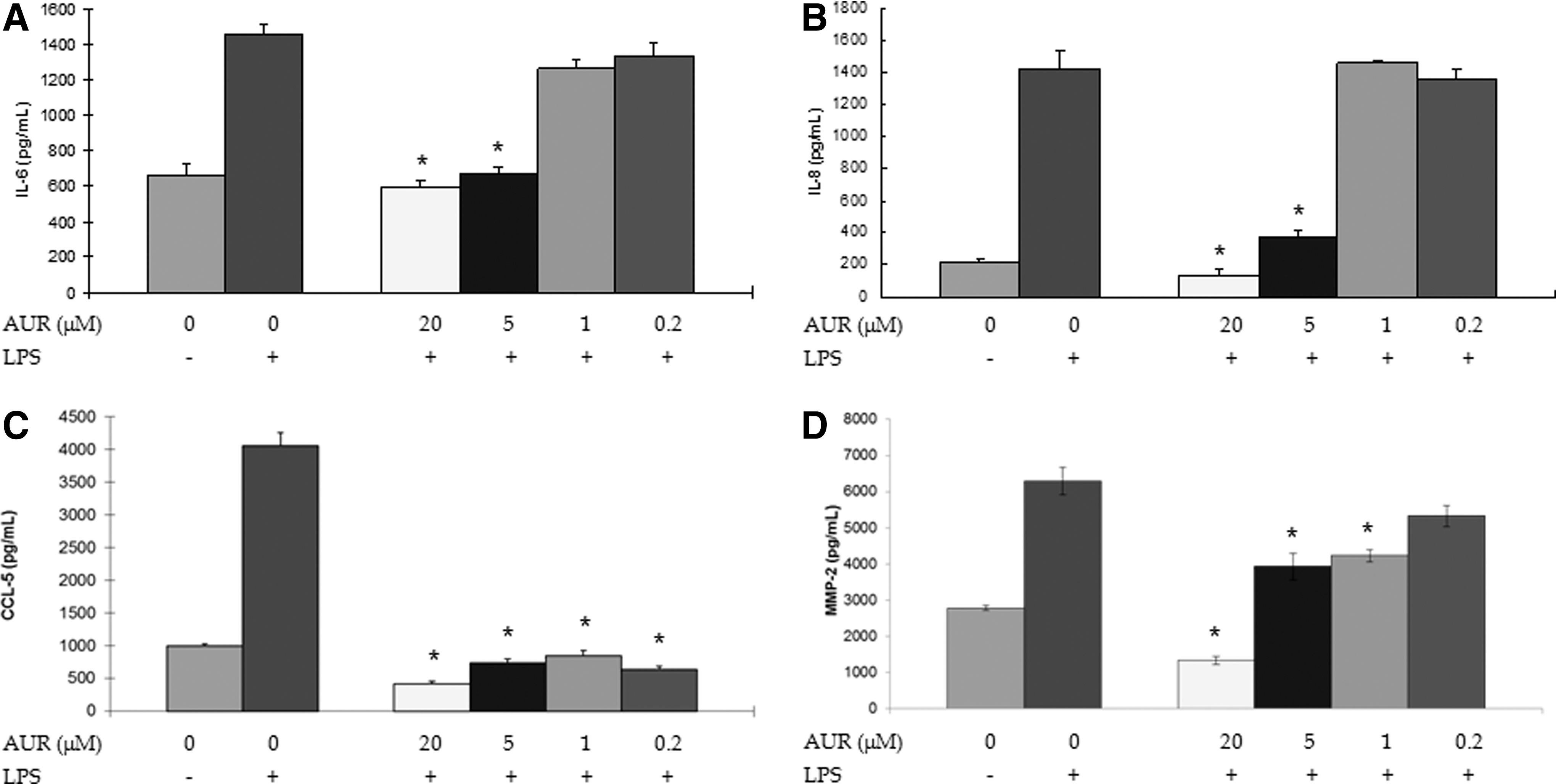
Effects of auraptene on interleukin (IL)-6
These results are of particular importance given that a pathway contributing to periodontal disease pathogenesis involves the secretion of high levels of proinflammatory cytokines and chemokines by host cells in periodontal tissues. Higher levels of IL-6, 17 IL-8, 18 and CCL-5 19 have been detected in the gingival crevicular fluid of patients with progressing periodontitis. IL-6 has been reported to induce osteoclast formation, which is involved in bone resorption. 20 The local inhibition of IL-6 secretion may thus have a positive effect on the inflammatory and bone destructive processes associated with periodontitis. IL-8 and CCL-5 are potent chemokines that direct the migration of polymorphonuclear leukocytes, monocytes, and macrophages to sites of infection. 21 The ability of auraptene to reduce IL-8 and CCL-5 secretion by oral epithelial cells may contribute to reducing the afflux of inflammatory cells to diseased sites.
We also investigated the ability of auraptene to reduce LPS-induced MMP-2 secretion by oral epithelial cells. As shown in Figure 2D, the decrease was dose dependent. At the highest concentration tested (20 μM), auraptene reduced the amount of MMP-2 to below that observed with the untreated controls. While MMPs contribute to normal oral tissue development and remodeling, uncontrolled expression of these enzymes by inflammatory and resident cells has been associated with periodontal tissue destruction. 22 In a previous study, Makela et al. 23 suggested that MMP-2 plays a role in tissue destruction in periodontitis since levels of this MMP increase in diseased sites and decrease following periodontal treatments. The ability of auraptene to reduce MMP-2 secretion may thus contribute to limiting the degradation of tissue components.
Wound healing is a complex process involving cell attachment to various components of the extracellular matrix as well as cell migration and proliferation. 24,25 During wound healing, fibroblasts play a critical role in forming healing (granulation) tissue by proliferating and migrating as well as remodeling the extracellular matrix by the de novo synthesis of matrix molecules. 24,25 Since fibroblasts are critical for the healing of gingival wounds, studying the effect of auraptene on this cell type may reveal whether this geranyloxycoumarin can contribute to the gingival wound healing process. As a matter of fact, wound closure was improved by 50% in the presence of 1 μM auraptene, while 2.5 and 5 μM auraptene improved wound closure by 100% (Fig. 3). To the best of our knowledge, this is the first time that auraptene has been shown to promote wound healing. We performed the migration assay using Oris Cell Migration Assay kit in which, the cells migrate onto a similar surface of migration created by a cell seeding stopper in each well along with the mask applied to the plate bottom that restricts visualization to the detection zones, allowing only cells that have migrated to be detected, thus minimizing error when compared with other methods that measure wound closure. This is an accurate and reproducible model to study wound healing by monitoring only migrated cells.
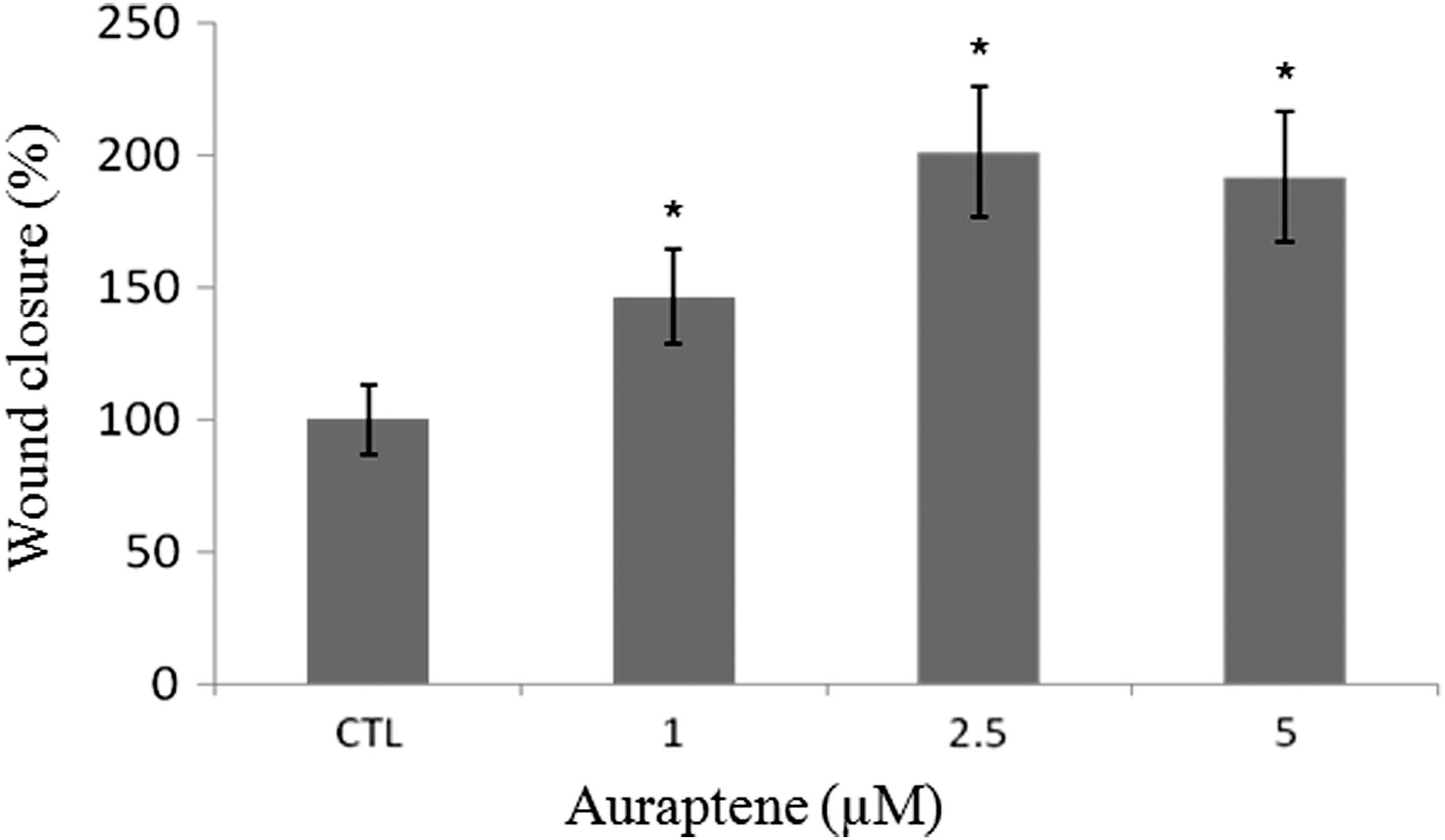
Effect of auraptene on wound closure using a gingival fibroblast model. A value of 100% was assigned to control cells not treated with auraptene. Oris Cell Migration Assay kits were used to measure cell migration. After a 3-day incubation, the fibroblasts were stained with calcein acetoxymethyl ester, and a fluorescence microplate reader was used to quantify migration. Data were analyzed using the Student's t-test (*P<.05 vs. untreated control).
Periodontal diseases are polymicrobial infections and are the most common chronic inflammatory disorders in adults. Periodontitis is induced by a specific group of Gram-negative anaerobic bacteria and is the main cause of tooth loss in adults. 1 Over the past two decades, natural compounds with synergistic antibacterial and anti-inflammatory properties have received considerable attention as potential new therapeutic agents for periodontitis. We recently reported that auraptene possesses beneficial antibacterial and anti-inflammatory properties since it can inhibit the growth of P. gingivalis, prevent the adhesion of this bacterial species to the oral mucosa, dose dependently reduce the secretion of cytokines (IL-8 and TNF-α) and MMP-8 and MMP-9 by LPS-stimulated macrophages, and inhibit MMP-9 activity. 14 In the present study, we further investigated the possibility of using auraptene to manage periodontal diseases. The results give additional evidence to the role of auraptene as a novel agent for the management of dental diseases. In particular, we showed that it also decreases the secretion of IL-6, IL-8, and CCL-5 by oral epithelial cells stimulated with LPS, and that it dose dependently inhibits MMP-2 secretion. We also showed that auraptene can facilitate wound healing by promoting cell migration. Given these novel properties as well as those previously reported by Marquis et al., 14 this natural product may be as a very effective weapon in the quest to manage and treat periodontal diseases. Since auraptene is effective on both etiologic components of periodontal diseases (periodontopathogenic bacteria and the host inflammatory response) and has the potential to promote wound closure, it shows promise as an adjunctive treatment for periodontitis.
Footnotes
Acknowledgments
We thank V. Murrah (University of North Carolina, Chapel Hill, NC, USA) for providing the GMSM-K epithelial cell line. This study was supported by an International Association for Dental Research-GlaxoSmithKline Innovation in Oral Care Award. F.E. and S.G. also wish to thank the “G. D'Annunzio” University of Chieti-Pescara for financial support.
Author Disclosure Statement
The authors have declared that there is no conflict of interests.