
Abstract
The role of saliva in maintaining oral health and homeostasis is based on its physicochemical properties and biological activities of its components, including salivary immunoglobulin A (IgA). Both salivary rates and immunological status of saliva are found to be compromised in smokers. The aim of this study was to investigate the acute time-dependent effect of smoking and black currant consumption on the salivary flow rate (SFR) and salivary IgA secretion rate (sIgA SR) in healthy smokers. SFR, sIgA levels in saliva, and sIgA SRs were determined in healthy smokers (n=8) at eight times of assessment within three consecutive interventions: at the baseline; 5, 30, and 60 min after smoking; 5, 30, and 60 min after black currant consumption (100 g), followed by smoking; and 5 min after black currant consumption. Smoking induced a significant delayed effect on SFR measured 60 min after smoking (P=.03), while black currant consumption preceding smoking prevented that effect. Salivary IgA concentrations and sIgA flow rates were not acutely influenced by smoking. Black currant consumption preceding smoking induced a significant decrease in sIgA concentrations 5 min after the intervention compared with the baseline (P=.046), with a further increasing trend, statistically significant, 60 min after the intervention (P=.025). Although smoking cessation is the most important strategy in the prevention of chronic diseases, the obtained results suggest that the influence of black currant consumption on negative effects of tobacco smoke on salivary flow and immunological status of saliva could partly reduce the smoking-associated risk on oral health.
Introduction
S
Oral tissues are constantly, and often simultaneously, exposed to harmful factors from the environment and diet, including pro-oxidants, carcinogens, and pathogenic microorganisms, and beneficial agents, including dietary bioactives, and the overall effect on human health relies greatly on their complex interactions. 6
A smoking habit has numerous negative effects on human health and is considered to be the leading modifiable risk factor for obstructive pulmonary disease, cardiovascular diseases, and lung cancer. 7 Effects of tobacco smoking on oral tissues involve numerous molecular mechanisms, resulting in decrease of salivary antioxidants and antioxidant enzymes, 8 negative effect on immunological status, induced secretion of proinflammatory cytokines and related mediators, increased activities of metalloproteinases, vasoconstrictor effects influencing oxygen and nutrient supplies, and compromised collagen synthesis. 9 These mechanisms are directly or indirectly associated with both systemic diseases and the diseases of the oral cavity.
Black currants have long been known to be a good source of vitamin C, but they also contain high levels of polyphenols, particularly flavonols and anthocyanins, 10 which contribute to the high antioxidant capacity. 11,12 Numerous studies have demonstrated beneficial effects of polyphenols and polyphenol-rich foods on oral health mediated by antimicrobial effects on oral pathogens, 13 interaction with dietary carcinogens, 14 activation of salivary antioxidant enzymes, 15 increase in salivary antioxidant status, 6 and increase in NO bioavailability after dietary nitrate intake. 16 Oral mucosal tissues, saliva, and oral microbiota are also rich sources of numerous enzymes involved in metabolism of polyphenols with high interindividual variation observed, influencing bioavailability and beneficial systemic effects. 17 However, data on the effects of polyphenol-rich food consumption on normal or disturbed salivary flow or the immunological status of saliva are lacking.
The aim of our study was to investigate the acute time-dependent effect of smoking and black currant consumption on the salivary flow rate (SFR) and salivary IgA secretion rate (IgA SR) in healthy smokers.
Materials and Methods
The human intervention study
Subjects
Eight apparently healthy volunteers were recruited for the study. All participants were smokers with a history of smoking longer than 10 years and more than 10 cigarettes a day during the last year. Exclusion criteria were as follows: chronic diseases, acute infections of the upper respiratory tract or symptoms related to oral cavity, use of medication, use of antioxidants or vitamin supplements, alcohol consumption (>20 g alcohol/day), intense physical activity (>5 h/week), and immunological disorders. Subjects with high consumption of polyphenol-rich food, estimated from the food frequency questionnaire, were also excluded from the study. All subjects declared themselves healthy and they had no evidence of chronic disease and none were taking any drugs. No subjects wore removable dentures or had other extensive dental work. Table 1 shows the characteristics of the participants enrolled in the study. The study protocol was approved by the Ethics Committee of the Public Hospital of Leskovac, Serbia. The study was conducted in February 2012 at the Centre of Research Excellence in Nutrition and Metabolism (CENM) of the Institute of Medical Research, University of Belgrade, in accordance with the revised Declaration of Helsinki. All participants provided written informed consent.
Participants were instructed not to consume any food containing anthocyanins 48 h before the study (berry fruits and juices, red wine, grapes, plums, apples, peaches, red grapefruit, red cabbage, red beans, red onion, pistachio), to avoid excessive exercise, and to have minimum 7 h of overnight sleep. Additionally, they were instructed not to smoke on the day of the study. All of the recruited participants fulfilled the study requirements.
Test product
Black currant berries, obtained from the commercial orchard in western Serbia, were washed and stored. Chemical characteristics of black currant berries used in the study are given in Table 2. A single intervention meal consisted of 100 g of black currants.
Values are mean±SD.
Study design
On the experimental day, after overnight fasting (minimum 12 h), participants attended the CENM at around 09:00 h in the morning. After an initial 20-min rest, the first saliva sample was taken (T0) and all subjects were given one cigarette to smoke (Intervention 1; I-1). Saliva samples were taken again 5, 30, and 60 min after smoking (T5, T30, and T60 of I-1). Subsequently, subjects were instructed to consume the test meal consisting of 100 g of black currant berries, wash the mouth with a small quantity of water afterward, and smoke another cigarette (Intervention 2; I-2). Saliva samples were taken 5, 30, and 60 min (T5, T30, and T60 of I-2) after smoking the second cigarette. After T60 of I-2, subjects were given only black currant berries (100 g) to consume, but without subsequent smoking (Intervention 3; I-3), and saliva samples were taken only 5 min after consumption (T5 of I-3). Flow diagram of the study design is given in Figure 1.

Flow chart of saliva assessment time points during each of three consecutive intervention periods. Subsequent interventions: I-1, smoking; I-2, black currant meal+smoking; and I-3, black currant meal. Color images available online at
Saliva sampling
Unstimulated total saliva was collected by the direct expectoration (spitting) method, as previously described by Miletic et al. 18 Briefly, at each time point, subjects were asked to allow spontaneous saliva flow during 2 min and afterward expectorate the whole saliva content from the mouth into the previously measured, sterile plastic tubes. Tubes were measured again and centrifuged for 5 min, at 2500×g at 4°C. Supernatants were aliquoted and immediately stored at −20°C.
Salivary flow determination
The SFR was calculated by dividing the sample volume (mL) with the time (min) taken to produce it. For the estimation of SFR, it was assumed that saliva density was 1.00 g/mL. 18
Salivary IgA determination
Salivary IgA concentrations (IgA conc) were measured by enzyme-linked immunosorbent assay (ELISA) as described previously, 19 with a slight modification. In detail, 96-well microtiter plates (MaxiSorp; NUNC, Roskilde, Denmark) were coated with goat anti-human IgA (Sigma-Aldrich, Steinheim, Germany) and incubated overnight at 4°C. The next morning, plates were washed thrice using TTBS (50 nM TBS containing 0.05% Tween 20) as washing buffer, subsequently blocked with 250 μL of 1% bovine serum albumin (BSA) in TTBS for 2 h at room temperature, and washed again thrice with TTBS. Saliva samples were thawed and diluted (1:1000) with 1% BSA in TTBS, 100 μL of each was added to the wells, and incubated for 1 h. Serial dilutions of IgA from colostrum (3.9–500 ng/mL) (Sigma-Aldrich) were used as calibrators. After 1 h, wells were washed again thrice and incubated with 100 μL of goat anti-human IgA antibody conjugated with alkaline phosphatase (Sigma-Aldrich) for 1 h. After washing, substrate solution (p-nitrophenyl phosphate) was added and the color intensity produced during a period of 30 min was measured by a microplate reader (Multiskan FC; Thermo Scientific, Vantaa, Finland) at 405 nm. All samples were assayed in triplicate with all samples from each subject analyzed on the same plate to avoid interassay variations. Saliva IgA concentrations were obtained by interpolation from the standard curve using regression analysis.
Salivary IgA SRs were obtained by multiplying values of salivary IgA concentrations and SFRs.
Statistical analyses
Normality of the obtained data was analyzed by the Shapiro–Wilk test. The repeated measures ANOVA was employed to analyze SFRs, salivary IgA concentrations, and salivary IgA SR changes over time with Bonferroni adjustment for multiple comparisons. Differences were considered significant at P<.05. Data are shown as mean±standard deviation (SD). Statistical analyses were performed with SPSS software (SPSS, Chicago, IL, USA).
Results
Data obtained for all investigated parameters, given as mean±SD, are presented in Table 3.
Values are mean±SD, significantly different at * P<.05, ** P<.01, and *** P<.001 by repeated measures ANOVA with Bonferroni adjustment for multiple comparisons.
Significantly different from the baseline (t=0).
Significantly different from T5 in Intervention-1.
Significantly different from T60 in Intervention-1.
Significantly different from T60 in Intervention-2.
Significantly different from T5 in Intervention-2.
SFR, salivary flow rate; sIgA SR, salivary IgA secretion rate.
Salivary flow rate
A repeated measure ANOVA with Greenhouse–Geisser correction showed that SFRs differed statistically significantly between eight time points [F (2.928, 20.494)=17.232, P<.0005]. Post hoc test using the Bonferroni correction elicited that smoking (I-1) induced a slight, but not significant, decrease in SFR measured at T5, 5 min after I-1 (P=.089). The effect persisted 30 min after smoking (T30 vs T5, P=1), but further reduction, statistically significant, compared with the baseline values (P=.03) was observed at T60 after I-1.
Combined intervention with black currants and subsequent smoking (I-2) induced a nonsignificant increase in SFR measured at T5 compared with the values obtained at the previous time point, T60 after I-1 (P=.074), reaching values similar to the baseline. Furthermore, changes in SFRs measured at T30 and T60 after I-2 were nonsignificantly different compared with the values at T5 after I-2.
The black currant meal alone (I-3) induced the increase in SFR measured at T5 after I-3 compared with the values obtained at all times of assessment, statistically significant at P<.01, for all time points.
Salivary IgA concentrations
Statistical analysis of salivary IgA concentration data showed a statistically significant difference at different times of assessment [F (2.78, 16.682)=5.69, P=.008]. Post hoc analysis showed that values obtained at three time points after smoking were not significantly different from the baseline values.
Values determined in saliva collected at T5 after the combined intervention with black currants and subsequent smoking (I-2) showed a decreasing trend without statistical significance compared with both the values obtained at T60 after I-1 and the baseline (P=.092 and P=.108, respectively). However, they were significantly different from the values obtained at T5 after I-1 (P=.019). Values obtained at T30 and T60 after I-2 were markedly higher compared with T5 after I-2, but without statistical significance.
Salivary IgA concentrations measured in saliva at T5 after the black currant meal alone (I-3) were not statistically different to the values obtained at any of the times points of assessment.
There is a strong negative correlation between sIgA concentrations and SFR observed regardless of the time (r=−0.507, P<.001).
Salivary IgA SR
Statistically significant differences between salivary IgA SR values at eight time points were shown by repeated measures ANOVA [F (1.894, 11.367)=5.759, P=.020], and the post hoc test with Bonferroni correction revealed that IgA SR was not influenced by smoking significantly at any time of assessment, although slight reduction at T60 after I-1 was observed (0.287).
Combined I-2 intervention resulted in a significant decrease at T5 compared with the baseline (P=.046), but the difference compared with both T5 and T60 after I-1 was not statistically significant. Salivary IgA SR values measured at T30 after I-2 showed an increasing trend reaching statistical significance at T60 compared with T5 after I-2 (P=.025) and reaching values similar to the baseline (P=1).
Salivary IgA SR measured 5 min after the black currant meal (I-3) declined nonsignificantly compared with the values recorded at T60 after I-2, but were still significantly higher compared with the values at T5 of I-2 (P=. 004).
Individual values obtained for SFRs, IgA concentrations in saliva, and salivary IgA SRs for three consecutive interventions at all investigated time points are given in Figure 2.
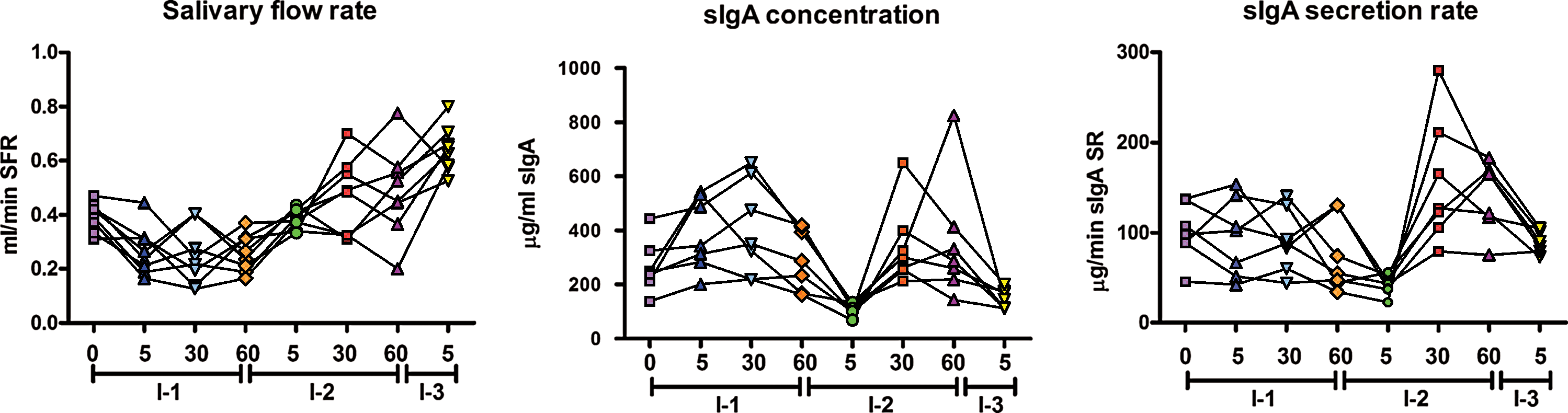
Salivary flow rate (SFR), concentration of salivary IgA (sIgA conc), and salivary IgA secretion rate (sIgA SR) in individual subjects. Color images available online at
The results obtained demonstrated delayed effect of smoking on salivary flow, with a significant decrease observed 1 h after the exposure, but without significant effects on concentration and SR of salivary IgA. Consecutive intervention revealed that black currant meal consumption following smoking attenuated the observed effects of smoking alone on salivary flow. At the same time, a short-term decrease in concentrations of salivary IgA with an increasing trend during the next hour was observed. Similar effects of combined intervention on SR of IgA were shown with a significant short-term decrease compared with the baseline values, followed by a significant increase during the next hour, resulting in IgA SR values similar to the values at the baseline. The consumption of the black currant meal alone induced a significant increase in SFR, but altered neither salivary IgA concentrations nor IgASFR, indicating that putative effects of polyphenols on the immunological status of saliva need further elucidation. However, the results obtained demonstrated the potential of a polyphenol-rich meal to attenuate unfavorable effects of different agents that could compromise the multiple roles of saliva in the homeostasis of the oral cavity by the decrease in SFR.
Discussion
Based on previously published data, the long-term effects of smoking on SFRs are unclear. Nagler 20 reported that SFR values in smokers were higher compared with nonsmokers, while in some studies SFRs were found to be similar in both populations. 21,22 Rad et al. 23 reported significantly lower SFRs and a significantly higher frequency of xerostomia symptoms in smokers compared with nonsmokers, in accordance with previous studies. 9,24 There are numerous factors found to influence salivary flow, including age, sex, health status, or medication used, that could induce the inconsistency in the obtained data. 25 However, there is a lack of kinetic data on acute effects of smoking on SFRs. In this study, we demonstrated the significant inhibitory effect of smoking on SFRs observed only after 1 h as a delayed effect. Immediate increasing effect of smoking on SFR 26 was explained with the stimulation of oral receptors and/or salivary glands rather than the effect of nicotine on parasympathetic synapses. However, Khan et al. 27 showed that orally applied nicotine solution in smokers induced hypersalivation only in the first few minutes. It is postulated that stimulation of salivary flow during smoking could induce the subsequent decrease as a second-phase response or could be a result of delayed vasoconstrictor effect of nicotine. Some authors also suggested that prolongation of the smoking habit and intense smoking could induce tolerance to the observed stimulatory effects of acute smoking or even degenerative changes in salivary glands, influencing salivation. 28 Drying of oral mucosa induced by hot smoke without compensatory response of salivary glands can additionally contribute to SFR reduction.
Results obtained after combined intervention (I-2) indicate that delayed SFR reduction induced by smoking could be prevented by black currant consumption preceding smoking. The observed effects could be attributed to either the acidic character of the intervention meal 29 and mechanical stimuli 30 or specific bioactive compounds. Nevertheless, it could be a good strategy for reduction of adverse effects of hyposalivation induced by smoking.
Black currant consumption without smoking (I-3) induced the most pronounced increase in SFR, postulating that the effect of the black currant meal on SFR, if it precedes smoking, could be partially compromised.
Salivary IgA SR in smokers is reported to be lower compared with nonsmokers accompanied by other effects on oral mucosa and immunity status, including decreased salivary IgG levels, reduced number of polymorphonuclear leucocytes, and decreased CD4+/CD8+ ratio, consequently making smokers more susceptible to periodontal diseases. 9 It is suggested that smoking influences both IgA-producing B-cells and secretory component-producing glandular cells. 31,32 Observed long-term effects are not supported by the direct acute effects of smoking on sIgA SR, which were found to be nonsignificant in our study. However, combined intervention with black currant berries preceding smoking showed surprising results. The decrease in sIgA SR observed 5 min after the intervention, which could be explained by the significant inducing effect of I-2 on SFR, is followed by marked increase in sIgA SR demonstrated 30 min after I-2, reaching statistical significance 60 min after I-2. Observed delayed effects on sIgA SR indicate different kinetics and mechanisms of action of combined intervention with black currants and smoking on salivation and sIgA. The precise mechanisms of bioactive-rich black currants on secretory IgA-producing machinery and putative interactions with effects of smoking are still not known, but it could be hypothesized that they include fine modulation of different components of mucosal immunity supported by previously shown effects of other polyphenol-rich food, in vitro and in animal models. 33,34 Additionally, hypothetic application of salivary IgA status after consumption of polyphenol-rich food as a screening tool for the effects of polyphenols, other dietary constituents, or their metabolites on gastrointestinal mucosal tissue needs additional scientific support, but should not be ignored.
The oral cavity is the entry point for all foods and drinks with the highest concentration of food constituents. It is also the first part of the digestive system that is considered to be one of the major sites of action of dietary antioxidants, including polyphenols. 35 Thus, the investigated biomarkers and the results obtained represent a contribution to the dossier of numerous effects of polyphenols in health promotion and the prevention of diseases.
Smoking has detrimental effects on human health mainly due to the constant exposure to the harmful effects of cigarette constituents. Lower consumption of fruits and vegetables in smokers compared with nonsmokers, shown in several cross-sectional studies, 36 further increases the risk.
In conclusion, although smoking cessation is the most important strategy in disease prevention, beneficial influence of black currant consumption on negative effects of tobacco exposure as a model of acute chemical stress could lower the health risks and needs further investigation.
Footnotes
Acknowledgment
This study was supported by a grant III 46013 from the Ministry of Education and Science of the Republic of Serbia.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.