
Abstract
This study evaluated the effectiveness and safety of Labisia pumila var alata (L. pumila) water extract for improving quality of life, cardiovascular and hormonal balance. A randomized, double-blind, placebo-controlled, parallel group, 16-week study in healthy pre- and postmenopausal women aged 40–60 years was conducted in Kelantan, Malaysia. The subjects were randomized to 400 mg propriety extract of L. pumila or placebo. A Women's Health Questionnaire was used to assess quality of life. Repeated-measures analysis of variance was used to evaluate the data. A total of 197 subjects (L. pumila: n=102 and placebo: n=95) were analyzed. Subjects in the herbal group showed improved memory/concentration, vasomotor symptoms, menstrual symptoms, and sleep problems by 8.3%, 15.9%, 11.8%, and 31.0%, respectively. The greatest improvement was observed for the question: “I get frightened or panic feelings for apparently no reason at all” with a 53% decrease as compared with placebo. Improvements were also seen in the cardiovascular parameters, and the safety profiles were normal. Postmenopausal women supplemented with L. pumila showed no changes in gynecological relevant hormones luteinizing hormone (LH), follicle-stimulating hormone (FSH), and 17β-Estradiol. Water extract of L. pumila was shown to be safe and effective for improving several parameters of quality of life and cardiovascular risks factors (total cholesterol [TC], low-density lipoprotein cholesterol [LDL-C]).
Introduction
L
In a rat study by Wahab et al., 3 a 60-day treatment with L. pumila at doses of 17.5 mg/kg body weight resembled the effects of Premarin (0.07 mg/kg body weight) as indicated by significant elevations of estrogen and testosterone levels and suppression of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) levels compared with the ovariectomized-control group. The androsteindione and DHEA-S levels were not altered. In in vitro assays, water extract of L. pumila showed antioxidant activity. 4 Animal studies using estrogen replacement therapy in ovariectomized Sprague–Dawley rats show lypolytic effect when treated with 17.5 mg/kg/day orally fed standardized aqueous extracts of L. pumila. The modulation of “postmenopausal adiposity” was observed through the initiation of the lipolysis process in adipose tissues characterized by the breakage in adipocytes membrane when treated with water extracts of L. pumila. 5 L. pumila exerted uterotrophic effects and regulated body weight gain by modulating secretion of leptin and resistin, and expression of the adipokines in adipose tissues. 6 A genotoxicity assessment of the herb was carried out using an in vivo rodent micronucleus assay where at doses of approximately 2000 mg/kg, body weight of L. pumila extract was demonstrated to have no mutagenicity. 7
Phytochemical studies of roots and leaves of L. pumila have shown the presence of alkenylresorcinols 8 and benzoquinons. 9 Phyto-chemical studies identified flavonoid, isoflavonoid, and phenolic compounds as bioactive ingredients in leaf extracts of the three varieties of L. pumila. 10,11 Flavonoids, mainly apigenin, kaempferol, rutin, and myricetin, were identified for L. pumila, along with phenolic contents such as gallic acid, pyrogallol, and caffeic acid. A randomized, double-blind, placebo-controlled study comparing three different doses (140, 280, and 560 mg/day) of the spray-dried water-soluble extract of L. pumila over a period of 6 months has proved to be safe, 12 including 280 mg extract of dosage recently published by Azidah et al., 2012. 13
The objectives of this study were to investigate the efficacy and safety of L. pumila water extract on the quality of life profile, cardiovascular risk factors, and hormonal profiles of healthy pre- and postmenopausal women.
Materials and Methods
Study design and setting
This was a 16-week randomized, double-blind, placebo-controlled study of healthy pre- and postmenopausal women in Universiti Sains Malaysia (USM) Hospital, Kubang Kerian, Malaysia from December 2009 till October 2010 and was conducted in accordance with the Guidelines for Good Clinical Practice (ICH-6) and the Declaration of Helsinki. The protocol was evaluated and approved by the Human Research and Ethics Committee for Clinical Studies of USM on 2 November 2009 (218.3).
Study participants
Healthy women aged 40–60 years who had undergone a hysterectomy or oophorectomy, bilateral tubal ligation or postmenopausal, no childbearing potential, or childbearing potential but on a medically approved method of birth control and had a negative urine pregnancy test were eligible for this study. The participants were stratified into premenopausal and postmenopausal (more than 1 year since last menstruation) status. Presence or absence of menopausal symptoms was not an eligibility criterion.
The exclusion criteria included having very irregular menses (>45 days cycle), abnormal pelvic ultrasound examination (e.g., endometrium thickness >5 mm), major uncontrolled psychiatric disorders, history of alcohol or drug abuse, renal or hepatic disorders, active peptic ulcer or bleeding disorder, unstable cardiac history, and use of oral natural herbal health products/dietary supplements within 1 month before randomization. Any other condition that in the Investigator's opinion might adversely affect the subject's ability to complete the study or its measures or which might pose significant risk to the subject was also a reason for exclusion.
Sample sizes were calculated using Power and Sample Size calculation software 14 for comparing two means, and the biggest sample size was for the variable estradiol level. Standard deviation of mean estradiol in the treatment group was taken as 28.8 15 and a detectable difference of 12 pM was decided after considering its clinical importance and feasibility of the study. The minimum required sample size was 91 and after considering the nonresponse rate of 10%, the sample size calculated for each group was 100.
Randomization and interventions
The allocation of random numbers was done by an independent quality control pharmacist at the manufacturer site using computer-generated tables. The study participants were informed and their consent was obtained. Baseline assessments included physical examination and assessment of quality of life profile using a validated Women's Health Questionnaires (WHQ). Blood samples (hormonal profile, cardiovascular risks profile, fasting blood sugar [FBS], and growth hormone) were drawn as indicated and sent to Gribbles Pathology (M). Pelvic scan, electrocardiogram, and the urine pregnancy test (if necessary) were performed at USM Hospital.
Participants were then dispensed the investigational product, returned to the clinic after week 8; any remaining investigational product or empty packaging was returned; and a new supply for 8 weeks was dispensed. Participants returned again after week 16. A follow up was performed at 2–3 weeks after completion of the study. Results from the trial were stored and analyzed at the School of Medical Sciences, USM, Kelantan.
Herbal product
The manufacturing process was performed according to good manufacturing practice standards, 16 by extracting 100 kg dried L. pumila var alata plant material with 1000 L of purified water at 100°C for 30 min followed by 4 h of cooling and was repeated for another cycle. The herbal extract was spray–dried using a spray tower having a tower inlet and outlet; the tower inlet temperature was 150°C, and tower outlet temperature was 80°C. The dried plant material to extract ratio was 10:1. Microbial limit test and heavy metal limit test were conducted for quality control.
High-performance liquid chromatography analysis of the extract
The extract was characterized by Agilent 1290 Infinity LC with photodiode array detection. The extract was sonicated in 50% methanol aqueous, whereas the reference compound was dissolved in methanol. Both solutions were filtered with 0.45 μm filter before injection. Five microliters sample was injected into the system. The mobile phase consisted of solvent A: 0.1% formic acid in water and solvent B: 0.1% formic acid in acetonitrile mixed according to a linear gradient of 10–95% solvent A and 5–90% solvent B. The flow rate and the detection wavelength were set at 0.3 mL/min and 260 nm, respectively. Several reference compounds were used to characterize the extract based on the fingerprint and reference compounds. The constituents of the L. pumila extract were identified by high-performance liquid chromatography by comparing the retention time (RT) with reference compounds. In order to identify the peaks, the extract was co-eluted with reference compounds, respectively. The peaks correspond to three compounds identified as Gallic acid, quercitrin, and kaempferol-3-rhamnoside at RT 2.309, 12.444, and 13.871 min, respectively.
Dosage and study protocol
The intervention group was instructed to take five capsules of 40 mg L. pumila water extract (BIOLP101) with 360 mg maltodextrin, and the placebo group was instructed to take five capsules of 400 mg maltodextrin, twice daily, morning and night for a total of 16 weeks. During intervention, the total intake of herbal product was 400 mg extract daily (10 capsules×40 mg extract). The dosage used in this trial was consistent with the amount consumed traditionally. Placebo medication corresponded to the active medication without the herbal extract. Participants who were found to be <75% compliant with test article usage at any two consecutive study visits were withdrawn.
Outcome measures and follow-ups
Quality of life assessed by the WHQ was the primary outcome. The Malay version of WHQ has been translated by MAPI Research Institute (27, rue de la Villette, 69003 Lyon, France who can be contacted to obtain translated questionnaire), and permission for its use was obtained from MAPI Research Trust, on behalf of Dr. Myra Hunter, the copyright holder of the WHQ. It consisted of 36 items assessing 9 dimensions/domains of physical and emotional health. The test reliability ranged from 0.98 to 0.78. 17 The secondary outcomes included safety profile, cardiovascular risk factors, and hormonal profile.
Statistical analyses
The study uses (modified) intention-to-treat analysis and last observation carried forward principle. Descriptive analysis and exploratory data analyses were conducted for all continuous and categorical-independent and -dependent/outcome variables. Univariate comparisons between L. pumila and placebo were conducted using independent t-tests for continuous variables and the chi-square (χ 2) test for categorical variables. Repeated-measures analysis of variance was used at 0.05 and 0.1 level of significance. Post hoc multiple comparisons with paired t-test Bonferroni correction analyses were used when indicated. Subsequent analysis of covariance was used only when the comparison groups or group-time interaction were significant. Statistical analyses were done using SPSS (PASW 18.0).
Results
A total of 202 subjects were randomized into L. pumila (103, 51%) and placebo (99, 49%) groups (Fig. 1). Subjects were omitted from analysis if they had no baseline data or missed a postbaseline evaluation at week 8 or 16. One and four subjects in L. pumila and placebo group, respectively, were excluded as they declined to participate and were noncompliant. A total of 197 subjects were analyzed (L. pumila, 102; placebo, 95). Table 1 shows the baseline demographic characteristics of L. pumila and placebo groups, and there was no significant difference between the two groups using independent t-test and χ 2 test.

Flowchart of the study.
Values are expressed as mean (SD), unless otherwise specified.
Independent t-test.
Chi-squared test.
SD, standard deviation.
Quality of life profile
Table 2 shows the quality of life for the total study population of L. pumila and placebo groups. There were no overall significant differences between the two groups in all the WHQ domain scores at baseline, week 8, and 16 with a few exceptions. Depressed Mood Domain showed a significant mean difference over time (P≤.001) with improvement in L. pumila (13.5%) compared with placebo (10.4%). Postmenopausal women in L. pumila group showed significant differences between baseline and week 8 (P=.018) and between baseline and week 16 (P=.006) (Fig. 2). Item 3 “I feel miserable and sad” showed improvement over time (P=.001) in both L. pumila and placebo groups (41.1% vs. 40.6%). Item 12 “I am more miserable than usual” showed improvement over time (P≤.001) in both groups (36.7% vs. 35.4%). When analyzed by menopausal status, postmenopausal women in L. pumila group showed significant improvement between baseline and week 16 (P=.020).
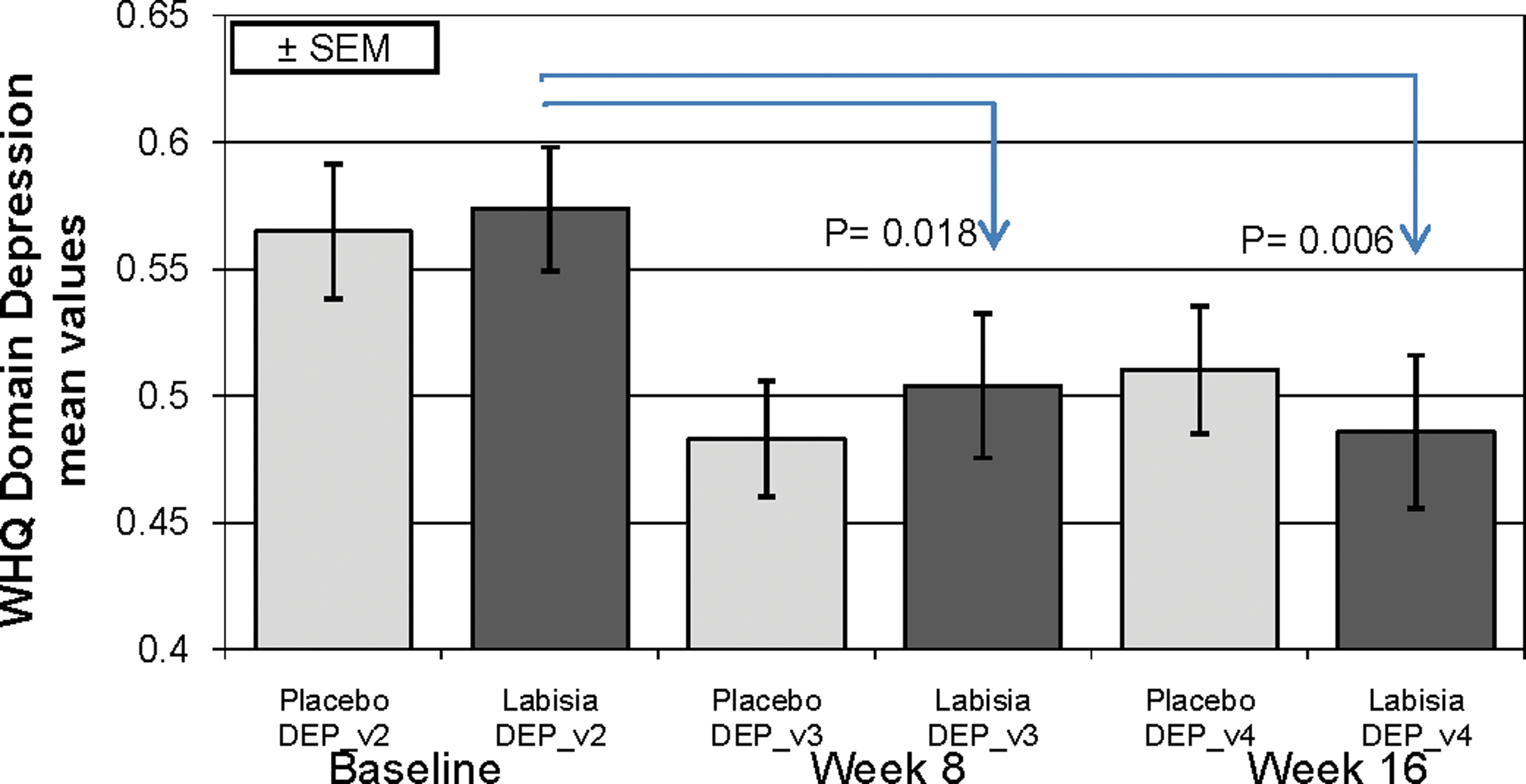
Mean (SEM) of Depressed Mood Domain from the Women's Health Questionnaire for postmenopausal women during 16 weeks of treatment with Labisia pumila (dark bars) and placebo (light bars). Color images available online at
Independent t-test.
Estimated marginal mean (95% confidence interval).
Group-time interaction by repeated-measures analysis of variance.
For sexual behavior domain, the No. of subjects analyzed were 157 (84 L. pumila and 73 placebo).
For menstrual symptoms, the No. of subjects analyzed were 97 (49 L. pumila and 48 placebo).
EMM, estimated marginal mean; IGF, insulin-like growth factor.
The Somatic Symptoms Domain showed an overall significant mean difference over time (P=.024) with improvement in both L. pumila and placebo group (11.8% vs. 12.5%). Item 15 “I feel more tired than usual” showed a significant difference between baseline and week 16 (P=.001) in placebo group but not within L. pumila or between groups.
Memory/Concentration Domain showed an overall significant mean difference over time (P=.030) with improvement in L. pumila (8.3%) and none in placebo group. Item 36 “My memory is poor” showed an improvement over time (P=.013) in L. pumila (8.4%) compared with placebo (4.9%).
Vasomotor Symptoms Domain showed an overall significant mean difference over time (P=.006) with less worsening in L. pumila (17.1%) compared with placebo (33.0%). Those with vasomotor symptoms showed better improvement in L. pumila (14.7%) than in placebo (7.9%) (P=.017).
Anxiety/Fears Domain showed an overall significant mean difference over time (P=.002) with better improvement in L. pumila (22.9%) than in placebo (15.8%). Item 2 “I get frightened or panic feelings for apparently no reason at all” showed a significant group×time interaction (P=.056) but after adjusting for its baseline value and menopausal status, L. pumila showed improvement by 53.0% compared with placebo (8.7%) (P=.088). Item 9 “I feel tense or ‘wound up’ ” showed improvement over time (P=.004) in placebo (25.8%) compared with L. pumila (18.5%).
Sexual Behavior Domain, however, showed improvement over time (P=.006) but less in L. pumila than placebo (7.4% vs. 19.3%). When analyzed by menopausal status, premenopausal women in the placebo group showed statistically significant improvements between baseline and week 8 (P=.022) and baseline and week 16 (P=.031).
Sleep Problems Domain showed greater improvement over time (P=.011) for L. pumila-treated subjects compared with placebo (38.1% vs. 7.1%). When analyzed by menopausal status, premenopausal women in L. pumila group exhibited the most significant improvement from baseline to week 16 (P=.003). Those with sleep problems showed improvement over time (P≤.001) in L. pumila by 33.6% compared with placebo (19.7%). Item 1 “I wake early and then sleep badly for the rest of the night” showed improvement over time (P=.001) in L. pumila by 23.9% compared with placebo (12.2%). When analyzed by menopausal status, postmenopausal women in L. pumila group showed more significant differences between baseline and week 8 (P=.024).
Menstrual Symptoms Domain showed greater improvement over time (P=.002) in L. pumila than in placebo (29.2% vs. 17.4%). Paired t with Bonferroni correction showed significant difference between baseline and week 8 [mean diff (95% CI)=0.12 (0.020, 0.215); P=.019] and between baseline and week 16 [mean diff (95% CI)=0.14 (0.061, 0.224); P=.001] in L. pumila group. Item 28 “My stomach feels bloated” showed improvement over time (P=.010) in L. pumila group by 46.6%, while placebo showed 0.0% improvement.
Hormonal profile
Table 2 shows the hormonal profile of L. pumila and placebo groups. Insulin-like growth factor showed a significant difference over time (P≤.001) with small increments in L. pumila compared with placebo (2.2% vs. 1.8%). Other parameters were not significant. Hormones FSH, LH, and 17β-Estradiol showed different values in pre- and postmenopausal women. Due to the increasing ovarian insufficiency during the transition period (peri-postmenopause), postmenopausal subjects had much higher concentrations of FSH, LH and lower 17β-Estradiol (Table 4). After 16 weeks of treatment, postmenopausal subjects in the L. pumila and placebo groups reported no significant changes in hormonal values compared with baseline.
Premenopausal women.
Postmenopausal women.
FSH, follicle-stimulating hormone; IQR, interquartile range; LH, luteinizing hormone.
Safety profile
Table 3 shows the safety profile of L. pumila and placebo groups. No safety parameters exhibited clinically important differences (>2×upper limit of normal range [ULN] or ≥3×ULN in alanine aminotransferase [ALT], alkaline phosphatase [ALP], or aspartate aminotransferase [AST]) at week 8 and 16 postintervention.
Independent t-test.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CRP, C-reactive protein; FBS, fasting blood sugar; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides.
Cardiovascular risk factors
Table 3 shows that the significant difference over time in L. pumila and placebo groups were total cholesterol (TC) (P=.031) with reductions of 2.2% (3.5% vs. 1.3%) and low-density lipoprotein cholesterol (LDL-C) (P=.005) with reductions of 1.7% (5.0% vs. 3.3%). There were no significant differences in high-density lipoprotein cholesterol (HDL-C), FBS, C-reactive protein, homocysteine, systolic blood pressure, diastolic blood pressure, and waist circumference. However, subjects with high levels of triglycerides (TG) and treated with L. pumila benefited by a decrease of 19.3% (23.8% vs. 4.5%).
Total bone mineral density
There were no statistical differences between groups over time though there appears to be an improving trend in total bone mineral density among postmenopausal women in the L. pumila group after 16 weeks. No changes were observed in the placebo group.
Adverse events
There were a total of three adverse events (AEs). Two AEs occurred in L. pumila group (cough, headache), and one AE occurred in placebo group (constipation). All AEs were reported as “unlikely” related to the medication.
Discussion
There were no significant differences between herbal and placebo groups within WHQ, but several significant findings within the WHQ domains were observed. The overall improvement in the Depressed Mood Domain, specifically among postmenopausal women who reported “feeling less miserable and sad,” may be due to higher estrogen levels, as periods of low estrogen are associated with mood disturbances. 18 However, in this study, estrogen-sensitive targets such as FSH, LH, and estradiol exhibited no change in concentration during L. pumila treatment among postmenopausal women, indicating no overall estrogenic or estrogen-like influences. Therefore, the improvement in depressive symptom during L. pumila intake may be via non-estrogenic pathways. Hormone therapy has been associated with improvements in mood changes, general well-being, and a decreased depression in postpartum, peri-, and postmenopausal women. 19,20 Estrogen receptors are distributed throughout the body and brain and closely linked to cognition and mood. Estrogens can, therefore, interact with central nervous system (CNS) monoaminergic pathways, for example, via neurotransmitters noradrenaline and serotonin. Antidepressant therapy for menopausal depressive symptoms management, including SSRIs (selective serotonin reuptake inhibitors), SNRIs (serotonin, norepinephrine, and reuptake inhibitors), or herbal products based on Hypericum perforatum (St. John's Wort), target these CNS pathways. 21,22 Based on the results of this study, it is possible that L. pumila contain nonestrogenic bioactive ingredients which interact with CNS pathways that are essential for depressive mood changes.
Several phenolic compounds, isoflavonoids, and flavonoids have been isolated from L. pumila. 11,23 –25 The total flavonoids and phenolic (anthocyanin) content for a similar aquoes extract of the same L. pumila var alata variety was determined to be 0.732 (0.05) mg/g fresh weight (FW) and 0.328 (0.07) mg/g FW respectively. 24 The flavonoids gallic acid, quercitrin, and kaempferol-3-rhamnoside were identified in the aquoes extract used in this study. There were many other unidentified peaks, and it would be worthwhile to identify them in the future. While less polar isoflavones and flavanones were identified from water extracts of L. pumila, the more polar flavanols of the water extract reportedly have stronger estrogenic effects. 26 Flavonoids are known to benefit the CNS, 27 and certain herbs such as Calluna vulgaris have been traditionally used as nerve calming remedies and found to possess quercetin as the active component. 28
Quercitrin, also known as quercetin 3-rhamnoside, is a derivative of quercetin. 29 The flavanoids in L. pumila may have been responsible for the overall significant mean difference over time in the Anxiety/Fears Domain, with a better improvement in L. pumila (22.9%) than in placebo (15.8%). In Item 2 of the WHQ scale, “I get frightened or panic feelings for apparently no reason at all” menopausal women on L. pumila fared better than placebo (53% vs. 8.7%). The findings are consistent with in vivo research in which aqueous extracts of L. pumila were able to reverse alterations arising from physical stress-induced depletion of neuromuscular coordination and scopolamine-induced memory deficit, thereby restoring homeostasis in vivo. 30
The L. pumila group improved in the Sleep Domain irrespective of pre- or postmenopausal status, or the severity of their sleeping problems. L. pumila appears to improve sleep, probably due to its high flavonoid content, 23 which are also known to be monoamine oxidase inhibitors, 31 –33 which tend to increase when estrogen levels drop 18 as is in the case of menopausal women. When monoamine oxidase increases, it breaks down neurotransmitters serotonin and dopamine, both of which are important mood stabilizing neurotransmitters. The decrease in their levels leads to fatigue and depression. 18 Although serotonin and dopamine decrease with age, the effect was not obvious in postmenopausal women by Item 2 in Anxiety/Fear Domain. The flavonoids in L. pumila may have inhibited the monoamine oxidase enzyme, thus elevating serotonin and dopamine levels in these women. 27,28
Sexual Behavior Domain, however, showed conflicting effects, where overall the placebo fared better than the Labisia group. There was an improvement in premenopausal women from baseline to week 8 and 16 in the placebo group. Both placebo and L. pumila groups of postmenopausal women improved over time in spite of aphrodisiac markers detected in L. pumila and Eurycoma longifolia. 34 Weak responses in this domain may be due to libido and sexual behavior mostly motivated by testosterone levels, which rose only slightly over the 16 week period in placebo and L. pumila group (0.67% vs. 3.0%). This is unlikely to trigger an aphrodisiac effect such that can be seen with herbs such as E. longifolia. 35 A longer supplementation period using L. pumila or a combination of L. pumila and E. longifolia may be able to modulate estrogenic and androgenic hormones optimally in women. This may lead to significant feelings of sexual well-being associated with hormonal balances. 36
The menstrual symptoms improved in the L. pumila group, especially for “My stomach feels bloated.” Bloating is one of the symptoms associated with menopause and is linked to the hormonal imbalances of estrogen, progesterone, and LH. 37 Since there were no significant changes in hormonal levels, the mechanism of action leading to this phenomenon is unknown. The herb may have reduced fluid retention, which is symptomatic of menopausal women. 38 Traditionally, the water decoction of the herb was used to get back into shape and slimming, 34 –36 which could be due to decreasing fluid retention.
There was an increasing trend in total bone mineral density in the postmenopausal L. pumila group. This is consistent with an animal study, where bone biomechanical testing in ovariectomized rats showed that the administration of 17.5 mg/kg L. pumila extract was as effective as estrogen replacement therapy (64.5 μg/kg/day conjugated equine estrogens) for improving bone strength and stiffness. 39,40 The bone marker for bone formation and ALP 41 significantly increased in the L. pumila group compared with the placebo group. Therefore, it is possible that L. pumila can be effective for herbal management against osteoporosis in postmenopausal women.
There were no significant differences in the safety parameters. Only 2 out of 102 subjects in the herbal group reported minor AEs not likely related to the herbal medication. L. pumila water extracts have established safety via sub-acute, teratogenicity, and micronucleus assays. 24,42 Significant differences over time in L. pumila and placebo groups were observed for TC, LDL-C, and subjects with high TG. Our data are in accordance with the recently published results from a 6-month randomized, placebo-controlled clinical trial of 63 postmenopausal Malay women using a 280 mg/day water extract of L. pumila, 20 in which 29 subjects receiving herbal medications had reduced cardiovascular risk during treatment, with a significant reduction in TG level compared with placebo.
No significant changes were observed in the gynecological relevant hormones observed during a 6-month treatment with L. pumila water extract in postmenopausal women, 13,20 which is similar to the herbal group in this study population. If L. pumila exhibits clinically relevant estrogen-like influences, it would be seen in the postmenopausal hormonal profiles. However, the hormonal profiles were comparable to placebo. In the premenopausal women, though the mean at baseline for 17β-Estradiol was similar for placebo and treatment groups, 17β-Estradiol levels increased by 29.4% in the treatment group compared with 9.3% in placebo. An interpretation of this observation is difficult, as pre (peri)menopausal women still menstruate, reflecting various underlying hormonal profiles; however, an improving trend in pre (peri)menopausal women in whom hormone fluctuations (irregular menstruation cycles, menopausal transition) are more prevalent than postmenopausal women was observed. 43 This finding justifies traditional use of this herb in treating postpartum women who have a drop in estrogen levels after birth. The herb appears to behave similar to an adaptogen, 44 where in premenopausal women, hormonal levels of 17β-Estradiol have improving trends; whereas in postmenopausal women, the phytoestrogenic-like behavioral improvement is experienced without alterations in hormone levels. This is consistent with the in vitro investigation of L. pumila in displacing 17β-Estradiol binding to antibodies raised against 17β-Estradiol. 8
In conclusion, water extract of L. pumila (BIOLP101) at a daily dose of 400 mg for 4 months was shown to be efficacious in several quality of life parameters as well as improving cardiovascular risks factor (TC, LDL-C) in pre- and postmenopausal women. The extract was well tolerated, and safe. L. pumila may also be beneficial in older women with a higher risk of cardiovascular disease postmenopause. It can be considered a therapy against cardiovascular disease and for improving overall health.
Footnotes
Acknowledgment
The authors would like to thank the phyto-pharmaceutical company Biotropics Malaysia Berhad, Kuala Lumpur, Malaysia for financially supporting the clinical trial.
Author Disclosure Statement
No competing financial interests exist.