
Abstract
Laminaria japonica—a widely used ingredient in seaweed kimchi—and lactic acid bacteria (LAB)—a main component of traditional fermented Korean food—may alter human intestinal microbiota composition and have a positive effect on various digestive problems. However, few clinical trials have investigated the potential benefits of L. japonica when combined with LAB for human intestinal microbiota. Therefore, this study was designed to evaluate the effects of L. japonica and representative LAB on the human intestine. Forty participants with no known digestive diseases were randomly assigned to one of the two combination groups: (1) L. japonica with LAB and (2) L. japonica with placebo LAB. The study agents were administered for 4 weeks with a 2-week follow-up period. The primary outcome measure was the number of each of the seven LAB species in the human intestine, and the secondary outcome measures included the Korean version of the Gastrointestinal Symptom Rating Scale, the World Health Organization Quality of Life, and bowel functions. The primary outcome was evaluated before and after administration of the study agents (0 and 4 weeks), and the secondary outcomes were evaluated at 0, 4, and 6 weeks. Four of the seven LAB species were found to be significantly increased in the L. japonica with the LAB group and five species were significantly different from those of the placebo group. The secondary outcome measures did not change significantly. In conclusion, L. japonica with LAB facilitated the proliferation of beneficial human intestinal microbiota. (Trial number:
Introduction
K
Lactic acid bacteria (LAB) are primarily responsible for the fermentation of kimchi and more than 108 colony-forming units of LAB are involved. 6 During the early stages of kimchi fermentation, the LAB profile is comparatively diverse; however, in the later stages, the LAB profile becomes simpler and consists mostly of Lactobacillus plantarum. 7 LAB have been the focus of international research for their potentially beneficial roles in stabilizing the gut microflora. 8 LAB are also effective for preventing various digestive problems such as colon cancer 9 and chronic diarrhea. 10
Recent research on L. japonica and LAB has shown that L. japonica with LAB possesses a high antioxidant activity and protects against hepatic damage, obesity, hypertension, stress, insomnia, and alcoholic liver damage. 11,12 However, although the beneficial effects of L. japonica with LAB are well known, few clinical trials have investigated its effect in human intestine.
This study aimed to evaluate the effect of L. japonica with LAB as representative compounds of seaweed kimchi. We examined the microbial communities in the healthy human intestine before and after the administration of L. japonica with LAB. We also compared the number of intestinal microbiota between the two groups (L. japonica with LAB and L. japonica with the placebo LAB group). Additionally, questionnaires on gastrointestinal symptoms and quality of life were used to investigate the combined effect of L. japonica with LAB.
Materials and Methods
Subjects and study design
Forty-three volunteers with no history of disease, aged 18–75 years were recruited from the local community through bulletin board advertising, brochures, and banners. Three subjects failed in the screening test and the remaining 40 participants were enrolled in the study. The current study was reviewed by the Institutional Review Board and Ethics Committee of the Kyung Hee University Hospital at Gangdong (KHNMC-OH-IRB 2012-005). The trial followed the standards of the International Committee on Harmonization of Good Clinical Practice and the revised version of the Declaration of Helsinki. All participants were asked to fill out informed consent forms, and they were allowed adequate time to decide whether they would participate in the trial before signing the consent.
The study was performed as a placebo-controlled and double-blinded trial with 40 participants randomly allocated to two groups: (1) L. japonica with Duolac7S (DUO) and (2) L. japonica with placebo DUO. Participants were required to complete a 4-week treatment period (weeks 0–4) and a 2-week follow-up period (weeks 4–6). The flowchart of the entire trial is shown in Figure 1.

Flow chart of the trial. LJE, Laminaria japonica extract; DUO, Duolac7S; DUO-P, Placebo of Duolac7S.
All eligible participants were free of diseases and clinical symptoms, according to the Korean version of Gastrointestinal Symptom Rating Scale (KGSRS) with scores of <3 points and no history of abdominal surgery related to the digestive system. Subjects who took over-the-counter medications that affected gastrointestinal motility or antibiotics, herbal medicine, or probiotics 2 weeks before the start of the trial were excluded. Pregnant women or women who planned to become pregnant during the trial period were also excluded. The study participants were asked not to take any medication that could affect the gastrointestinal tract during the trial, and if medications were taken, the drug name, usage, and duration were recorded on the case report form.
An independent statistician was responsible for the assignment of random numbers that were generated through a creation program. An opaque sealed envelope containing the table of random serial numbers was kept in a locked cabinet. The participants, investigator, and clinical research coordinator (CRC) were blinded to the randomization, and the blinding procedure was monitored by an authorized clinical research associate.
All participants were asked to report any adverse events to the principal investigator or CRC during the entire trial. The values for serum complete blood count, blood urea nitrogen, creatinine, aspartate aminotransferase, alanine aminotransferase, gamma-glutamyltransferase levels, and erythrocyte sedimentation rate were assessed to confirm the safety of the study agents after the treatment period. The safety test analyses were performed at an accredited laboratory, and any adverse events and safety issues were documented on the case report form.
Interventions
The agents used in this trial were water-extracted L. japonica (LJE) and DUO. The LJE tablet was an oval-shaped, green tablet comprising 625 mg of LJE and 20 mg of diluting agent. Hanpoong Pharm and Foods Co., Ltd. (Jeonju, Republic of Korea) was in charge of LJE manufacturing according to the Korea Food Manufacturing Practice standards. LJE was packaged in a white plastic bottle, and one bottle of LJE was distributed to each participant.
DUO is a probiotic mixture composed of seven LAB: three strains of Bifidobacterium (B. brevis, B. lactis, and B. longum), three strains of Lactobacillus (L. acidophilus, L. plantarum, and L. rhamnosus), and one strain of Streptococcus (S. thermophilus). DUO has been approved by the Korean Food and Drug Administration for improving the balance of the intestinal microbiota. The DUO was packaged in a white ellipse capsule containing 5×109 bacteria (7×108 viable cells/strain). Placebo DUO was composed of cornstarch and nearly identical to the study agent in color, shape, odor, and taste. DUO and placebo DUO were produced by Cell Biotech Co., Ltd. (Gimpo, Korea). Participants took two LJE tablets and one DUO or placebo capsule twice daily (30 min after the morning and the evening meal) for 28 days. The dosage of LJE was determined based on preliminary experimental research in mice showing that the optimal results were achieved with a dose of 100–300 mg of LJE (data not shown). Considering the human metabolic rate (about 10% of mouse) and mean adult weight (50 kg), we set the dosage of LJE as 1.25 g per day (625 mg/capsule). Compliance was determined by counting the remaining LJE tablets or DUO capsules, and all participants reached the required compliance rate of 80%.
Primary outcome
The primary outcome was the number of each of the above-mentioned seven LAB species in the subject's intestine. Each participant was asked to submit a 5-g fecal sample at baseline (week 0) and at the end of the administration period (week 4). The samples were stored at −70°C until analysis. The qualified laboratory of Cell Biotech Co., Ltd. analyzed the fecal samples for the presence and the number of the seven LAB species.
Secondary outcomes
The severity of gastrointestinal symptoms was assessed by the KGSRS. KGSRS included 15 questions to evaluate various digestive problems, including abdominal pain, heartburn, indigestion, diarrhea, and constipation 13 and each item was assessed on a five-point Likert scale, with a higher score indicating a severe degree of symptoms. KGSRS has been regarded as reliable and validated by a previous study. 14
The quality of life was evaluated by the World Health Organization Quality of Life Brief Assessment (WHOQOL-BREF), which consists of four categories and 26 questions that yield a multidimensional profile of scores related to the quality of life such as physical function, psychological function, social relationships, and environmental function. The Korean version of the WHOQOL-BREF demonstrated consistency, validity, and reliability in a previous study. 15
Last, stool frequency and consistency by the Bristol stool scale 16 was evaluated. Ease of passage, as defined by the adjectival scale (from manual disimpaction to incontinence) was also assessed. All secondary outcomes were investigated at baseline (week 0), the end of the administration period (week 4), and the end of the follow-up period (week 6).
Statistical analysis
The sample size was calculated considering that the current trial was a pilot study. According to similar previous research, 17 the sample size in this trial was set as 20 in each group. The withdrawal rate was assumed to be 25% and the statistical power was 80% with statistical significance of P value<.05.
All data were analyzed by an independent statistician using SPSS version 16.0 (SPSS, Inc., Chicago, IL, USA). A comparison of the baseline characteristics between the two groups was made using an independent t-test for continuous variables and the Fisher's exact test for categorical variables. All continuous variables were presented as mean±SEM and categorical variables were presented as percentages. The primary outcome, the comparison of the number of LAB between the two groups at 4 weeks, was analyzed using an independent t-test. A paired t-test was used for comparison of the number of each LAB species before (week 0) and after administration of the study agents (week 4).
KGSRS, WHOQOL-BREF, or bowel function scores were compared between the two groups using an independent t-test. Comparison of subgroup scores on the KGSRS or WHOQOL-BREF was conducted using the Wilcoxon signed-rank test. A P value of<.05 was considered statistically significant.
Results
General demographic characteristics
Between May 2012 and November 2012, 43 patients were screened; of these, 3 participants failed to meet the inclusion criteria (Fig. 1). No subject dropped out and all subjects completed the study, possibly because of the short study duration. Baseline demographic characteristics, the KGSRS scores, and bowel function scores were balanced between the two groups at the beginning of the study as shown in Table 1. There were also no significant differences in WHOQOL-BREF scores except for the mind domain (P=.042).
Data are presented as mean±SD values or percentages. Baseline values were analyzed by the Fisher's exact test for categorical variables and the independent t-test for continuous variables.
Used a scale of 1–7: 1, watery stool; 7, hard, lumpy stool.
Used a scale of 1–7: 1, fecal incontinence; 7, manual disimpaction.
KGSRS, Korean version of gastrointestinal symptom rating scale; LJE, Laminaria japonica extract; DUO, Duolac7S; DUO-P, Placebo of Duolac7S; WHOQOL-BREF, The World Health Organization Quality of Life Brief Assessment.
Intestinal microbiota
After completing the treatment, there were statistically significant changes in the number of intestinal microbiota in the paticipants' feces. The numbers of four types of intestinal microbiota (B. brevis, B. lactis, L. plantarum, and L. rhamnosus) showed a statistically significant increase after administration of L. japonica with DUO, whereas no significant change in the number of any intestinal microbiota was noted in the L. japonica with the placebo DUO group (Fig. 2). There was a significant difference in the numbers of five intestinal microbiota (B. brevis, B. lactis, B. longum, L. plantarum, and L. rhamnosus) between the L. japonica with DUO and L. japonica with placebo DUO groups after administration (week 4) as shown in Figure 2.
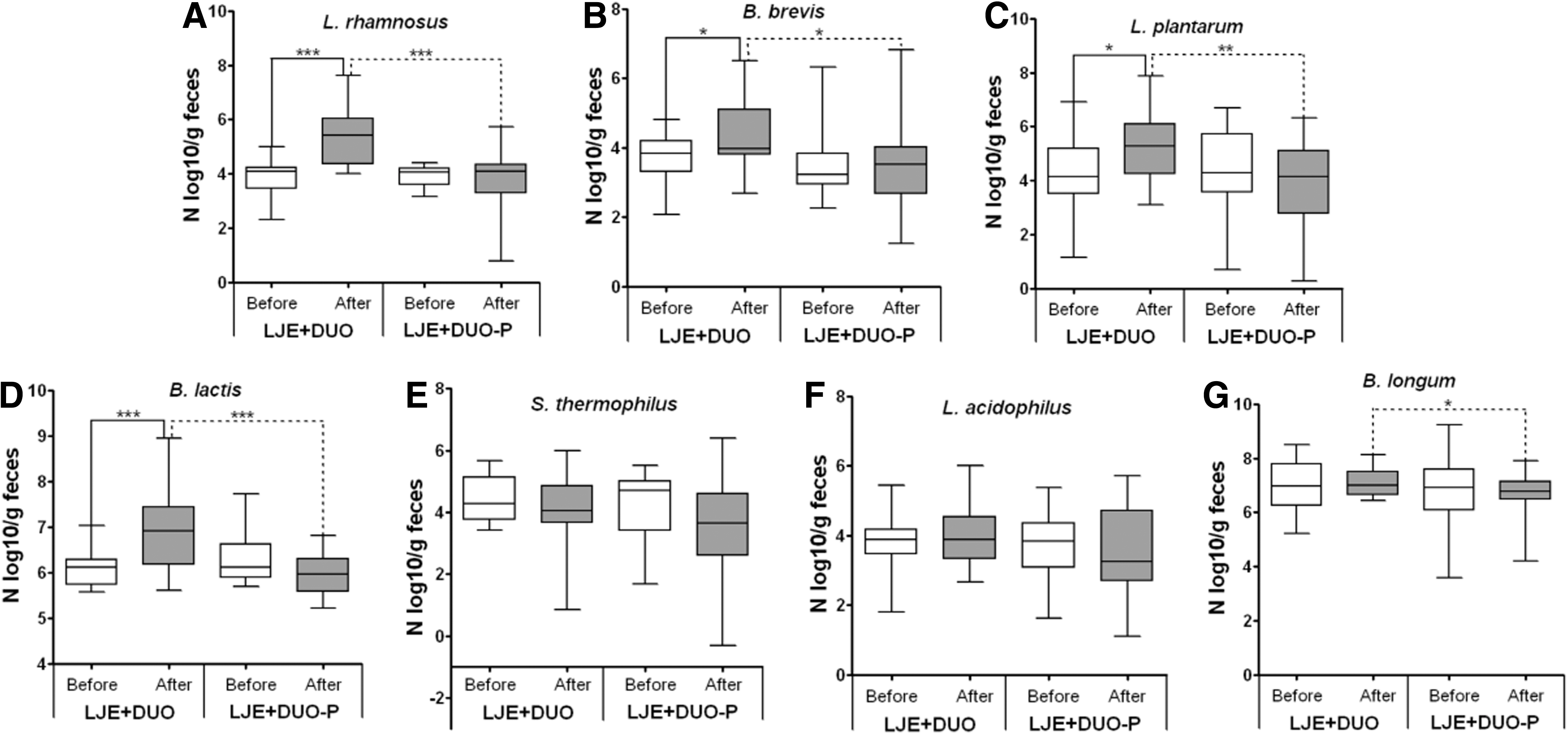
Effect of 4-week LJE with DUO on intestinal microbiota compared with LJE with DUO-P in subjects who have no organic disease.
KGSRS, WHOQOL-BREF, and bowel function scores
There were no statistically significant changes in the KGSRS, WHOQOL-BREF, and bowel function scores (stool frequency, consistency, and ease of passage) after the intake of study agents in either group. Furthermore, no difference in the KGSRS, WHOQOL-BREF, and bowel function scores was noted between the two groups at week 4.
Adverse events and safety
No major adverse events were noted after treatment with the study agents. Liver and kidney functions were evaluated at week 4, and no safety issues were found in either group.
Discussion
In the current study, we examined the effect of L. japonica, a main ingredient of kimchi, with DUO, a probiotic containing kimchi LAB, on human intestinal microbiota. Administration of L. japonica with DUO caused an increase in the number of four types of intestinal microbiota (B. brevis, B. lactis, L. plantarum, and L. rhamnosus), and that of five microbiota (B. brevis, B. lactis, B. longum, L. plantarum, and L. rhamnosus) was significantly different compared with the placebo group. In the placebo group, there were no significant changes in the number of intestinal microbiota. Moreover, there were no significant changes in KGSRS, quality of life, or bowel function after the treatment in either group.
Normal intestinal microflora consists of >1000 bacterial species and their number is the highest in the terminal ileum and colon. 18 In healthy people, there is a good balance between beneficial and pathogenic bacteria in the intestines. Fecal microbial changes associated with aging include reduced number of beneficial bacteria such as Bifidobacterium 19 and instability of intestinal microbiota, which may play a role in the pathophysiology of irritable bowel syndrome. 20 Other studies have reported that the lack of Bifidobacteria and Lactobacilli could cause functional abdominal pain and diarrhea. 21,22 Because the intestinal microbiota plays a significant role in the intestinal metabolism and natural defense of the host, maintaining and increasing the intestinal microbiota for improved barrier function of the mucosa and resistance to invasion and proliferation of pathogenic agents are vital. 23
Seaweed kimchi is a popular traditional fermented Korean dish made of vegetables and seaweeds such as L. japonica, with diverse seasonings. 24 Kimchi has been recognized as a healthy functional food with an ability to regulate digestive problems, and has gained popularity after being mentioned in the magazine “Health”. 25 East Asian individuals, who consume a greater quantity of seaweed than those in the West, have been reported to experience fewer constipation episodes, and the rates of cancer and obesity are also comparatively lower. 4 As a fermented food, kimchi contains a number of LAB, in which L. plantarum plays a crucial role at the final stage of fermentation. 26 LAB in kimchi are important for taste and quality and play a potentially beneficial role as probiotics, which are viable microorganisms that improve the host's intestinal microbial balance. 27 DUO, containing a large number of LAB such as L. plantarum, has been a popular dietary supplement in Korea because of its beneficial effects on digestive symptoms and easy accessibility without a prescription. 20 Recently, L. japonica with LAB has been the focus of clinical research for its beneficial profiles, including gamma-aminobutyric acid and taurine, which prevent metabolic syndrome and mental disorders. 11,12 This trial is the first study to investigate the change in the number of intestinal microbiota after administration of L. japonica with LAB. We tried to standardize and formulate each study agent (L. japonica and LAB), which made it possible to conduct a patient, assessor-blind trial.
Kimchi has a variety of ingredients and contains a great variety of LAB during fermentation. The LAB species in kimchi have not been fully identified and some of them cannot be cultured. Therefore, we designed a study to compare the two main components of kimchi (L. japonica and DUO). L. japonica has been reported to have anti-inflammatory, anticoagulant, antiangiogenic and antiadhesive effects, 3 and it is also the most effective for improving colitis symptoms in mice among eight species of representative seaweeds in our previous experimental research (data not shown). Although DUO does not contain most kinds of kimchi LAB, it includes species of Lactobacillus and Streptococcus genera that are mainly involved in kimchi fermentation.
In our previous clinical study on the effect of a herbal prescription combined with DUO on intestinal microbiota in subjects without any organic disease, we observed synergistic effects on the numbers of several beneficial LAB (data not shown). In addition, DUO significantly increased the number of several beneficial LAB, and the placebo group showed a slight decrease in the number of beneficial LAB in feces. Considering that temporal instability in the fraction of active microbiota is related to functional disease and fluctuating digestive symptoms, 28 and that healthy people tend to show a decrease in the number of intestinal Bifidobacteria with advancing age, 29 L. japonica might potentially be used to prevent the decreases in intestinal bacterial numbers. Because L. japonica with real DUO was associated with a significant increase in the number of intestinal microbiota compared with the placebo group, there might be a synergistic effect of L. japonica and DUO. This finding suggests that L. japonica might serve as a prebiotic supporting the proliferation of beneficial microbacteria in the human intestine.
There were no significant changes between the two groups in KGSRS, quality of life, and bowel function. Because L. japonica, which contains a lot of fiber, has been widely reported to prevent constipation, 2 it is possible that it might also cause diarrhea or abdominal pain. We therefore investigated secondary variables associated with digestive symptoms and quality of life to confirm the safety profile of L. japonica, and no factors that might negatively affect the quality of life or aggravate digestive problems were detected. The statistical difference (P=.042) at baseline in the mind domain of WHOQOL-BREF is a negligible level without clinical meaning.
We could not use placebo L. japonica, because it is almost impossible to make placebos of a natural product (L. japonica in this case) with the same odor, taste, and color. Thus, the most feasible design reflecting real kimchi for the general Korean population was considered to be a two-group (L. japonica with LAB and L. japonica with placebo LAB) comparison parallel design.
Our study has some limitations. The study agents in this trial did not fully reflect seaweed kimchi consumed in everyday life. Furthermore, more research will be needed to identify new kimchi LAB and their role during fermentation. This study has a small sample size, which might weaken the significance of the beneficial effects of L. japonica with LAB. Further studies, including the mechanisms of action and with large sample sizes, are needed.
In conclusion, this study showed that L. japonica with LAB might have a beneficial effect on human intestinal microbiota by enhancing the proliferation of beneficial bacteria. DUO as a LAB played a key role in increasing the number of intestinal microbiota and L. japonica might also help prevent the reduction in the number of beneficial intestinal microbiota. The synergistic effect of L. japonica with LAB might improve the intestinal environment and overall health by alleviating digestive symptoms.
Footnotes
Acknowledgments
This research was supported by the Globalization of Korean Food R&D Program and was funded by the Ministry of Food, Agriculture, Forestry and Fisheries, Republic of Korea (Assignment number: 911029-1).
Author Disclosure Statement
No competing financial interests exist.