
Abstract
This exploratory study was designed to assess the effectiveness of a lignan-rich extract of flaxseed hulls (LinumLife EXTRA®) in alleviating symptoms in subjects with benign prostatic hyperplasia (BPH) compared with placebo. Two dosages of extract were compared against placebo in a double-blinded, randomized, parallel, multicenter study. Newly diagnosed cases of BPH in patients aged 45–75 years with an American Urological Association Symptom Index (AUASI) score of ≥13 were included. Study treatment consisted of 500 or 1000 mg of extract containing 100 mg (low-dose active [LDA] group, n=26) or 200 mg (high-dose active [HDA] group, n=26) of secoisolariciresinol diglucoside (SDG), respectively. The placebo (P) group (n=28) received matching maltodextrin capsules. Sixty subjects (LDA [n=19], HDA [n=20], and P [n=21]) completed the study as per the protocol requirements. Change in the AUASI score within a period of 8 weeks, from baseline to end of treatment, was assessed. Significant improvement of obstructive symptoms and management of irritable BPH symptoms was achieved in all groups after treatment. Due to a strong placebo effect, there was no statistical difference between the groups that were treated with flaxseed hull extract as compared with the placebo group. Treatment with flaxseed hull extract did not lead to adverse effects compared with placebo. Supplementation with flaxseed hull extract was found to be safe and well-tolerated and may have improved the quality of life of individuals with BPH. The significant placebo effect as well as the number of subjects per treatment group and the relative short duration of the study may explain the lack of statistical significance between groups.
Introduction
T
The current pharmacotherapy of BPH utilizes drugs like alpha adrenergic blockers and 5α-reductase inhibitors. 5 –7 Evidence from clinical studies as well as clinical practice have proven the efficacy of these agents in providing symptomatic benefit. 5 –7 However, a plethora of side effects is associated with the use of these drugs. 6,8
Transurethral resection of the prostate (TURP) is currently the gold-standard surgical management of BPH and is one of the most frequently performed surgeries in men above the age of 65 years, but it is also associated with a multitude of postoperative systemic complications commonly referred to as the TURP syndrome. 9
Along with the improvements in the surgical and pharmacotherapeutic management of the condition, a proportional rise has also been witnessed in the overall cost incurred during therapy, which is a significant economic burden on the elderly population. 10 This has resulted in the exploration of safer and more economical treatments, like the use of secoisolariciresinol diglucoside (SDG) for the longer term management of BPH. SDG is the predominant lignan in flaxseed and flaxseed hulls. SDG as well as the mammalian lignans enterodiol and enterolactone, metabolites that are formed upon gastrointestinal conversion of SDG, are the predominant bioactives responsible for a number of beneficial effects, including the improvement of cardiovascular health, chemoprevention, and metabolic syndrome. 11,12
Animal and human studies have demonstrated that flaxseed lignan extract has the potential to improve symptoms in subjects with BPH. 13 The current randomized, double-blind, placebo-controlled study was planned to investigate the efficacy and safety of two dosages (low and high) of a lignan-rich flaxseed extract, LinumLife EXTRA®, for the improvement of BPH.
Subjects and Methods
Design
This was a randomized, double-blind, placebo-controlled study in BPH subjects conducted at nine study sites located in Mumbai, Pune, and Nasik in India, over a period of 8 weeks. Randomization and blinding were performed to ensure minimization of bias and robustness of design.
The subjects were randomized across three groups (low-dose SDG, high-dose SDG, and placebo) in a 1:1:1 ratio. Block randomization was employed for assigning treatment codes to each subject. The randomization sequence was generated by a person not involved in the study. The randomization codes were sealed in tamper evident envelopes and preserved accordingly. The integrity of the envelopes was checked during each monitoring visit. The study medications were matched for appearance and weight. They were packed in identical containers with identical labels.
Ethics
The protocol, its amendments, and all other study-related documents, including the informed consent form (ICF), were reviewed and approved by Institutional Ethics Committee (IEC), BYL Nair hospital and TN medical college, Mumbai, and by the Independent Ethics Committee, Worli, Mumbai. Signed and dated informed consent was obtained from each subject prior to screening. The investigators ensured that the subjects were given adequate information about the study prior to participation. The study was conducted in compliance to International Conference on Harmonization-Good Clinical Practices (ICH-GCP) guidelines.
Objectives and endpoints
The primary objective of the study was to assess the symptomatic relief achieved with the low- and high-dose SDG versus placebo, as measured by a change in the (American Urological Association Symptom Index [AUASI]) score from baseline to end of treatment. Secondary objectives of the study were (i) to determine the most effective dose of SDG at which maximum symptomatic benefit could be achieved as judged by the investigators, (ii) to assess the extent of reduction of postvoiding residual urine volume and prostate volume/mass/size, (iii) to determine the effect on serum testosterone (total and free) and dihydrotestosterone (DHT), and (iv) to evaluate the safety of flaxseed extract.
The AUASI includes seven questions regarding frequency, nocturia, weak urinary stream, hesitancy, intermittence, incomplete emptying, and urgency designed to capture the severity of BPH symptoms. This index has been validated by the AUA and was proven to be clinically relevant, reliable, valid, and responsive. 14 Individual-question responses were assigned a score ranging from 0 to 5, which are then summed to form a total score ranging from 0 to 35. Subjects' self-assessment of therapy was also included in the study as a secondary endpoint. Subjects were asked whether they were satisfied with the new therapy and whether they would prefer to continue the therapy even after the study. Incidence of adverse events (AEs) and serious adverse events (SAEs), including adverse clinical and laboratory findings, across the treatment groups were the safety endpoints. For assessment of serum testosterone, DHT, and laboratory parameters, fasting blood samples were collected and analyzed at Metropolis Health Services, Mumbai. Blood samples for assessment of serum testosterone and DHT were collected at baseline and at end of treatment. For safety assessments, blood samples were collected at screening and at end of treatment.
Study subjects
Newly diagnosed subjects of BPH aged 45–75 years as confirmed by ultrasonography and by symptoms, AUASI score of ≥13, prostate-specific antigen (PSA) levels ≤4 ng/mL, and postvoiding residual urine volume between 30 and 200 mL were included in the study.
Subjects receiving 5α-reductase inhibitors and alpha blockers or those receiving a combination therapy or anticholinergic drugs were excluded from the study. Subjects with atonic bladders and/or neurogenic bladder, detrusor hyporeflexia/areflexia (detrusor instability or overactivity) as known from their history or diagnosed with active urethral structures, bladder neck contracture, acute prostatitis affecting bladder function, prostate or bladder malignancy, history of prostate surgery, those presenting with postvoiding residual urine volume ≥200 mL were also excluded from the study. Urge incontinence, bladder stone, hematuria, acute urinary retention or a history of the same within the previous 12 weeks, and other urogenital disorders were the other exclusion criteria.
Study treatments
The study consisted of three treatment groups: low-dose active (LDA) and high-dose active (HDA) treatment groups and placebo. Capsules containing 500 mg of LinumLife EXTRA equivalent to 100 mg SDG were provided by Frutarom Netherlands (Ede, The Netherlands), and used for the LDA and HDA groups and identical capsules with maltodextrin for the placebo group. The LDA group received one capsule each of active containing 100 mg of SDG and one placebo capsule containing maltodextrin. The HDA group received two active capsules each containing 100 mg of SDG equivalent to a daily dose of 200 mg SDG. The placebo group received two maltodextrin capsules. The capsules were manufactured at Adroit Pharmaceuticals Pvt. Ltd. (Nagpur, Maharashtra, India).
Statistics
Since this was an exploratory study, no statistical method was used for determination of sample size. We planned to screen about 130 subjects and recruit 72 subjects to get at least 60 evaluable cases. As data of five subjects were not considered, an additional eight subjects were recruited into the study.
Kruskal–Wallis test and Friedman test, each followed by Dunns' test, were used to compare results from the AUA symptom score between treatment groups and within the treatment groups, respectively. Results of the secondary efficacy endpoints prostate size, prostate mass, and residual urine volume were analyzed using Kruskal–Wallis test followed by Dunns' test and Wilcoxon matched pair test across and within the treatment groups, respectively.
Chi-square test was used to analyze the results of the investigators' overall assessment, subjects' self-assessment, tolerability, and demographic data pertaining to subjects' occupation and dietary habits. Data regarding safety and vital parameters were compared between treatment groups using the one-way analysis of variance (ANOVA) followed by Tukeys' test. Student's paired t-test and repeated-measure ANOVA were used for within-group analysis of these results. One-way ANOVA followed by Tukeys' test was used for determining the treatment differences with respect to age, within and across the treatment groups. Confidence intervals of 95% were considered and “P” values<.05 were considered as statistically significant. Data analyzed for a given endpoint were taken from those subjects for who all values for that particular endpoint were available as per protocol.
Results
Subject disposition
Figure 1 presents a flowchart of subject disposition during the study. Subjects who completed AUASI scoring for all visits were considered to have completed the study. A total of 80 subjects were recruited and randomized into the three treatment groups. Out of these, five subjects were excluded (one subject's file was lost and four subjects' data were not considered due to noncompliance to GCP). At the end of the study, 60 subjects completed the study as per the protocol of specified visits.
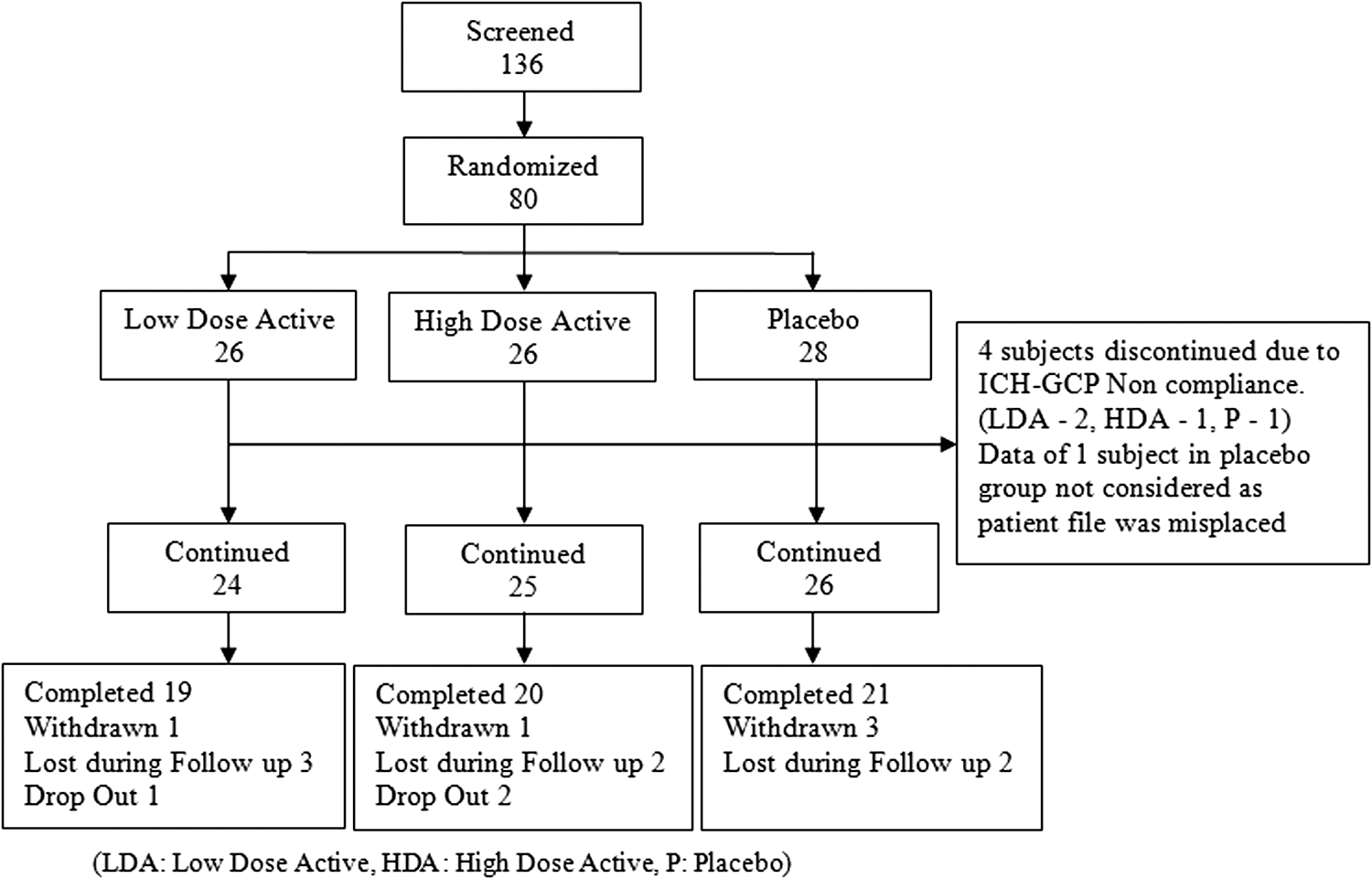
Disposition of subjects.
The demographic characteristics of age, diet, and occupation as well as the AUASI scores were comparable at baseline and there were no significant differences among the study groups (P>.05) (refer Table 1).
AUASI, American Urological Association Symptom Index; PSA, prostate-specific antigen; SD, standard deviation.
Primary efficacy results
Table 2 presents a summary of AUASI scores.
P<.001, ** P<.01, and * P<.05 as compared with baseline.
Q1–Q7 refer to the seven items on the AUASI scale. For each of these items, please refer to the text.
B, baseline; W2–W8, weeks 2 to 8.
AUASI scores
A statistically significant decrease in the sensation of incomplete bladder emptying was reported in LDA and HDA groups at week 8 as compared with baseline (P<.05 and P<.01, respectively). A statistically significant decrease was reported in the HDA group at week 6 as well in comparison to baseline values (P<.01). The decrease observed in the placebo group was not statistically significant.
A statistically significant decrease was observed at week 2 (P<.01) and at week 8 (P<.001) as compared with baseline in LDA group. In the HDA group, a statistically significant decrease from baseline was also observed at week 8 (P<.05). In the placebo group, the decrease from baseline was statistically significant at weeks 4 and 6 (P<.01) and week 8 (P<.001).
The LDA and HDA groups demonstrated a statistically significant decrease in this symptom from baseline at week 8 (P<.05). No statistically significant difference was seen in placebo group.
In LDA group, as compared with baseline, a statistically significant decrease was observed at week 8 (P<.01) in the difficulty to postpone urination. At weeks 6 and 8, a statistically significant difference was observed (P<.05 and P<.01, respectively) as compared with baseline in the placebo group. Though a decrease was observed in HDA group too, it was not statistically significant.
A statistically significant decrease in the frequency of a weak urinary stream was noted at week 6 (P<.01) and at week 8 (P<.001) as compared with baseline, in LDA group. A similar statistically significant finding was noted for HDA group as well at week 6 (P<.05) and week 8 (P<.01). Though a statistically significant decrease was not noted for this symptom at week 8, the reduction observed at week 6 was statistically significant (P<.05).
As compared with baseline, a statistically significant reduction in the need to push or strain to begin urination was observed in LDA and HDA groups (P<.05 and P<.01, respectively). No statistically significant reduction was observed in the placebo group.
No statistically significant reduction was observed in the score of night-time awakenings from baseline to week 8 in LDA group. A statistically significant reduction was observed at week 6 (P<.01) and week 8 (P<.001) in the HDA group. A similar statistical reduction was also observed in the placebo group, at weeks 4 and 6 (P<.01) with an increased statistical significance noted at week 8 (P<.001).
Total AUASI score
Each of the three treatment groups demonstrated symptomatic benefit on the total AUASI score at weeks 6 and 8 as compared with baseline. Comparison of week-8 symptom scores for all the three groups to baseline values demonstrated a statistically significant reduction (P<.001 for all the groups). However, the first statistically significant reduction in symptom score from baseline was observed at week 4 in the placebo group (P<.001).
For each of the seven individual questions as well as for the total score, no statistically significant treatment differences were noted when comparing the three treatment groups.
Effect on prostate size, mass, and residual urine volume
The changes observed for the three treatment groups from baseline to week 8, with respect to prostate size, mass, and residual urine volume postvoiding have been summarized in Table 3.
P<.05 and *** P<.001 as compared with baseline using Wilcoxon matched pair test.
A statistically significant reduction was observed in prostate size and residual urine volume in HDA, and prostate mass and residual urine volume in placebo group at week 8 as compared with baseline. However, the change was not statistically significant when compared across the groups for any of the variables.
Effect on the levels of serum testosterone (total and free) and serum DHT
Serum testosterone and DHT levels at baseline and at end of study are provided in Table 4. A rise in total and free serum testosterone levels accompanied with a decrease in serum DHT levels was observed in LDA and HDA groups at week 8 as compared with baseline values. On the other hand, in the placebo group, a rise was noted in the testosterone as well as DHT levels at week 8. A statistically significant increase in total and free serum testosterone levels was observed only in LDA group at week 8 as compared with baseline.
P<.05 as compared with baseline using paired t-test.
DHT, dihydrotestosterone.
Tolerability of the flaxseed hull extract
The majority of subjects in the study rated the tolerability of the treatment as “good.” All subjects in HDA group rated the tolerability as “good” whereas only two subjects each in LDA and placebo rated the tolerability as “fair.”
Subjects' opinion regarding the treatment
It is notable that an almost equal number of subjects in each of the three treatment groups were satisfied with the treatment received during the study and preferred to continue with the study treatment poststudy completion.
Overall assessment of therapy by the investigator
The investigators rated the treatment response as “good” or “excellent” for the majority of subjects across the three treatment groups (A total of 15 [71.4%], 14 [66.6%], and 12 [54.5%] subjects were rated as “good” or “excellent” in LDA, HDA, and placebo groups, respectively.). A higher number of subject responses in the placebo group (8 [36.3%]) were rated as “fair” as compared with LDA (2 [9.5%]) and HDA (5 [23.8%]) groups. In contrast to this, the treatment response of a higher number of subjects in the LDA group (4 [19%]) was rated as “poor,” as compared with subjects in the HDA (1 [4.7%]) and placebo groups (2 [9%]). The investigators did not rate the treatment response of any of the subjects as “very poor,” with the exception of one subject in the HDA group.
Adverse events
A brief summary of the AEs that occurred during the study is presented in Table 5. A total of 27 AEs occurred: 7 in LDA, 6 in HDA, and 14 in the placebo groups; of which, 22 were mild and 5 were moderate in intensity. The majority of AEs were not related to the study treatment, two were termed as probably related (AEs of nausea and dyspepsia that occurred in two subjects in the placebo group), and one AE (AE of breathlessness that occurred in one subject in the placebo group) was termed as unknown. The 27 AEs occurred in a total of 18 subjects across the 3 treatment groups. AEs were reported in a higher number of subjects in the placebo group (18 [81%]) as compared with LDA and HDA (AEs were reported in 6 [28.5%] and 2 [9.5%] subjects in LDA and HDA groups, respectively).
AE, adverse event; BP, blood pressure; ESR, erythrocyte sedimentation rate; WBC, white blood cell.
The only SAE reported during the study was the death of a 73-year-old subject in placebo group. The subject had a sudden death due to cardiac arrest. The subject had been on aspirin, amlodipine, and multivitamin tablets for the past 6 years. The investigator's assessment showed that this SAE was not related to the flaxseed hull extract.
Hematological, biochemical, and vital parameters
No clinically significant changes were observed in the values of hematological, biochemical, and vital parameters from baseline to end of treatment, in any group.
Discussion
In this study, supplementation with the flaxseed hull extract provided greater relief than placebo in obstructive symptoms of BPH, such as sensation of incomplete bladder emptying, “stopping and starting” while urinating, weak urinary stream, and “straining while urinating.” Low and high doses of the flaxseed extract provided statistically significant improvements in the scores of these obstructive symptoms at week 8 as compared with baseline. In contrast to this, the placebo group did not show a statistically significant improvement with respect to these obstructive symptoms.
With respect to the irritation-related symptoms included in the AUASI questionnaire, both placebo and treatment with flaxseed extract showed a statistically significant improvement in reducing the repetitive urge to urinate after 8 weeks as compared with baseline. The fact that a statistically significant improvement was seen in six out of the seven items of AUASI questionnaire in LDA and HDA groups as compared with only three out of the same seven items in the placebo group cannot be overlooked. However, due to a strong placebo effect, the difference between the treatment groups and placebo was not significant. The results obtained for the irritable BPH symptoms on the AUASI might be attributable to the limitations of the study design and the choice of SDG doses. A relatively small sample size chosen for the study could have led to larger data variances and a reduction in the statistical power of the study. This might have prevented a few efficacy variables from attaining statistical significance, in spite of notable changes across or within the treatment groups. Also, the study duration was relatively short. The maximum effect of the active treatment can often not be observed in short clinical studies, especially for studies with nutraceutical ingredients. Moreover, since this was a placebo-controlled study, a certain degree of “placebo effect” also seems to have confounded the efficacy results of the active treatment. This strong placebo effect in combination with short study duration was also observed in a recently published study that investigated the effects of a nutraceutical ingredient on overactive bladder-related voiding dysfunction and quality of life. 15 Despite the strong placebo effects observed after 4 and 8 weeks, these effects returned to baseline after 12 weeks. This allowed the researchers to observe statistically significant effects for the treatment group after 12 weeks, implying that the length of the study was of importance.
Two human studies have previously investigated the effect of flaxseed lignan supplementation on BPH. In the first study Demark-Wahnefried et al. evaluated the effect of 30 g flaxseed per day for a period of 6 months and found a significant improvement in the PSA levels (prostate-specific antigen, biomarker for BPH). 16 The dosage of 30 g per day equals a daily dosage of ∼210 mg SDG 11 and is comparable to the highest dosage used in this study. However, the subjects within the study from Demark-Wahnefried et al. were instructed to follow a low-fat diet for the duration of the study (6 months). Within the framework of that study, the change to a healthier, low-fat diet might have resulted in stronger, more significant results on the BPH markers.
In a more recent study by Zhang et al. 13 higher dosages of 300 and 600 mg SDG were administered in the form of a lignan-enriched flaxseed extract over a period of 4 months. The study allows a closer comparison with the current study due to similar design and efficacy variables. All the treatment groups in the current study achieved a statistical significance for the total AUASI score at week 8, as compared with baseline. A similar statistically significant reduction of the total AUASI score at end of treatment as compared with baseline was reported by Zhang et al. However, it is essential to note that Zhang et al. administered higher doses of SDG. This indicates that a daily dosage of 100–200 mg SDG in the form of lignan-rich flaxseed extracts serves to prevent the onset symptoms of BPH. Something that Zhang et al. also reported in their study was the strong placebo effect. Most changes in the treatment groups were significant to baseline; however, only the QOL score (quality of life, a subjective score measured as part of LUTSs) of the highest-dosage group differed significantly compared with the placebo group. This supports what is reported in the earlier mentioned study from Shim et al. where the observed placebo effects in these kinds of studies are relatively strong.
DHT, a metabolite of testosterone, is a critical mediator of prostatic growth. A decrease in DHT values translates into decreased stimulation for prostate growth, thereby at least decelerating prostatic hyperplasia if not stopping it altogether. In the present study, DHT levels were lower in both low- and high-dose flaxseed extract groups as compared with the increased values in the placebo group. However, small subject numbers in the study and the relatively short study duration may have prevented the changes in DHT levels from being statistically significant across the groups. The reduction was also not accompanied with a decrease in prostrate size. This may suggest that the physiological effect of reducing DHT in the target tissue was not visible, necessitating a longer period of treatment. DHT is synthesized in the prostate from circulating testosterone by the action of the enzyme 5α-reductase, type 2. Therapy with 5α-reductase inhibitor markedly reduces the DHT content of the prostate and in turn decreases prostate volume and, in many cases, BPH symptoms. Hence, the oral intake of LinumLife EXTRA might be associated with a 5α-reductase inhibitory activity. But this needs to be studied further and could provide the scientific fuel for future studies on this formulation.
No major safety concerns were observed with the use of the flaxseed hull extract during the study. This further supports that daily supplementation of a standardized flaxseed extract equivalent of up to 200 mg SDG is safe for human use and leads to no adverse effects.
In conclusion, supplementation with flaxseed hull extract in this study was found to be safe and well-tolerated treatment in individuals with BPH. Further, supplementation led to a significant improvement of the serum DHT levels, a known biomarker for BPH. The significant placebo effect as well as the number of subjects per treatment group and the relative short duration of the study may explain the lack of statistical significance between groups. This study provides support that the dosage of flaxseed hull extract equal to 100–200 mg SDG may be safely used to ameliorate the symptoms of BPH.
Footnotes
Acknowledgments
This work has been conducted by Vedic Lifesciences Ltd. with the financial support of Frutarom Netherlands BV. Vedic Lifesciences Ltd. is an independent research organization, which is in no way related to Frutarom Netherlands BV nor has a financial interest in the results of the study.
Author Disclosure Statement
No competing financial interests exist.