
Abstract
For thousands of years, Chios Gum Mastic (CGM), the resin produced by the trunk of Pistachia lentiscus var Chia, has been used for culinary and medicinal purposes and several therapeutic properties have been attributed to it. CGM has been used in traditional medicine of various nations in the eastern Mediterranean area. This survey was carried out to identify biological mechanisms that could explain traditional usage and recent pharmacological findings. We reviewed the related scientific literature available from the NCBI PUBMED database on CGM studies and on natural products showing peroxisome proliferator-activated receptor (PPAR) agonist effects. We investigated whether CGM qualifies as a PPAR modulator. A large number of studies demonstrate that CGM has antioxidant, anti-inflammatory, hypolipidemic, and anticancer properties. Recently, the first evidence of CGM antidiabetic effect became known. CGM chemical composition has been extensively analyzed and the presence of several compounds, especially triterpenoids is well documented. Some of them, oleanonic acid, oleanolic acid, and gallic acid are considered to act as PPAR modulators. PPARs are nuclear receptors functioning as transcription factors and thereby controlling cellular functions at the level of gene expression. PPARs are involved in the pathways of significant diseases, such as metabolic syndrome, diabetes mellitus, dyslipidemia, inflammation, atheromatosis, and neoplasias, constituting a key target for pharmacological interventions. This article proposes that the synergistic action of some constituents of CGM on PPARs and more precisely on both PPARs isotypes-α and -γ, may be one of the major biological mechanisms via which CGM exerts its multiple effects.
Introduction
P

Chios Gum Mastic resin (from the archives of the Chios Gum Mastic Growers Association). Color images available online at
Since antiquity mastic has been used in traditional Greek medicine mainly for the treatment of gastrointestinal disorders. Ancient Greek physicians like Dioscourides and Galenos mentioned its properties and recommended its use. For thousands of years and till today mastic is used in Mediterranean cuisine, as a natural chewing gum, in perfumery, and as a relief for dyspepsia in local traditional medicine.
In the last decades Chios Gum Mastic (CGM) has been the object of numerous scientific researches providing a large number of relevant studies, which currently approach a number of 60 articles.
As it was expected the first studies described the most common and old therapeutic use of mastic in the field of gastrointestinal disorders. Several studies related to its antimicrobial, anti-inflammatory, antioxidant, hypolipidemic, antidiabetic, and anticancer properties followed since then. 1
Chemical Composition of CGM
The chemical composition of CGM has been thoroughly analyzed and a large number of compounds have been isolated and identified. 2 –10 Nevertheless, ongoing research still identifies new compounds, as is the case for mastichinoic acid A, a new tetracyclic triterpenoid recently isolated from CGM. 11
A sticky and insoluble polymer, poly-β-myrcene, constitutes approximately the 25% of total CGM. Several triterpenoids have been isolated from CGM. More specifically, total mastic gum (without the polymer) extract can be separated into acidic and neutral fractions. Acidic fraction includes all major triterpenic acids, such as masticadienonic, isomasticadienonic oleanonic acid, moronic acid, masticadienolic acid, isomasticadienolic acid, and oleanolic acid. Triterpenoid acids isolated from acidic fraction of mastic gum are depicted in Figure 2. Neutral fraction includes neutral triterpenic compounds, such as oleanolic aldehyde, 28-norolean-17-en-3-one, tirucallol, β-amyrone, isomasticadienolic aldehyde, and dammaradienone (Table 1).
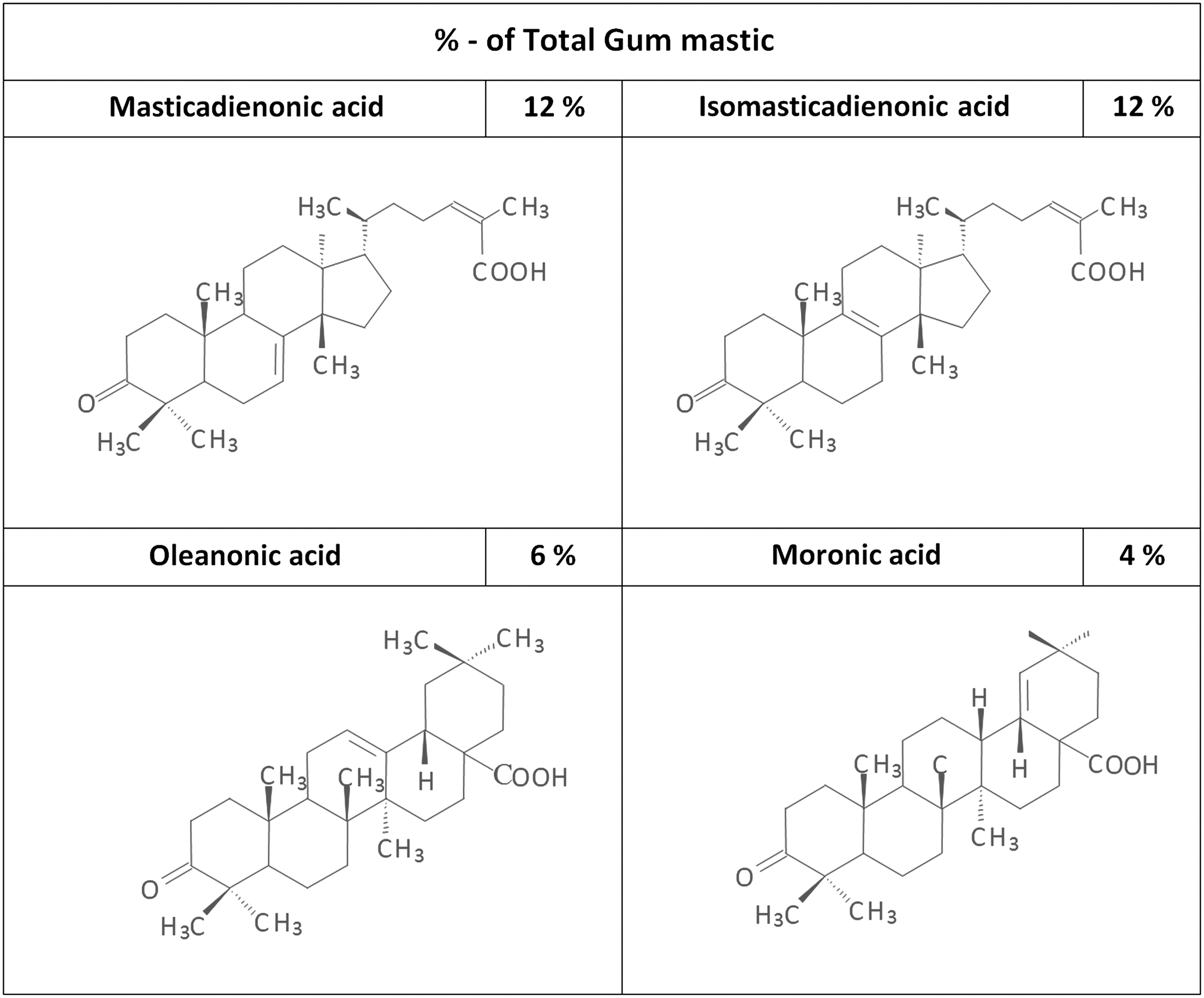
Triterpens isolated from acidic fraction of Chios Gum Mastic.
Other compounds present in smaller concentrations are verbenone, α-terpinolene, and linalool, which contribute to the antibacterial activity of mastic oil and camphene that exhibits hypolipidemic activity. 12 Also traces of gallic acid have been isolated.
It is remarkable that studies reporting antibacterial, hypolipidemic, and anti-inflammatory activity of mastic gum or mastic oil have suggested the existence of synergy phenomenon, where the combination of several compounds is more potent than any particular compound. This phenomenon of synergy is quite common with herbal products that contain several different active constituents.
Peroxisome Proliferator-Activated Receptors
Peroxisome proliferator-activated receptors (PPARs) belong to the nuclear hormone receptors family. They have structural similarity to steroid hormone receptors and they regulate lipids metabolism, cellular differentiation and proliferation, and immune response. 13 PPARs activation is followed by the formation of heterodimers with members of retinoid X receptor family. Fatty acids and fatty acids derivatives have been recognized as some of the endogenous PPAR ligands. 13 PPARs act as transcription factors, activating cellular pathways with beneficial effects on lipid synthesis and oxidation, glucose uptake and insulin sensitivity, inflammation and expression of immunoregulatory genes. Until today, three isotypes of PPARs have been identified: PPAR-α, PPAR-γ, and PPAR-β/δ (also referred as PPAR-β or PPAR-δ).
Peroxisome proliferator-activated receptor-α
PPAR-α is highly expressed in liver and skeletal muscle, and to a lesser degree in heart, kidney, and vasculature. It not only regulates genes involved in lipid uptake, catabolism and homeostasis, but also in other pathways. 14 Additional to its major role in lipid homeostasis PPAR-α exhibits pleiotropic effects on endothelial dysfunction, myocardial ischemic injury, and immune-inflammatory responses. 15 PPAR-α activation by polyunsaturated fatty acids and fibrates results in a reduction in very low-density lipoprotein triglyceride levels, an increase in apolipoprotein A-I and high-density lipoprotein (HDL)-C levels, a stimulation of “reverse” cholesterol transport, and an increase in fatty acid uptake and oxidation and in anti-inflammatory effects. 16 In particular, PPAR-α agonists increase the serum level of HDL-C via PPAR-α activation of the genes of 2 major HDL apolipoproteins, APO-I and APO-II, decrease the serum levels of triglycerides via PPAR-α-mediated inhibition of the gene of apolipoprotein C-III, a well-known inhibitor of lipoprotein lipase, and elevate the expression of genes of lipoprotein lipase and apolipoprotein A-V. The PPAR-α is considered therapeutic target mainly for hypertriglyceridemia. 17
Peroxisome proliferator-activated receptor-β/δ
PPAR-β/δ is less well studied and its action so far appears to involve fatty acid oxidation, energy consumption adaptive thermogenesis, and immunomodulation. The PPAR-β/δ expression in essentially all cell types and tissues suggests that it holds a primary role in cellular biology. 18 There are data that implicate PPAR-β/δ in fuel combustion and suggest that their activation might offset some of the weight gain issues seen with selective PPAR-γ agonists. 19 Selective overexpression of a constitutively active form of PPAR-β/δ in mouse adipose tissue induces significant weight loss and protects against the obesity and dyslipidemia induced by a high-fat diet. 20 Evidence emerging within the last few years suggests that PPAR-β/δ might be a potential therapeutic target for the treatment of disorders associated with the metabolic syndrome. More specifically, PPAR-β/δ activation improves serum lipid profile, increase insulin sensitivity, prevents weight gain, and suppresses macrophage-induced inflammation. 18,21
Peroxisome proliferator-activated receptor-γ
PPAR-γ is highly expressed in adipocytes, and to a lesser degree in skeletal muscle, liver, and kidney and its activation has been shown to regulate expression of genes that mediate adipocyte differentiation, energy metabolism, and insulin action. 14,22 PPAR-γ promotes adipocyte differentiation, stimulates fatty acid storage in adipocytes via the activation of genes, such as lipoprotein lipase, fatty acid transport protein, CD36 and acyl-coA synthase, and decreases free fatty acid secretion, resulting in enhanced insulin signaling. PPAR-γ activation regulates the expression of cytokines (e.g., decreases tumor necrosis factor-α [TNF-α]) and adipokines (e.g., increases adiponectin, decreases resistin), decreasing obesity-induced inflammation and insulin resistance. As a result PPAR-γ activation increases insulin sensitivity and therefore glucose and fatty acids uptake, in addition to anti-inflammatory effects. Clinically, selective PPAR-γ agonists like thiazolidinediones (TZDs) are being used for the treatment of diabetes mellitus type 2. 23,24 However, selective PPAR-γ agonists also cause water retention, weight gain, peripheral edema, and possibly congestive heart failure among several other side effects. Such adverse effects may contribute to controversial cardiovascular outcomes despite apparent improvements in other risk factors. 25
PPAR-Ligands
Single, dual, and pan-PPAR agonists
Recently, research has focused on combination therapies with drugs that have the ability to simultaneously act on more than one isotype of PPARs. In theory, these new nonspecific PPAR agonists, having the ability to act on two (dual agonists) or even all three (pan-agonists) PPAR isotypes, would provide broader therapeutic potential, with beneficial effects on glucose and lipid metabolism. The ultimate goal of this approach is to provide greater efficacy, with an improved safety profile at the same time. Although the first dual PPAR agonists have been already designed, even the more promising of them—muraglitazar and tesaglitazar—have failed to prove their merit in large-scale phase III clinical trials. 26 Despite the provided evidence of high effectiveness on improving both, glucose and lipids homeostasis, safety issues were serious enough to ignore. Weight gain, fluid retention, and edema, anemia, elevated serum creatinine, decreased glomerular filtration rate, and increased incidence of major cardiovascular events rate were some of the adverse effects recorded during the clinical trials. 27 The PPAR agonists capable of activating all three PPAR subtypes are characterized as pan-agonists. From a pharmacological point of view, the idea of all PPARs acting harmonically on the whole body level as the result of balanced pan-PPAR activation is extremely fascinating. They are expected to exert beneficial effects in an array of metabolic disorders, especially in insulin resistance, diabetes mellitus, obesity, and dyslipidemia. Clinical experience with bezafibrate, a balanced pan-PPAR activator, is quite promising. Improved insulin sensitivity, lower glucose and triglycerides levels, and higher HDL levels were documented following bezafibrate's administration. 28,29
Medicinal-pharmaceutical PPAR agonists
All marketed PPAR-α agonists belong to the fibrates family. Fenofibrate and gemfibrozil are the two most widely prescribed fibrates. They are considered hypolipidemic agents, especially effective in reducing triglyceride levels and raising, to some extent, HDL plasma levels. Also, they reduce vascular inflammation and thrombogenicity and as a result they reduce progression of atherosclerosis and minimize the incidence of coronary heart disease. Nevertheless, fibrates are associated with side effects such as muscle weakness, myopathy, rhabdomyolisis, and cholelithiasis. 30
Although bezafibrate belongs to the fibrates family it has a unique profile of action, since it is the only clinically available pan-PPAR balanced agonist. 13,31 Bezafibrate reduces plasma triglycerides level, increases plasma HDL-C level, and decreases the prevalence of small dense LDL particles remnants. 28,32 In addition bezafibrate reduces fibrinogen concentrations, TNF-α, interleukin-6 (IL-6), and C-reactive protein (CRP) levels, thus exerting antiatherogenic and anti-inflammatory activity. 29 The main difference between bezafibrate and other fibrates is the fact that bezafibrate demonstrates beneficial effects on glucose level and insulin resistance. 29 PPAR-γ activation by bezafibrate is probably one of the mechanisms that lead to this result. Increased level of adiponectin following bezafibrate treatment is mediated mostly by PPAR-α, but also partially by PPAR-γ activation. 33 Finally bezafibrate, despite its potential to act on PPAR-γ, is not associated with weight gain, probably due to PPAR-β/δ-mediated effects. 34
TZDs are the most well known PPAR-γ activators and they have been in use for many years, as antidiabetic drugs. They have been shown to be efficacious in establishing glycemic control, in both monotherapy and combination therapy. Even though the molecular mechanisms by which TZDs exert hypoglycemic and insulin-sensitizing effects are not totally understood, adipose tissue appears to be the major organ implicated. It is the insulin sensitizing effects of TZDs that result in long-term glycemic control, as shown in A Diabetes Outcome Progression Trial (ADOPT). 35
Evidence from the large PROactive study suggests that pioglitazone may exert protective effects in patients with diabetes mellitus type 2 and macrovascular disease. 36 The currently marketed TZDs—pioglitazone and rosiglitazone (controversy about rosiglitazone use still exists)—are potent and selective PPAR-γ agonists that increase insulin sensitivity. On the other hand, TZDS are associated with several side effects, mainly weight gain, peripheral edema, myocardial ischemia, heart failure, osteoporosis, and urinary bladder cancer. 37
Herbal-natural PPAR agonists
In the past decades the search for compounds with medicinal effects coming from natural sources—plants, herbs, fruits etc—has been intensified. As a result of this effort several herbal-natural products have been identified as PPARs modulators.
Water soluble extract from stem parts of Curcubita moschata (pumpkin) and aqueous extract of Melissa officinalis (Labiatae), Morus alba (Moracae), and Artemisia capillaris (Compositae) have been identified as PPAR-α agonists, but the active compounds responsible for their effects have not yet been isolated. 38,39 Salacia oblonga root extract has been shown to improve serum lipid levels and hepatic lipid metabolism at least in part via PPAR-α activation. 40 Mangiferin, one of the main components in S. oblonga root extract, has been shown to be at least partially responsible for the PPAR-α activating potential of S. oblonga's root extract. 41 Gynostemma pentaphyllum is another herb used in the traditional Chinese medicine for the treatment of inflammatory and cardiovascular diseases. Gypenoside XLIX, a damaran-type glycoside, isolated from G. pentaphyllum has been shown to exert its effects via PPAR-α-dependent pathways. 42
Zingiber officinale (ginger)-derived components and specifically 6-shogaol, have been shown to act as PPAR-γ agonists. 43 Ginseng, another oriental traditional medicine, has been extensively researched and its beneficial effects on cardiovascular, neurological, and endocrine diseases are well documented. Ginsenosides are the chemical compounds responsible for ginseng actions. One of them, 20(S)-protopanaxatriol has been shown to increase PPAR-γ activity and another one, ginsenoside Rb1, has been identified as a PPAR-γ2 agonist. 44,45
Momordica charantia (bitter melon) has been shown to increase liver PPAR-α and adipose PPAR-γ mRNA levels. 46 The gum resin of Commiphora mukul (gugul) demonstrates dual agonostic properties for PPAR-α and PPAR-γ. Commipheric acid and guggulipid seem to be the active compounds responsible for the dual effects of C. mukul. 47 Punica granatum (pomegranate) has been used in traditional Greco-Arabic (Unani) medicine as an antidiabetic agent. P. granatum's dual PPAR-γ and PPAR-α-activating properties are attributed to active compounds such as oleanolic acid and gallic acid. Oleanolic acid belongs to triterpenoid family and seems to enhance PPAR-α activity. Gallic acid is a polyphenolic compound and seems to be at least partially responsible for the PPAR-γ-related effects of P. granatum's extract. 48
Finally, there is only one herbal product identified as pan-PPAR agonist and it is derived from the Bitter Chinese tree Pseudolarix kaempferi. Pseudolaric acid B isolated from the bark of P. kaempferi is considered to be the active compound with the potential to activate PPAR-α, PPAR-β/δ, and PPAR-γ. 49
Biologic Effects of CGM–Are They Related to PPAR Modulation?
Nature seems to be a few steps ahead in respect to human science and concomitant modulation of various PPAR isotypes by natural products is a fact. The value of this type of concomitant modulation has been recognized and several natural products have been identified as dual or pan PPAR agonists. CGM may be characterized as a natural product presenting properties of a PPAR agonist. In this study we reviewed the related scientific literature available from the NCBI PUBMED database on CGM studies and on natural products with PPAR agonist effects and we investigated whether CGM qualifies as a PPAR modulator. Our target was to define the properties of a herbal product that could assign it as a PPAR modulator.
Effects on lipids metabolism
CGM has been proven to be a potent antioxidant, extremely efficient in protecting human LDL from copper-induced oxidation in vitro. 50 Total polar extract of CGM inhibits the cytotoxic effect of oxidized LDL on peripheral blood mononuclear cell, which undergo apoptosis and necrosis when exposed to oxidized LDL without the presence of CGM. Oxidized LDL decreases GSH level and upregulates CD36 expression, while mastic total polar extract restores GSH levels and downregulates CD36 expression. Fractions of total extract of CGM derived from Reverse Phase High-Performance Liquid Chromatography analysis were examined for their antioxidant activity, and the triterpenoid fraction was the one to exhibit remarkable increase in intracellular GSH. Restoration of GSH and downregulation of CD36 expression are the pathways for mastic triterpenes to exert their antioxidant/antiatherogenic effect. 51 The hypolipidemic effect of mastic gum essential oil (MGO) has been investigated in naive and in rats susceptible to detergent-induced hyperlipidemia. MGO administration into naïve rats resulted in a dose-dependent reduction in serum total cholesterol, LDL, and triglycerides levels by as much as 53.6%, 45.2%, and 30.6% respectively. In hyperlipidemic rats, MGO administration also produced substantial reduction of total cholesterol, LDL, and triglycerides levels, by as much as 59.9%, 72.5%, and 65.4% respectively. The effects of various components of MGO on plasma lipids level were tested to determine the active substances. The hypolipidemic effect was unequivocally associated with camphene. The lipid lowering effect of camphene was exerted in a dose-dependent manner and it was not related with inhibition of HMG-CoA. Reactivation of lipolytic enzymes by camphene for early clearance of lipids from circulation in detergent-induced hyperlipidemia was considered as an alternative metabolic process that could explain the hypolipidemic effect. The fact that administration of MGO in naive rats led to the same reduction of total cholesterol, LDL, and triglycerides plasma levels implies that camphene may act as an LPL activator. Camphene represents only a minor constituent of MGO—approximately 0.83%. Administration of camphene alone resulted in lower lipid reduction than the administration of total MGO. On the other hand, administration of camphene in combination with all the five major constituents of MGO had almost the same degree of efficacy with total MGO, implying a synergism phenomenon between several substances. 12 In another study investigating the hypolipidemic effect of CGM on diabetic mice, total CGM in the form of powder was administered, blended with the food, in low and high dose for 8 weeks. The low-dose group presented significantly lower serum levels of total cholesterol, LDL-C and triglycerides and significantly higher levels of HDL-C. The high-dose group presented significantly lower levels of triglycerides. 52 Administration of total mastic extract without polymer and of neutral mastic fraction in hypercholesterolemic rabbits reduced the total cholesterol concentration by 47 and 88% respectively, demonstrating significant hypolipidemic activities. 53 Total mastic extract has been administered to healthy humans over the age of 50. Subjects were randomly assigned to two groups and received daily 5 g of mastic powder (high dose) for 18 months or a mastic solution (low dose) for 12 months. A decrease in serum total cholesterol, LDL-C, total cholesterol/HDL-C ratio, apolipoprotein A-1, and apolipoprotein B was observed in the high-dose group, while apoB/apoA-1 ratio did not change. 54
The studies above provide evidence that CGM exerts beneficial effects on lipid metabolism. Most of these studies demonstrated significantly lower levels of total and LDL cholesterol, two of them lower levels of triglycerides and one higher levels of HDL. Restoration of intracellular GSH and downregulation of CD36 expression are possible pathways for the mastic triterpenes to exert their antioxidant/antiatherogenic effect. Also camphene, in synergy with other mastic constituents, plays a significant hypolipidemic role, independent of HMG-coA, possibly via LPL activation. The profile of CGM effects on lipid metabolism is quite consistent with the hypothesis that CGM acts as PPAR-α agonist (Table 2).
NS, non significant; ↓, weak; ↓↓, moderate; ↓↓↓, strong effect. Down-ward arrows indicate reduction and upward arrows indicate increase.
CGM, chios gum mastic; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PPAR, peroxisome proliferator-activated receptor.
Effects on glucose metabolism
The antidiabetic effect of CGM is a rather new finding and so far there is not a large body of evidence to support it. For the first time evidence of glucose lowering activity was provided by Triantafyllou et al., where in the low-dose group, glucose levels were significantly decreased in male subjects. 54 In the study by Georgiadis et al., CGM exerted a surprisingly potent antidiabetic activity, substantially lowering glucose levels in both low- and high-dose groups of mice. 52 It is of interest to comment here that the low-dose group presented better results compared with the high-dose group, which is in accordance with the findings of Triantafyllou et al. 54
In search for new antidiabetic compounds, Petersen et al. developed a pharmacophore model based on partial agonists of PPARγ. 55 They combined in silico and in vitro methods to identify natural compounds that act as PPAR-γ agonists. They used pharmacophore-based virtual screening for the initial screening of target compounds and then verified the hits using bioassay-guided chromatographic fractionation. The model was used for the virtual screening of the Chinese Natural Product Database, a library of plant-derived natural products used in traditional medicine. Methyl oleanonate, a compound found among others in CGM, was one of the resulting hits. The acid of methyl oleanonate-oleanonic acid- was identified as a PPAR-γ agonist through bioassay-guided chromatographic fractionations of CGM fractions. Testing of oleanonic acid data in dose–response studies led to the conclusion that it acts as a low potency PPAR-γ activator with an efficacy reaching approximately 20% of the activity of rosiglitazone at saturating concentration. Some of the others subfractions of CGM and consequently some other substances, also exhibited biological activity toward PPAR-γ. The existence of pharmacokinetic synergy, where the pharmacological effect of CGM could be the result of multiple compounds acting in combination toward the same biological target, is very possible. 55 Evidence of antidiabetic activity and the presence of oleanonic acid support the hypothesis that CGM can exert some of its effects via PPAR-γ activation (Table 3).
−, no relation; +, weak relation; ++, significant relation.
Effects on inflammation and inflammatory bowel disease
CGM inhibits one of the main cellular sources of superoxide and H2O2 indirectly by blocking the PKC-dependent activation of NADPH oxidases. This antioxidant property may have direct implication to the anti-inflammatory activity of CGM. 56 Also, mastic inhibits the production of pro-inflammatory substances such as nitric oxide (NO) and prostaglandin E2 (PGE2) by activated macrophages mainly via the inhibition of iNOS and COX-2 protein expression and to a lesser degree mRNA expression, rather than by NO scavenging. 57 CGM and an isolated phytosterol tirucallol exhibit anti-inflammatory activity in human aortic endothelial cells. Both CGM extract and tirucallol significantly inhibit vascular cell adhesion molecule-1 and intracellular adhesion molecule-1 (ICAM-1) expression in TNF-α-stimulated human aortic endothelial cells and they also inhibit the binding of U937 cells to TNF-α-stimulated human aortic endothelial cells and attenuate the phosphorylation of NF-κB p65. 58 (Table 4)
CRP, C reactive protein; ICAM, intracellular adhesion molecule; IL-6, interleukin-6; MIF, migration inhibitory factor; MMP-2, matrix metalloproteinsase 2; NO, nitric oxide; PGE2, prostaglandin E2; TNF-α, tumor necrosis factor-α; VCAM, vascular cell adhesion molecule; VEGF, vascular endothelial growth factor.
Another aspect refers to the effectiveness of CGM on the clinical course and plasma inflammatory mediators of patients with active Crohn's disease. A significant reduction of CD activity index, plasma IL-6 and CRP level were recorded after CGM therapy. 59 Moreover, reduction of TNF-α and increase in the macrophage migration inhibitory factor have been documented in patients with active Crohn's disease treated with CGM. 60 Also, in studies on experimental colitis, CGM administration resulted in significant reduction of inflammatory markers as TNF-α, IL-6, and ICAM-1 and downregulated NF-κB p65. 61,62 (Table 4)
It is of interest to note that a growing body of evidence indicates that PPAR-α and PPAR-γ have an anti-inflammatory effect on inflammatory bowel disease (IBD) and its agonists may serve as an additional therapeutic choice. It has been demonstrated that PPAR-α mediates anti-inflammatory effects of glucocorticoids in a mouse model of chemically induced colitis. 63 In the same model deletion of PPAR-α aggravated colitis, whereas activation of PPAR-α by its agonist activity significantly reduced colonic inflammation. 64 In the case of PPAR-γ there are several lines of evidence to support its therapeutic value. In mouse models of chemically induced colitis PPAR-γ mediates the anti-inflammatory effect of 5-aminosalicylic acid (5-ASA), and TZDs reduce colonic inflammation suggesting that PPAR-γ suppresses inflammation in IBD. 65,66 Also, in two trials in humans, one open label and one randomized placebo-controlled, rosiglitazone demonstrated a therapeutic effect in patients with ulcerative colitis. 67,68 CGM ability to modulate both PPAR-α and -γ provides a biological mechanism, which could explain its beneficial effect on IBD (Table 3).
CGM anticancer effects
In the last decade, several studies provided evidence that CGM may possess anticancer activity in some types of human neoplasia and specifically prostate, 69 –71 lung, 72,73 colon, 74 –76 and hematological malignancies. 77,78 The ability of CGM to inhibit cell proliferation through extrinsic and intrinsic apoptosis signaling pathways appears to be the cornerstone for its anticancer activity. Specifically, CGM suppresses NF-κB and JAK-STAT pathways, inhibits vascular endothelial growth factor, and depletes GSH. Among CGM constituents, it is the triterpenoids again that appear to be responsible for its anticancer activity. Mastic oil may also exhibit antimetastatic potential since there is evidence that it can prevent crucial processes related to cancer metastasis (Table 4). Evidence indicate that mastic oil could limit the metastatic potential of Lewis lung adenocarcinoma cells via downregulation of matrix metalloproteinsase 2 expression, actin cytoskeleton remodeling, and tumor endothelial adhesion and attenuation of tumor-related angiogenesis. 79
There is an extensive literature with contradictory results about PPARs implication in the promotion and development of cancer. Although a large number of studies report that expression and activation of PPARs correlate with positive outcome against cancer, this is not a universal phenomenon. This diversity seems to arise from issues such as cell-type and organ-specific effects, stage of cancer, time of exposure to related ligands and other variables. Nevertheless, in some cases the evidence is more uniform and compelling. In this regard, decreased expression of PPAR-γ has been associated with poor prognosis in lung cancer and activation of PPAR-γ has been found to inhibit growth of human lung cancer cells. 80,81 Data also suggest that PPAR-γ acts as a colon cancer suppressor and that decreased expression of this receptor may increase colon cancer risk. 82,83 Modulation of PPAR-γ could be at least partially responsible for some of CGM anticancer effects (Table 3).
Conclusions
Several studies have shown that CGM exerts beneficial effects on lipid and glucose metabolism, on inflammation and IBD and on various types of cancer. CGM antibacterial activity is also well documented. These effects build the pharmacological profile of a herbal product that can modulate both PPAR-α and PPAR-γ. CGM is a natural mixture of several compounds. Some of them, oleanolic acid, oleanonic acid, and gallic acid, have been already known to act on PPARs. Many studies on the CGM have reached the conclusion that most of the effects are the result of pharmacological synergy between several compounds and it seems very possible that beside the aforementioned compounds there are others with similar activities. Further studies are required to establish the PPAR modulating potential of CGM, to clarify its PPAR-mediated effects and to specify the formula of its active compounds.
Footnotes
Author Disclosure Statement
No competing financial interests exist. No conflicts of interest declared.