
Abstract
The drugs used in chemotherapy treatments have little specificity, attack tumor cells, and also injure proliferative tissues. Knowledge of the functions of micronutrients has greatly increased, especially of Selenium (Se) that presents immunomodulatory and antitumor functions. The present study evaluated the health-related quality of life of patients undergoing chemotherapy for the treatment of leukemias and lymphomas (LL) and solid tumors (ST) while receiving Selenium (Se) supplementation. This is a randomized, double-blind, crossover study that evaluated the quality of life (EORTC-QLQ-C30 questionnaire), renal and liver functions of patients supplemented with Se. There was no statistically significant alteration in LL patients. However, the fatigue and nausea scores after 30 days did decrease in this group as well as in the ST group. After 1 year supplementation with Selenium, a more noticeable decrease in the scores concerning fatigue and nausea could be observed in the ST group, when compared with the beginning of the study. The LL patients also presented a decrease in the fatigue scores and physical functions. The kidney function as well as liver function has improved after Selenium supplementation when compared with the placebo intake in LL and ST patients, more remarkably in the LL group. Supplementation with Selenium promotes the reduction of chemotherapy side effects in cancer patients, especially by improving the conditions of patients with fatigue, nausea, and impaired physical function. Renal and liver functions have also improved.
Introduction
T
Selenium deficiency is frequently associated with the decrease in infection resistance, the antibody synthesis, the lymphocytes proliferation, and the cytokines secretion. Moreover, it considerably increases tumorigenesis. 4 –6 Selenium is also an essential nutritional factor for the development and expression of immune response mediator cells that act against malignant cells. 7 The inverse relation between cancer incidence and a Se-enriched diet is reported in experimental and epidemiological studies. 8 –10 When tumors are used as models, Selenium supplementation has proved in many cases to be effective in reducing or inhibiting neoplastic growth in humans. In low concentrations, Se plays a preventive role against cancer, whereas when it is in high concentrations, it has an antitumor 5 and a hepatic protector effect. 6
Anorexia seems to be pathophysiologically associated with the increase in cytokine production in response to the tumor. This cytokine burst reduces food intake due to the fact that it stimulates leptin release and/or mimics the hypothalamic effects. 11,12 Se is able to control inflammatory status 6,11,12 and is efficient as a regulator of transcription factor - Nuclear factor-kappa B (NFκ-B), which is essential for the transcription process and the synthesis of inflammatory cytokines. 12 With these facts established, it is clear that the association between Se levels (through antioxidant system) and the control of anorexia in patients who present chronic inflammatory response, is similar to what is observed in oncologic patients.
Low serum Selenium has been shown to be associated with elevated interleukin 6 (IL-6). 13,14 Elevated serum IL-6 levels have been linked with an increased risk of reduced physical function and sarcopenia, 15,16 as well as the development of disabilities. 17,18 Thus, Selenium may also play a role in muscle weakness due to its relationship with the upregulation of IL-6 through the redox sensitive transcription factor Nuclear factor-kappa B (NF-κB). Consequently, NF-κB is a potent activator of the IL-6 promoter 19 and may be involved in the pathway through which Selenium deficiency contributes to the decline in muscle strength and mass.
Chemotherapy protocol is also responsible for cellular damage in nontarget tissues that are protected by antioxidant systems like GPx (Glutathione peroxidase) and GSH (Glutathione). In this way, kidney function is closely connected to Se levels since GPx3 (Glutathione peroxidase 3) is one kind of Selenium protein that presents elevated expression in kidney tissue, mostly in renal tubules. This fact suggests that Selenium, in an indirect manner, exerts protective function in the tissue against toxicity of the chemotherapy. 20
It is well established that Se takes part in antioxidant mechanisms, protects nontarget tissues from chemotherapeutic treatment (mostly kidney and liver) and controls inflammatory response that is associated with anorexia and muscle strength. All the above considered, the aim of the current study was to evaluate the influence of Se supplementation on nausea, fatigue, physical function, and treatment-related hepatotoxicity and nephrotoxicity in patients undergoing chemotherapy for the treatment of leukemias and lymphoma (LL) and solid tumors (ST).
Patients and Methods
Patients
Patients with leukemias and lymphomas or ST were recruited from the ABC Medical School's Pediatric Oncology Care Unit. They were of both sexes, aged up to 18 years, and they were submitted a questionnaire to evaluate their nausea, fatigue, and physical function. Patients who broke the protocol, who withdrew spontaneously, or who died were excluded.
The study was approved by the Ethics Committee of the ABC Medical School (CAAE -0103.0.290.000-09). All the patients' legal guardians (parents, grandparents, or tutors) were informed about the risks involved in the research and signed the term of informed consent.
Study design
First, this was a randomized, double-blind, placebo controlled, phase II crossover study. Second, during a 1-year follow-up after the end of the first protocol, only patients who continued to be supplemented were observed.
Upon accepting to participate in the study, patients answered the initial questionnaire (D0). They were then randomized into two groups: Group 1 received daily supplementation of Se according to the age group presented and Group 2 received placebo capsules. In both cases, administration lasted 30 days (Fig. 1). Both groups underwent a washout period (without supplementation for 7 days). After this period, Group 1 received placebo and Group 2 Selenium for 30 more days. Each patient has received 80% plus Dietary Reference Intake (DRI).
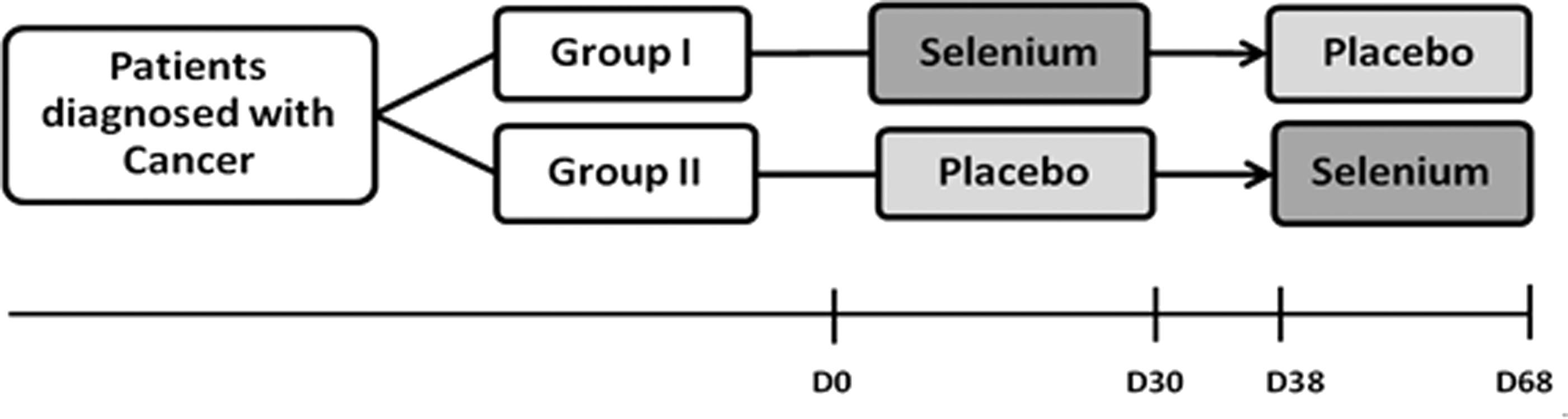
Study design: Randomization in Selenium and placebo groups during 30 days; 7-day washout; group inversion (for 30 more days).
Every 30 days blood samples were collected for urea, creatinine, liver enzymes quantification, and the patients answered the questionnaire. When the research was concluded, the scores for each parameter were calculated, followed by the calculation of the statistical significance between the obtained scores: initial versus placebo, initial versus Se, and placebo versus Se.
Eight patients from each group were followed up for a year. These patients continued to receive the daily supplementation of Selenium throughout the follow-up period and then answered the questionnaire again (D128 and D365). The administered dose was the same used during the randomization period.
Questionnaire
The questionnaire used was the EORTC-QLQ-C30 questionnaire (version 3), which has the purpose of assessing the quality of life of oncologic patients. 22 –25 It was developed by a multidisciplinary group of oncologists and scientists from different areas according to the European Organization for Research and Treatment of Cancer (EORTC) guidelines.
The third version is composed of 28 questions regarding the symptoms and functional scale. The questions were answered according to an intensity scale with four levels: not at all (1), a little (2), quite a bit (3), very much (4). There are two more questions concerning the global quality of life rated on a scale from 1 to 7, 1 being the minimum and 7 the maximum quality level.
A score was calculated from the answers given according to the orientations supplied by the European Organization for Research and Treatment of Cancer. It was then possible to measure levels of fatigue, nausea, appetite loss, and physical function.
Blood specimen collection
Approximately 5 mL of venous blood was collected from each patient after 30 days supplementation with placebo and Selenium. The specimens were placed into serum separator tubes and centrifuged at 10 g for 10 min to collect serum. Serum was analyzed after 2 h from collection for measurement of aspartate aminotransferase (AST), alanine aminotransferase (ALT), creatinine, and urea. The normal levels for the studied population were taken into account when interpreting the results.
Liver and kidney function analysis
To evaluate the possibility of hepatic dysfunction, the following laboratory tests were performed: Aspartate transaminase (AST) (Elitech®) and Alanine transaminase (ALT) (Elitech). To verify renal functions, urea (Elitech) and creatinine (Elitech) levels were analyzed. The parameters were measured by enzymatic colorimetric assay in an automated spectrophotometer from Flexor (Elitech), following the good practice in clinical laboratory analysis.
Supplementation
Group I received a daily supplementation of Selenium-glycine and Group II received glycine-starch capsules (placebo). The capsules used in both groups were identical in size and glycine dose amount, with no difference in the storage containers.
Dosage administration of Selenium corresponded to the daily value intake recommended by the DRI for children within the studied age group. Such recommendations are elaborated by the National Research Council (NRC), Food and Nutrition Board in the USA. 21 For each DRI an 80% overload was added and the following doses were established: 27, 36, 54, 72, and 100 μg of Selenium (Selenium-glycine) as presented in Table 1.
Micrograms per day.
Institute of Medicine/Food Nutrition Board, US National Academy of Sciences. DRIs for Selenium.21
Statistical considerations
The results analyses were performed by adopting a significance level of 5% (P≤.05), or, whenever possible, of 1% (P≤.01) in compliance with the following models: • Descriptive statistics; • measure of central tendency; • equality of means test (Student's t-test); • equality of medians test (Mann–Whitney); • The Software used was Prism 3.0 version.
Results
Fatigue, nausea, appetite loss, and physical function during supplementation
From September 2010 to January 2012 seventy-four patients were invited to participate in the study. As a consequence of the break in the protocol, spontaneous drop-out, or death of patients, only thirty-nine individuals finished the study. These 39 patients (19 LL or lymphomas and 20 ST) were of an average age of 8.2 years in the LL or lymphomas group, and 7.4 years in the ST group. In the former group, 9 of the patients were of the female sex and 10 of the male sex; in the latter, 8 patients were of the female sex and 12 of the male sex (Table 2).
Patients were randomized into two groups (Group I - Se and Group II - Placebo) for 30 days. Both groups underwent a washout period (7 days) and after this period, the treatment was inverted, that is, Group 1 received placebo and Group 2 Se for 30 more days. At the end of each protocol, randomization of each patient was revealed. After the application of the questionnaires, the respective scores for each evaluated parameter were calculated in each period (initial, placebo, and Selenium).
In patients with leukemia or Hodgkin lymphoma - LL Group (No=19), there were no significant alterations in the analyzed parameters (fatigue, nausea, appetite loss, physical function) when the data from the beginning of the treatment were compared with those obtained after supplementation with Selenium and the use of placebo (Table 3).
Parameters quartiles and medians concerning each randomization period (initial, Selenium, and placebo) and supplementation follow-up during 1 year (initial, D30, D128, and D365) in children and adolescents with leukemia or Hodgkin lymphoma. Q25: Quartile 25; Q75: Quartile 75.
Despite the fact that there was no statistical difference in parameters in relation to the beginning of the treatment, when the continuous supplementation of Selenium was analyzed during the period of 1 year (D30, D128 and D365), a decrease in the scores concerning fatigue and nausea could be noted when compared with the beginning of the study (Fig. 2). On the other hand, scores concerning appetite loss had an initial decrease (D30) with a subsequent increase at the end of the study.
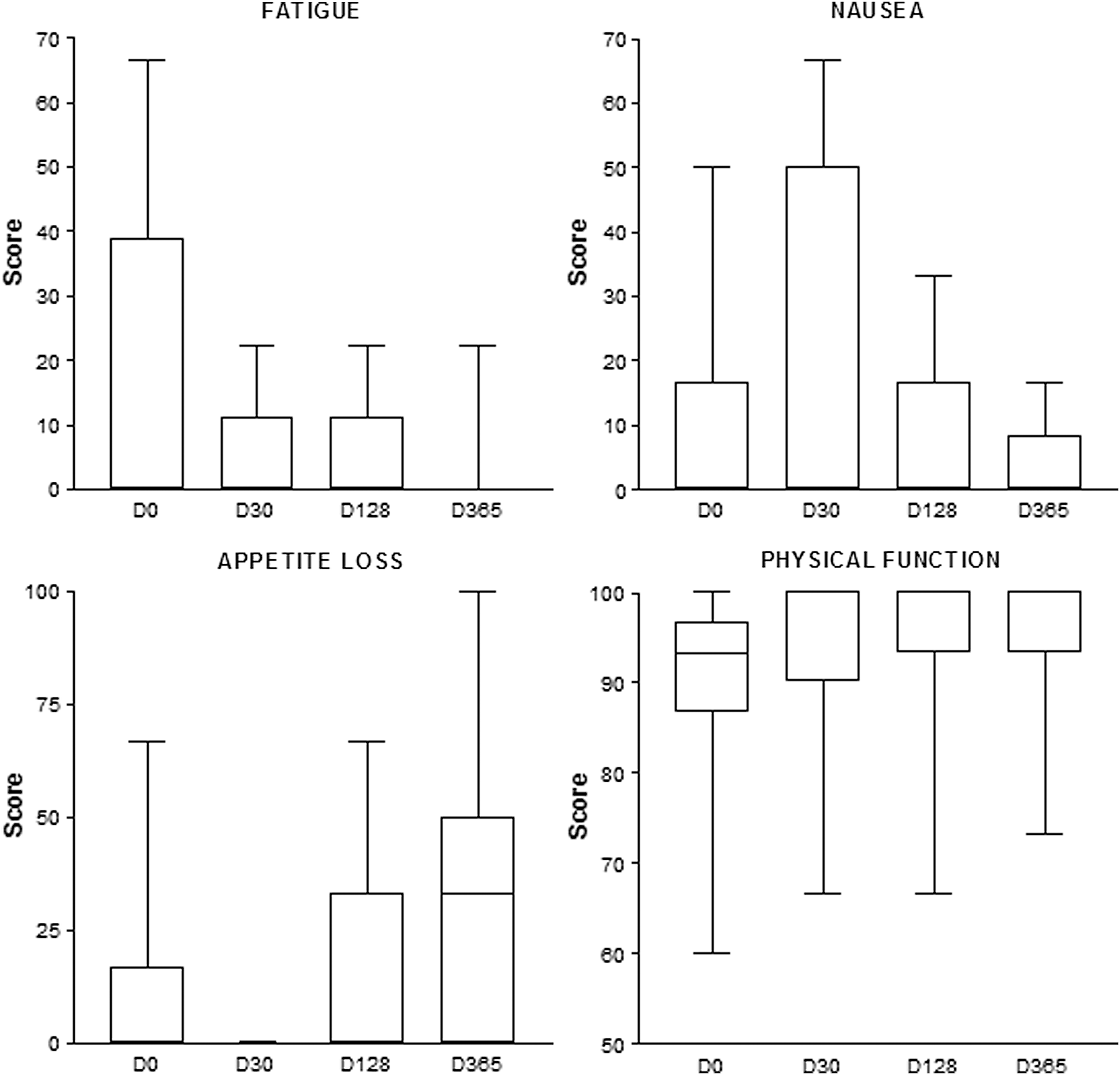
Fatigue, nausea, appetite loss, and physical function scores during the 1-year follow-up of patients with leukemias and lymphomas who were supplemented with Selenium.
In further consideration of Group LL, the physical function parameter showed an increase in scores in the first 30 days after the beginning of supplementation and this pattern was sustained throughout the evaluated year.
The analysis of the group of patients with any type of solid tumor - ST Group (No=20) - showed a significant decrease in the scores of nausea and appetite loss parameters after supplementation of Selenium (P=.0036 and P=.0208, respectively) and placebo administration (P=.0073 and P=.0469, respectively) compared with the beginning of the treatment. The fatigue parameter showed a significant decrease only during placebo administration (P=.0239). For all the other analyzed parameters, the supplementation of Se or the use of placebo did not determine any significant alteration in patients (Table 4).
Significant alterations (P<.05) in relation to the study.
Parameters quartiles and medians concerning each randomization period (initial, Se, and placebo) and supplementation follow-up during 1 year (initial, D30, D128, and D365) in children and adolescents with solid tumors. Q25: Quartile 25; Q75: Quartile 75.
Supplementation with Se in the ST Group during 1 year (D365) revealed a significant decrease (P=.0289) in the fatigue parameter. As to the other evaluated parameters, there was no significant alteration during the same period (D30, D128, D365). Nevertheless, a decrease in scores for nausea could be observed (Fig. 3). The appetite loss parameter decreased on D30 and then increased throughout the rest of the period (D128 and D365), but the values found in the beginning of the study were never reached. The physical function parameter score in patients from the ST Group increased throughout the year with supplementation.
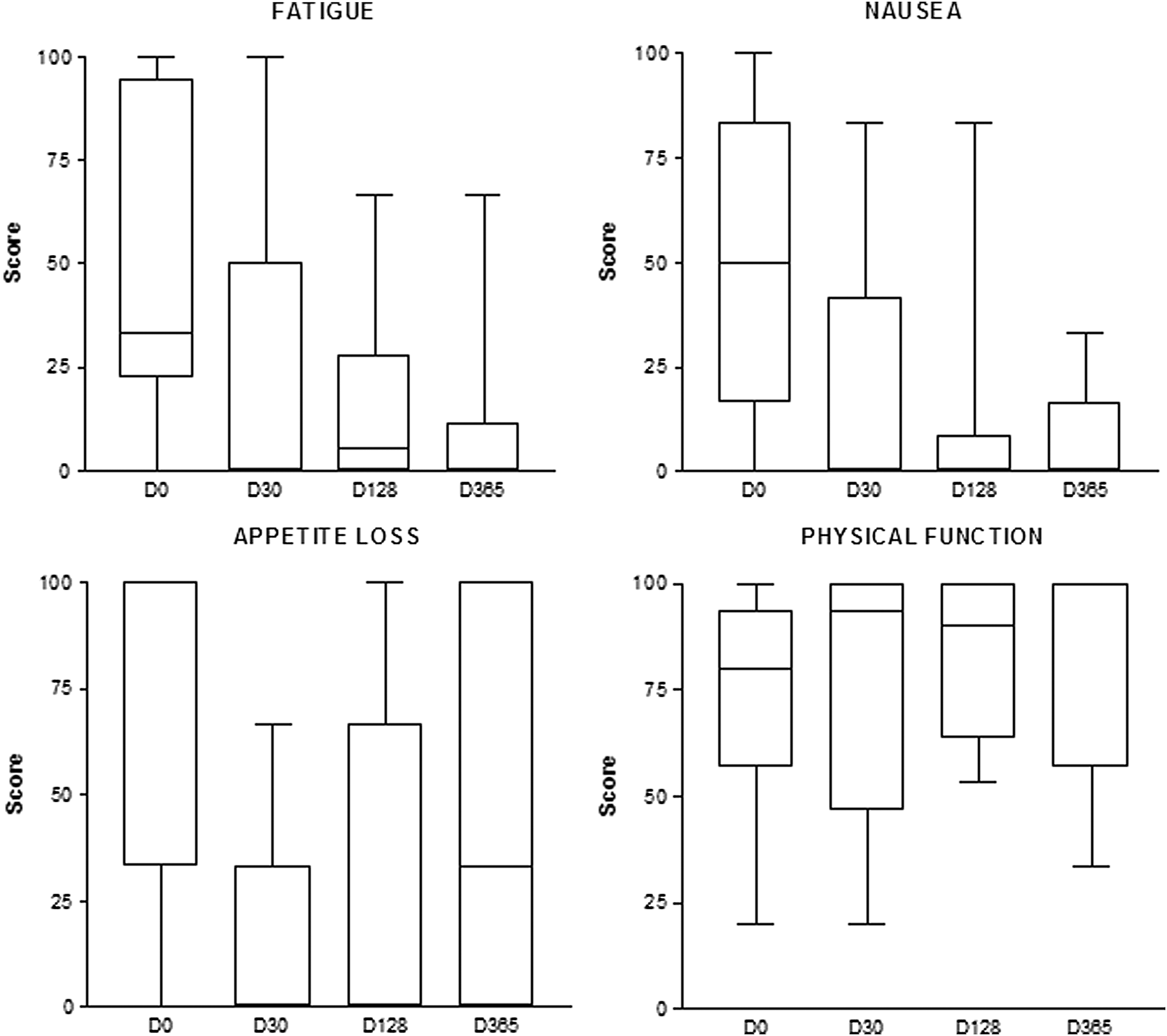
Fatigue, nausea, appetite loss, and physical function scores during the 1-year follow-up of patients with solid tumors who were supplemented with Se.
Hepatic function
When LL and ST serum liver enzymes (AST and ALT) were evaluated, we observed that there was no statistically significant difference after Selenium or placebo supplementation. Nevertheless, Selenium intake provoked AST and ALT decrease in both groups. In the LL patients, serum AST levels were above normal limits in 31.6% (6) and ALT levels in 52.6% (10) of the patients. After Selenium supplementation, the percentage of patients with high AST and ALT enzymes serum levels decreased to: 15.8% (3) and 26.3% (5), respectively. In the ST group, even though AST serum levels were in the normal range both before and after Selenium and placebo supplementation, there was a noticeable decrease in the enzyme levels, as has occurred with LL patients (Fig. 4). During placebo intake, 40% (8) of the ST patients presented ALT serum levels above normal and the percentage decreased to 10% (2) after Selenium supplementation. ALT and AST levels from LL patients were significantly lower than those in the ST group during placebo supplementation (P=.0165 and .0485, respectively). This difference disappeared following the use of Selenium. When all the patients (LL and ST) were evaluated together, there was a noticeable difference during Selenium and placebo supplementation (Table 4): the Selenium administration determined a significant decrease in AST levels (P=.0447). The medians, upper, and lower values are presented in Table 5.

AST, ALT, creatinine, and urea from LL and ST patients after placebo or Selenium supplementation (30 days). Dashed line represents normal value of studied population. AST, aspartate transaminase; ALT, alanine transaminase; Pla, placebo; Se, Selenium; LL, leukemia and lymphoma patients; ST, solid tumor patients.
Significant alterations (P<.05) in relation to the study (P=.0447) - comparison between Selenium and Placebo supplementation. Minimum, maximum, and medians of parameters concerning each randomization period (Se and placebo).
AST, aspartate transaminase; ALT, alanine transaminase; CREA, creatinine; Pla, placebo; Se, selenium; LL, leukemia and lymphoma; ST, solid tumor.
Renal function
The analysis of creatinine serum levels from LL and ST patients revealed that during placebo or Selenium supplementation, there was no statistically significant difference. However, in the LL patients, the above-normal creatinine serum levels decreased to normal values (Fig. 4) after Selenium supplementation: 36.8% of LL patients (n=7) presented serum creatinine levels above normal values during placebo intake, that decreased to 26.3% of LL patients (n=5) during Selenium intake. The ST patients (60%) maintained serum creatinine levels above normal values regardless of the supplementation used (placebo or Selenium).The serum urea levels were above normal values in 10% of the ST patients (2) after placebo intake, and normalized after Selenium supplementation. Despite urea levels being normal at 95% (37) of all the patients (LL and ST) during the placebo cycle, medians decreased after using Selenium (Table 5). After Selenium intake, the serum urea levels from the LL patients were significantly lower than in the ST group (P=.0398). This was not observed after using placebo. The medians, upper, and lower values are presented in Table 5.
Discussion
The essential trace mineral Selenium is of fundamental importance to human health. As a constituent of selenoproteins, Selenium has structural and enzymatic roles, in the latter context being best-known as an antioxidant and catalyst for the production of active thyroid hormone. Selenium is needed for the proper functioning of the immune system and appears to be a key nutrient in counteracting the development of virulence and inhibiting HIV progression to AIDS. 26
Supplementation of Se in patients with leukemias and lymphomas, or ST showed positive results to those undergoing chemo or radiotherapy. It was possible to observe some improvement in most of the parameters in the first 30 days, especially in relation to fatigue, nausea, appetite loss, and physical function. In the long run, after 365 days of supplementations, this improvement was even more relevant (fatigue and physical function).
Sieja and Talerczyk 27 verified similar results when evaluating female patients with ovarian cancer supplemented with 200 μg of Se for 3 months during chemotherapy treatment. The authors observed that those patients showed a significant improvement in the nausea, vomiting, appetite loss, and fatigue parameters when compared with the control group. However, their study differs from ours when we take into consideration the type of tumor, the age group, and the fact that the used doses in our study were much lower.
Moreover, Sieja and Talerczyk 27 used selenium-methionine in their study, whereas we chose to use selenium-glycine. Such a choice was derived from the known fact that methionine increases the risk of thromboembolism in oncologic patients. 28,29 Despite the experimental differences, those authors showed results compatible with ours when they identified that the micronutrient efficacy depends on the length of time for which it is administered.
Emphasizing the supplementation time, we observed a decrease in medians and quartiles in the scores concerning the nausea parameter in both the LL and ST groups, more noticeably in the 1-year follow-up. The significance found in the ST group during randomization was overshadowed due to the fact that it was also observed when the placebo was used. Nausea and vomiting are still very relevant adverse effects of chemotherapy treatments.
According to Hesketh, 30 one of the main pathways of induction of nausea and vomiting in oncologic patients would be the generation of free radicals after the treatment which leads to neurotransmitters release, like 5-HT (5-hydroxytryptamine) and dopamine, by enterochromaffin cells. These neurotransmitters connect with their respective receptors causing vagal stimulation. Once taken to the cerebral trunk, this stimulation reaches the vomit-inducing center, which activates the vomiting reflex. Considering this association between free radicals and the stimulation of nausea and vomiting during the chemotherapy treatment, and as Se is a trace element with antioxidant activity, it is reasonable to speculate that patients who receive supplementation of Se could have a better control over the production and activity of free radicals. Such control would diminish the vagal stimulation and thus reduce the vomiting reflex.
Besides nausea, during the 1-year follow-up, the median and quartile values for appetite loss scores in both groups were reduced only during the first 30 days (D30) of supplementation, but in the subsequent evaluations (D128 and D365) these values increased. Three patients from group LL presented complications (febrile neutropenia–that progressed to erysipelas–and pneumonia) along with the worsening picture in the evaluated parameters or after a change in the chemotherapy protocol. The two patients from the ST group who presented a worsening picture in the appetite loss parameter underwent a radiotherapy treatment and one of them also had a change in the chemotherapy protocol. According to Liberali et al. 31 the effects of radiotherapy depend on various factors like the irradiation location, duration, and the administered dose, and all cases eventually lead to appetite loss among other collateral effects.
On the fatigue parameter, there was no significant alteration in both L and ST groups during supplementation of Se and placebo for 30 days. However, when supplementation of Se was analyzed after 1 year, fatigue in the ST group significantly decreased (P=.0289). The association between Se deficiency and fatigue has been described in patients with long-lasting parenteral nutrition. 32 According to the authors, patients who undergo parenteral nutrition for a long period of time report muscular pain and difficulty to keep their basic motor activities. Considering that myofibrillar edema is associated with the incomplete metabolization of hydrogen peroxide through antioxidant mechanisms, it is possible to connect fatigue improvement in the patients of this study with the reestablishment of the necessary quantity of Se for the mechanisms of Se-dependent antioxidants. Throughout the study period, the physical function parameter had a gradual increase in both groups (LL and ST) during the 1-year supplementation.
Besides the emetic and muscular parameters, we also verified the effects of Se supplementation on liver and renal functions by studying the biochemical evaluations. The oncologic patients usually present kidney and liver function alterations as a consequence of polytherapies, which are highly nephrotoxic and hepatotoxic. 33 –38 The serum creatinine and urea levels above normal values might represent chemotherapy toxicity that affects drug clearance and/or facilitates the accumulation of cell death byproducts. Regarding kidney function, in our study, the response after Selenium intake in the ST patients was worse than in the LL patients. Even with Se supplementation the ST patients maintained serum creatinine levels above normal values, whereas at least 10% of the LL patients had creatinine levels decrease to normal values. In the same cycle, the LL patients had urea levels that decreased significantly when compared with the ST group. These results suggest that complementary treatment through Selenium supplementation is more effective in improving kidney function of patients with LL than of patients with ST.
Corroborating our data, Teodor et al. 39 demonstrated that acrylamide intake, in their experimental model of intoxication, resulted in severe perturbation of some biochemical parameters (liver and kidney function). The authors concluded that simultaneous intake of Selenium, as a dietary supplement, partially prevented renal damage. Salehi et al. 40 demonstrated that Selenium supplementation is capable of improving the nutritional status of hemodialysis patients. The authors attributed the effect produced to the control of the oxidative stress and inflammation involved in the pathogenesis of the disease. Other authors also reported that Selenium protected the kidney from the toxic effect of Cisplatin. 34,40 –42 In summary, as others proposed before, we observed in our study, that Selenium supplementation can be used as a complementary treatment to prevent kidney damage provoked by toxic products and inflammation, as occurs during oncologic treatment.
The clinical importance of Selenium in liver diseases emerged from experimental studies in animals, in which Selenium deficiency was shown to induce liver necrosis. Toxic liver injury can reproduce virtually any known pattern of injury, including necrosis, steatosis, fibrosis, cholestasis, and vascular injury. Liver injury during cancer chemotherapy may not always reflect hepatotoxic anticancer drugs. 43,44 In our study, when all the patients (LL and ST) were evaluated together, ALT serum levels were markedly different during Selenium and placebo supplementation: the ALT levels were significantly lower under Selenium intake. On the other hand, when LL and ST serum liver enzymes (ALT and AST) were evaluated separately, we observed that there was no statistically significant difference after Selenium or placebo supplementation. Nevertheless, in both groups, Selenium intake provoked serum AST and ALT decrease.
In conclusion, although only the fatigue parameter in the ST Group (after 1 year of supplementation) showed a statistically significant difference, it can be observed that Se supplementation enables the reduction of chemotherapy side effects when it comes to the fatigue, nausea, and appetite loss analyses. This is probably connected to the Se antioxidant effect noted especially during the 1-year follow-up, thus showing a time-dependent effect. Besides, in the ST Group, a higher efficacy was observed, probably connected to the inflammatory process triggered by the tumor itself. The suppression of this process is likely to be related to the use of Se.
Finally, our data suggested that it is possible to highlight the beneficial role of the Se supplementation in children and adolescent cancer patients, mainly in regard to the control of fatigue, nausea, appetite loss, liver function, and kidney protection indicating a cytoprotective and immunoregulatory effect, especially in the long run (1 year of supplementation). Moreover, more studies are recommended to establish the influence on the use of Se and the evolution of tumors without the interference of chemotherapeutic agents.
Footnotes
Acknowledgments
The authors thank the staff of the Pediatric Oncology of ABC Medical School for their support during the execution of the project study and for the support of the Association of Volunteers to Cancer Combat (AVCC).
Author Disclosure Statement
The authors declare that no competing financial interests exist.