
Abstract
Menopause leads to an increased risk for osteoporosis in women. Although drug therapies exist, increasing numbers of people prefer alternative therapies such as dietary supplements, for example, calcium, vitamin D, and collagen hydrolysates for the prevention and treatment of osteoporosis. We have previously shown that a 3-month intervention using a calcium-collagen chelate (CC) dietary supplement was efficacious in improving bone mineral density (BMD) and blood biomarkers of bone turnover in osteopenic postmenopausal women. This study reports the long-term efficacy of CC in reducing bone loss in postmenopausal women with osteopenia. Thirty-nine women were randomly assigned to one of two groups: 5 g of CC containing 500 mg of elemental calcium and 200 IU vitamin D (1,25-dihydroxyvitamin D3) or control (500 mg of calcium and 200 IU vitamin D) daily for 12 months. Total body, lumbar, and hip BMD were evaluated at baseline, 6 and 12 months using dual-energy X-ray absorptiometry. Blood was collected at baseline, 6 and 12 months to assess levels of blood biomarkers of bone turnover. Intent-to-treat (ITT) analysis was performed using repeated measures analysis of variance pairwise comparisons and multivariate analysis to assess time and group interactions. The loss of whole body BMD in women taking CC was substantially lower than that of the control group at 12 months in those who completed the study and the ITT analysis, respectively (CC: −1.33% and −0.33% vs. control: −3.75% and −2.17%; P=.026, P=.035). The CC group had significantly reduced levels of sclerostin and tartrate-resistant acid phosphatase isoform 5b (TRAP5b) (P<.05), and higher bone-specific alkaline phosphatase/TRAP5b ratio (P<.05) than control at 6 months. These results support the use of CC in reducing bone loss in osteopenic postmenopausal women.
Introduction
O
Among the dietary supplements, hydrolyzed collagen is promising with respect to bone. Collagen, specifically type I collagen, is one of the major protein components of bone and is the main extracellular matrix protein that is calcified. 9 The loss of collagen therefore leads to bone loss and a subsequent decline in bone strength and elasticity thereby increasing the risk of fragility fractures. 10,11 Collagen hydrolysates have been shown to provide bioavailable collagen-derived peptides following oral ingestion. 12 Furthermore, dietary collagen-derived peptides of low molecular weight have been shown to remain intact following absorption, contributing to the organic substance of bone, 13 and thus are able to exert beneficial effects in skeletal tissues. In fact, oral administration of collagen exerts osteoprotective effects as shown in preclinical 14 –17 and some clinical studies. 18,19 We previously reported 20 the findings of our 3-month clinical pilot study in which the efficacy of a calcium-collagen chelate (CC) supplement was demonstrated to improve bone mineral density (BMD) and shift the rate of bone formation to exceed that of bone resorption in postmenopausal women with osteopenia. We carried out a 1-year study to evaluate its long-term efficacy in modulating bone mass. Thus, the formulated hypothesis was that 1 year of dietary supplementation with CC would reverse or prevent the significant reduction of bone mass and favorably alter systemic concentrations of blood biomarkers of bone turnover. The findings of this study support the notion that regular intake of CC can be used as an adjunctive therapy in preventing bone loss in postmenopausal women.
Materials and Methods
Subjects
A total of 112 postmenopausal women were screened and recruited from the greater Tallahassee, FL and surrounding areas using flyers and radio and online listings. All participants were 1–10 years postmenopausal, had not received hormone replacement therapy for at least 3 months prior to initiation of the study, and had a lumbar spine BMD T-score between −1.0 and −2.5. The following exclusion criteria were used: the use of calcitonin, bisphosphonates, raloxifene and/or anabolic agents such as parathyroid hormone and growth hormone, or steroids for less than 3 months prior to the start of the study, being diagnosed as having cancer, diabetes mellitus, metabolic bone, renal, cardiovascular, respiratory, gastrointestinal, liver diseases, or other chronic diseases, heavy smoking (≥20 cigarettes per day), and current use of any prescription medications known to alter bone and calcium metabolism. The study protocol was approved by the Human Subjects Committee of the Institutional Review Board at Florida State University (FSU). Before the start of baseline, qualified subjects were invited to the research laboratories of FSU's Department of Nutrition, Food, and Exercise Sciences where written informed consent and complete medical history were obtained. All subjects were advised to maintain their usual physical activity and diet pattern throughout the duration of the study.
Study design
The study was carried out in a randomized, double-blind placebo-controlled manner. Thirty-nine women with a mean age of 55.7±3.3 (mean±standard deviation [SD]) completed all time points of the study up to 6 months. Twenty-two women with a mean age of 56.2±4.0 (mean±SD) completed all time points of the study up to 12 months. This information is presented in Figure 1. Those in the control group received 500 mg calcium and 200 IU of vitamin D (1,25-dihydroxyvitamin D3) daily as a placebo dietary supplement. The CC group received a proprietary hydrolyzed collagen calcium chelate (5 g) that contains 500 mg of elemental calcium and 200 IU of vitamin D daily. Both groups were instructed to consume four supplement pills twice daily in the morning and evening. Subject compliance was monitored via the following means: (1) Study participants were asked to return any remaining capsules of CC, control, and unused calcium/vitamin D pills at their follow-up visits; (2) Each individual was contacted via telephone on random dates to encourage compliance; and (3) Study participants were provided with customized calendar to record how many CC, control, and calcium/vitamin D pills were consumed.

Study flowchart. CC, calcium-collagen chelate; G.I., gastrointestinal.
Anthropometric measurements
Height without shoes was measured to the nearest 0.5 cm using a wall-mounted stadiometer and weight was assessed to the nearest 0.1 kg using a digital scale (Seca Corporation, Hanover, MD, USA). Body mass index was calculated as kg/m2. Height was measured at baseline and body weight was measured at each time point of the study.
Bone density assessments
Changes in bone density were assessed at the baseline, 6, and 12-month time points using dual energy X-ray absorptiometry (iDXA; GE Healthcare Lunar, Madison, WI, USA) equipped with appropriate software for total body, lumbar spine (L1–L4), and hip BMD. Densitometer stability was evaluated by performance of phantom scans on the dates of all data acquisition.
Blood collection and bone biomarker measurements
After an overnight fast, a venous blood sample (20 mL) was obtained from each subject between 8:00AM and 10:00AM at baseline, 6-, and 12-month time points for the analysis of blood biomarkers. Within 2 h of collection, blood samples were centrifuged at 3500 g for 15 min at 4°C, and serum samples were separated, aliquoted, and stored at −80°C until analyses. For the following bone marker assays, all samples from each time-point were measured in duplicate on the same day.
Serum bone-specific alkaline phosphatase (BAP), a marker of bone formation, was assessed using a direct capture enzyme-linked immunosorbent assay (ELISA) (MicroVue; Quidel Biosystems, Mountain View, CA, USA) following the manufacturer's instructions. Briefly, 20 μL of each sample was added to a monoclonal anti-BAP antibody coated 96-well plate. The substrate to catalyze the reaction was p-Nitrophenyl phosphate. The optical density was read at a wavelength of 405 nm. The reference values and limit of detection (LoD) for BAP were 14.2–42.7 and 0.7 U/L, respectively. Intraassay and interassay coefficients of variation were 2.0% and 3.2%.
Tartrate-resistant acid phosphatase isoform 5b (TRAP5b), a marker of bone resorption, was measured in serum using direct ELISA (MicroVue; Quidel Biosystems), following the manufacturer's instructions. Briefly, Tris buffer (100 μL) and 50 μL of undiluted sample were pipetted to the wells of a monoclonal anti-TRAP5b antibody coated 96-well plate. The plate was incubated while shaking for 1 h at 25°C. Following a 3×wash, 100 μL of 2-chloro-4-nitrophenyl-phosphate was added to each well for incubation (1 h at 37°C). The optical density was read at a wavelength of 405 nm. The reference values and LoD were 4.3±1.5 and 0.2 U/L, respectively. Intraassay and interassay coefficients of variation were 3.0% and 4.5%.
Sclerostin is an osteocyte-derived protein associated with significant increases in markers of bone turnover and decreased bone formation. 21 –23 Serum levels were measured using a direct-capture format ELISA (TECOmedical; Quidel Corporation, San Diego, CA, USA), following the manufacturer's instructions. Briefly, 25 μL of serum was loaded to each streptavidin and polyclonal antibody-coated assay well and incubated for 5 min with shaking followed by 24 h of incubation at 4°C. The optical density was read at 450 nm with a reference wavelength of 590 nm. The reference value and LoD for sclerostin were 0.69±0.20 and 0.015 ng/mL, respectively. Intraassay and interassay coefficients of variation were 5.1% and 6.3%.
Statistical analyses
Data were analyzed using SPSS Statistics software (Version 21.0; SPSS, Inc., Chicago, IL, USA). Independent samples t-test was used to compare mean differences between groups for baseline characteristics. Repeated measures analysis of variance (ANOVA) was used to analyze the time (baseline, 6, and 12 months) and treatment interaction effects for each treatment (control or CC) with statistical significance regarded as P≤.05. For those comparisons that reached significance, post hoc Bonferonni tests were performed for pairwise comparisons. Data are reported as mean±SD. Mean changes and percent changes were compared for significant differences using independent samples t-tests.
An intent-to-treat (ITT) analysis was used to evaluate measures at each time point to assess effects of the supplement on the subjects regardless of whether or not they completed the study. Using the statistical approach last observation carried forward data collected from subjects or measured at the time closest to dropout were used to fill any missing values. All but one dropout occurred between 6 and 12 month time points, thus data collected at 6 months were used for the subject's 1 year values. Secondary analyses were carried out to assess the efficacy of the supplement for those subjects who completed the study. Values for subjects that were 2.33 SD above or below the mean were considered outliers and were excluded prior to performing the secondary analyses.
Results
Baseline characteristics and level of compliance
The attrition rates for the CC and control groups were 5% and 0% from baseline to 6-months and 37% and 53% from 6- to 12-months, respectively. Common reasons for not finishing the study included noncompliance with the study protocol, claims of medical and health-related issues such as constipation, and personal reasons such as lack of time. The 22 participants who completed the study were compliant with their treatments as indicated in their self-monitoring checklists. Baseline characteristic data for subjects who completed the study are presented in Table 1. None of the subject baseline characteristics were statistically different between groups.
Data are presented as mean±SD. No significant difference (P≤.05) between groups was observed for any variables. For the control group, n=19; for the CC group, n=20.
CC, calcium-collagen chelate; SD, standard deviation.
Effect of CC on serum biomarkers of bone metabolism
Mean serum concentrations of biomarkers of bone metabolism, BAP, TRAP5b, and sclerostin were assessed and are presented in Tables 2 and 3. BAP concentrations were not significantly different at any time point between groups or on a time wise basis in either analysis (Tables 2 and 3). In the ITT analysis, serum concentrations of TRAP5b were significantly lower at 6 months (P=.046) but not 12 months (P=1.000) from baseline in the CC group. For those who completed the study (Table 3), the decrease from baseline at 6 months was not significant (P=.425); however, mean values for TRAP5b were different (P=.009) between groups at 12 months. With regard to sclerostin, in the ITT analysis a trend (P=.083) for decreased concentrations was observed in the CC group at 6 months, but not at 12 months (P=.334). Neither in the ITT analysis nor in those who completed the study were there significant differences in serum sclerostin between groups. The ratio of bone formation and resorption (BAP/TRAP5b) was significantly higher in the CC group than that of control group at 6 months (P=.029; Table 2) in the ITT analysis and at 12 months in the analysis of those who completed the study (P=.001), and tended to be higher at 12 months (P=.061) in the ITT analysis (Table 2).
The values shown are mean±SD. Sample sizes are based on the inclusion of all subjects at baseline for the purpose of the intent-to-treat analysis; control group, n=19; CC group, n=20.
Statistical significance between groups (P≤.05).
A significant difference (P≤.05) from that time point from baseline.
BAP, bone-specific alkaline phosphatase; BMD, bone mineral density; TRAP5b, tartrate-resistant acid phosphatase isoform 5b.
The values shown are mean±SD.
Statistical significance between groups (P<.05).
A significant difference (P<.05) of that time point from baseline.
Mean differences and percent differences were not statistically different for BAP, TRAP5b, sclerostin, or BAP/TRAP5b ratio in the ITT analysis or for those who completed the study (data not shown). However, a trend toward statistical significance (Control: −0.57±3.34 vs. CC: 2.37±6.11, P=.07) was observed with regard to the 6-month mean BAP/TRAP5b ratio differences in the ITT analysis.
Effect of CC on BMD
Mean BMD measures are shown in Tables 2 and 3. No significant time effect was found as a result of CC supplementation with regard to L1–L4 vertebrae, total hip, or total body BMD measures. In contrast, at 12 months, the control group was found to have significant decreases in vertebral (P=.029) and total body (P=.002) BMD for those who completed the study and in total body BMD (P=.005) for the ITT analysis. In relation to the control group, mean total hip BMD values were significantly (P<.05) larger at each time point; however, no change from baseline to final was noted in either group.
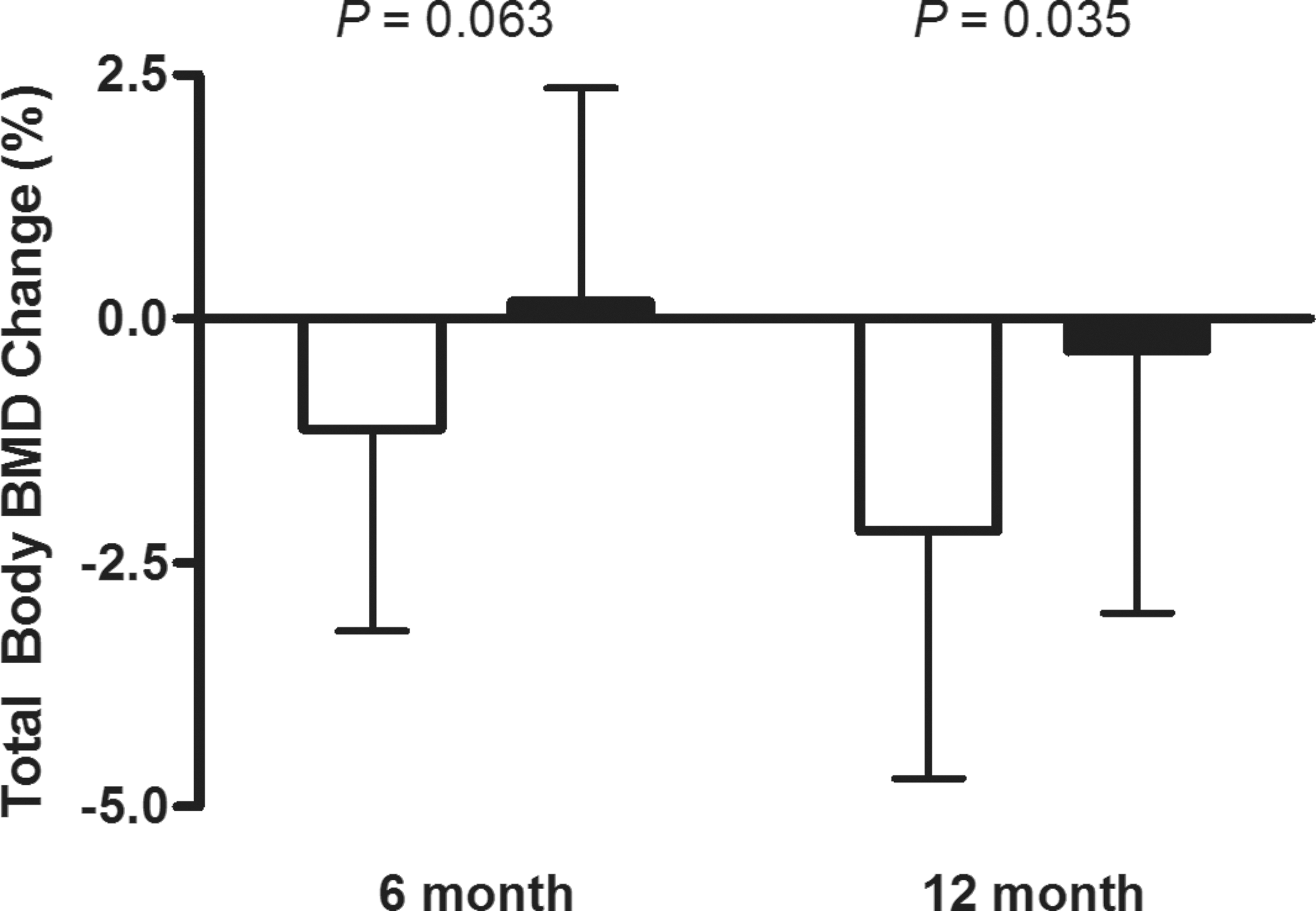
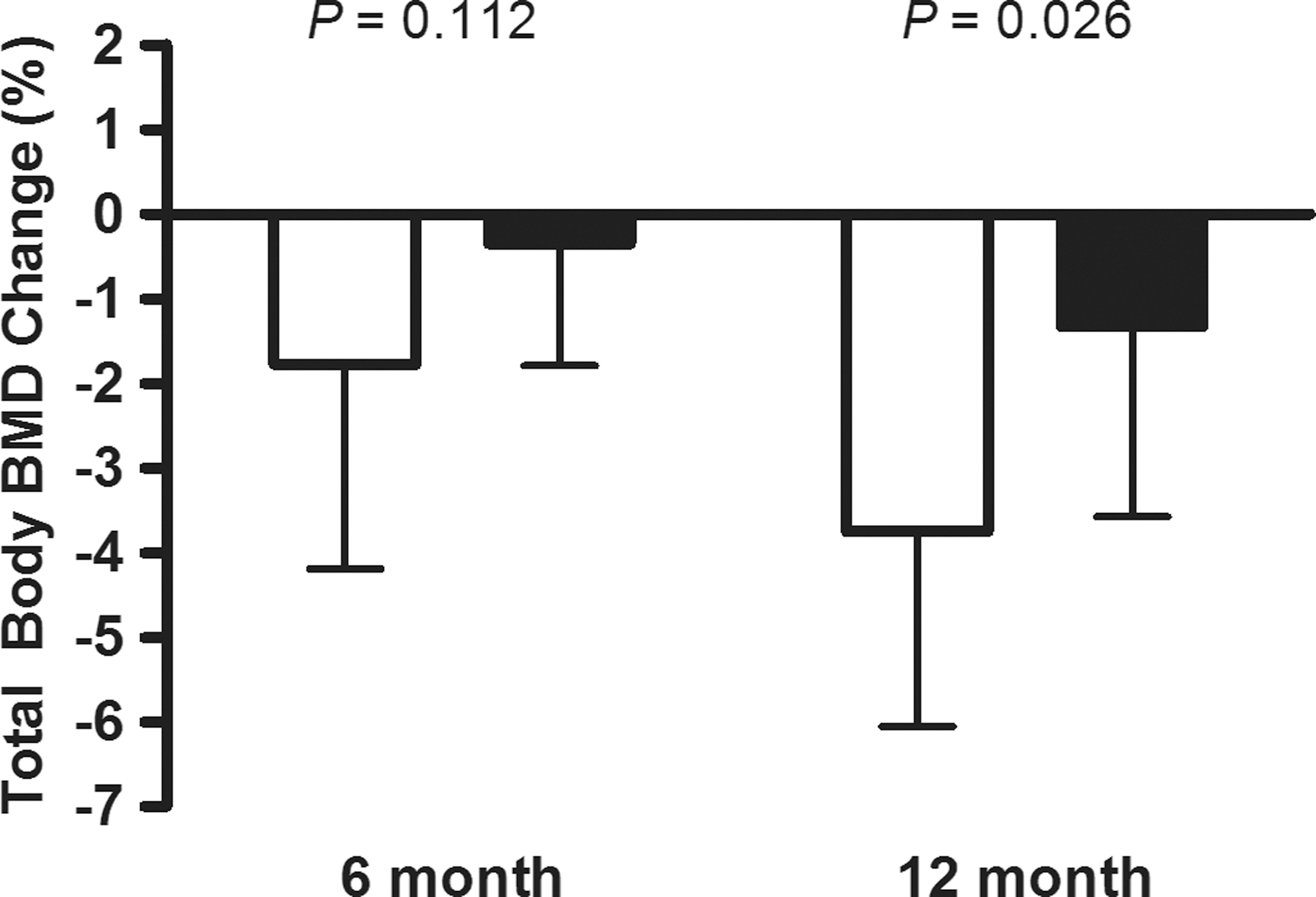
For the ITT and secondary analyses, mean total body BMD differences and percent changes were significantly different between groups at 12 months in favor of the CC supplement (Figs. 2 and 3). No other significant differences between groups were found with regard to changes in BMD (data not shown).
Total body BMD percent change at 6 and 12 months of treatment with the CC for the intent-to-treat analysis. Means of percent changes (mean±SD) shown and compared using an independent samples t-test with P-values presented. Statistical significance set at P≤.05. BMD, bone mineral density; SD, standard deviation.
Total body BMD percent change at 6 and 12 months of treatment with the CC in those who completed all 12 months. Means of percent changes (mean±SD) shown and compared using an independent samples t-test with P-values presented. Statistical significance set at P≤.05.
Discussion
To our knowledge, this is the longest clinical trial investigating the efficacy of a collagen hydrolysate supplement in preventing and/or reversing bone loss in postmenopausal women to date. During menopause, which is characterized by dramatic alterations in bone metabolism, 24 any reduction or preventive effect on bone loss is highly desired. The findings of this study are in agreement with our earlier feasibility study 20 in which we reported that CC favorably altered bone metabolism and decreased the rate of bone loss by tilting the ratio between bone formation over bone resorption. Furthermore, the significantly lower reduction in BMD in those supplemented with CC is further indication that hydrolyzed collagen-based supplements can be beneficial for osteopenic populations.
Though our findings were in agreement with the outcomes of past studies in children 19 and animals, 25,26 when pertaining to postmenopausal women with significant bone loss, only two other investigations have been reported. 18,27 Cúneo et al. 27 gave 10 g/day of a collagen hydrolysate preparation to postmenopausal women for a 6-month period. In their study, changes in BMD were not assessed, and the biochemical analysis of bone biomarkers, that is, BAP, C-telopeptide (CTx), and osteocalcin, indicated no improvements in bone metabolism in comparison with the controls. However, the authors noted the subjects' poor calcium intake and excessive body weight, which may have influenced the outcome of their study. These results are in contrast to those of our studies. In another clinical trial, Adam et al. 18 documented the bone protective effects of dietary pharmaceutical-grade hydrolyzed collagen (PHC) in osteopenic postmenopausal women in which a combination of the supplement (10 g/day of PHC) and calcitonin (100 IU twice/week) elicited a greater reduction (P<.05) in urinary cross-link excretion than with calcitonin alone after 6 months. Nonetheless, results of the densitometry of the forearm indicated no effect. Thus, the results of this study are important in that multiple sites of BMD were assessed and provide support for the use of enzymatically hydrolyzed collagen as a supplement for reducing bone loss, particularly when given with calcium in a chelated form.
At the end of the 1-year study there were significant differences between CC and the control group in terms of percent changes in total body BMD, signifying the efficacy of CC to reduce bone loss due to ovarian hormone deficiency. We should also emphasize the contrasting within-group differences in bone parameters such as the total body and lumbar, which excluding the hip, were not significantly altered. Conversely, in the control group, calcium and vitamin D supplementation alone led to a reverse effect, indicating the preventive effect of CC on the loss of bone. Similar outcomes have also been observed with the use of common osteoprotective drugs and calcium carbonate supplements. 28,29 However, calcium supplementation itself tends to be less efficacious for maintaining BMD in early menopausal women compared to those in latter stages. 30
The measure of TRAP5b, an enzyme specific to bone resorption activity of osteoclasts, 31 adequately detects alterations in bone degradation. 32 The significant decreases in TRAP5b that occurred at 6 months are similar to other modalities for bone loss in this population. One such observation was reported by Bonjour et al. 33 where in a 6-week randomized control trial, calcium and vitamin D-fortified white cheese, and calcium and vitamin D alone significantly (P<.0001 and P<.008, respectively) lowered TRAP5b concentrations. In that study, percent changes were approximately −5.5% (control) and −11% (experimental), demonstrating lesser, yet analogous results to that of the current study at a later time point. The same effect was found when older women consumed calcium and vitamin D-fortified yogurt daily for 8 weeks. 34 Though in this study concentrations of TRAP5b did increase at final from baseline and 6 months, the inhibiting effect on osteoclastic activity appears evident as indicated by higher values (P<.05) in control subjects who completed the study (Table 3). A similar outcome was also reported in a 4-month study examining the effect of a hydrolyzed collagen dietary supplement in prepubescent children. 19 They found up to an approximate 1.5 U/L reduction in serum TRAP5b with an increasing dose of collagen (up to ∼0.2% of body weight). Based on these data, CC and formulations alike may serve as an effective adjunctive therapy for decreasing bone resorption. In this study, since both groups received the same level of calcium and vitamin D, this signifies a beneficial effect from the collagen component of CC.
Serum sclerostin concentrations are commonly correlated with greater BMD 22,35,36 in postmenopausal women. However, other reports 37,38 have shown significant negative correlations between BMD and serum sclerostin. In agreement with these studies, and consistent with our previous findings 20 the CC group, who tended to have higher BMD measures, sustained lower concentrations of sclerostin compared with that of control subjects throughout the study. Additionally, serum BAP and TRAP5b concentrations have been shown to decrease and increase, respectively, with rises in sclerostin, 21,39 which suggests the negative effect of sclerostin on bone formation. When coupled with the stable BAP concentrations, which is in contrast to the controls and a trend for lower serum sclerostin in the CC group at 6 months, the differences between groups in regards to BMD and BAP, an indicator of osteoblast activity, may be explained. Hence, the authors suggest that CC may prevent bone loss, in part, through downregulation of sclerostin, which signals the activation of osteoblast apoptosis. 40
In this study and other dietary supplement studies related to bone, 41 –43 the ratio of bone formation to resorption biomarkers (BAP/TRAP5b) has been used to represent the state of bone turnover. An increased BAP/TRAP5b ratio indicates either more bone formation or less bone resorption, while a decreased ratio is representative of the exact contrasting effect as a result of the intervention. The significant difference in the BAP/TRAP5b ratio between groups at 6 months denotes an improvement in bone turnover in favor of bone formation resulting from CC supplementation, which is unlike calcium alone. Similarly, in postmenopausal women practicing Tai Chi and consuming green tea as a treatment, 43 the mean BAP/TRAP5b ratio (relative to baseline) rose and peaked (P<.05) after 3 months of treatment. However, after 6 months, the ratio began to decline, though still significantly greater than that of baseline values. This study was twice as long in duration as the aforementioned study, yet the mean BAP/TRAP5b ratio (% change) was elevated at 6 months and began to decrease up to 1 year. This outcome corresponds to the absence of an increase, or a minute, steady decrease in bone density that was observed.
In terms of mechanisms of action, CC may play a role in downregulating the production of pro-inflammatory molecules that are implicated in the development of osteoporosis, in part, as a result of ovarian hormone deficiency. 44 Although we did not examine the effect of CC on markers of inflammation, Han et al. 16 noted a suppressive effect of bone gelatin on pro-inflammatory cytokines such as interleukins-1β and −6, and tumor necrosis factor-α in ovariectomized rats. Because these cytokines in particular are responsible for upregulation of receptor activator for nuclear factor kappa-B ligand (RANKL) for osteoclast recruitment, 45 this may explain the noteworthy impairment of bone loss seen in the CC group. In ovariectomized rats, 0.375–6 g/kg of bone gelatin downregulated RANKL while having no effect on the gene expression of osteoprotegerin, the endogenous antibody of RANKL. 16 Thus, it is possible that CC and similar hydrolyzed collagen formulations reduce the production of pro-inflammatory cytokines that promote osteoclast activity through the activation of RANKL.
In addition, it was suggested from the results of a study in C3H/HeN mice that hydrolyzed collagen reduces osteoclast differentiation but not osteoclast proliferation while also stimulating osteoblast activity, 14 further supporting this postulate. Other researchers 25,46 have recently demonstrated that collagen hydrolysates may be bone-protective through mitogen-activated protein kinase signaling for promoting osteoblast proliferation and differentiation. Finally, CC may also serve as an effective supplement for preventing bone loss by significantly enhancing the organic substance content of bone, a suggested attribute of hydrolyzed collagen, specifically that of low molecular weight. 13 It is possible that hydoxyproline-containing peptides like proline-hydroxyproline stay intact through the gastrointestinal tract following digestion to allow for interaction with bone collagen matrices. 47,48 Nonetheless, future studies are needed to fully elucidate these potential mechanisms.
We conclude that CC supplementation may provide protection against excessive bone loss and turnover for which supplementation of calcium and vitamin D alone could not prevent. Based on our 3-month study results 20 and current findings, it can be suggested that the CC supplement improves bone health in terms of density and biomarkers of bone turnover. Results of this study are of great interest as a shortage exists for studies undertaken to examine the benefits of collagen hydrolysate supplements in clinical trials, which are most relevant to humans. However, further research is needed to identify whether lower doses of CC would have the same effect.
Footnotes
Acknowledgments
The funding and calcium-collagen chelate supplement (KoAct™) were provided by AIDP, Inc. (City of Industry, CA, USA). The authors would like to thank Jenna Browne, Jiyao Zhang, and Lauren T. Ormsbee for their contributions to subject recruitment and coordination of the study.
Author Disclosure Statement
Jennifer Gu is an employee of AIDP. No competing financial interests exist for the other authors.