
Abstract
This study was a randomized, double-blind placebo-controlled trial to assess the efficacy of 4 weeks of mulberry leaf aqueous extract (MLAE) supplementation (5 g/day) for postprandial glycemic control in 36 subjects with impaired fasting glucose (IFG) tolerance. Postprandial responses in the glucose, insulin, and C-peptide levels were measured after a carbohydrate load both at baseline and after 4 weeks of MLAE supplementation. The postprandial glycemic response was attenuated in the MLAE group after the treatment period, particularly 30 and 60 min after loading (P=.003 and 0.0325 for glucose, P=.0005 and .0350 for insulin, and P=.0151 and .0864 for C-peptide). Additionally, the incremental area under the curve for insulin was significantly lower in the MLAE group than in the placebo group (P=.0207). Four weeks of MLAE supplementation improved postprandial glycemic control in individuals with IFG tolerance.
Introduction
E
According to compelling evidence accumulated over the last 20 years, elevated postprandial glucose values, even in the high nondiabetic impaired glucose tolerance (impaired fasting glucose [IFG]) range, contribute to an approximately threefold increase in the risk of developing coronary heart disease or other major adverse cardiovascular events. 10,11 Improved postprandial glycemic control is therefore the most promising approach to decreasing the mortality associated with cardiovascular disease in individuals with prediabetes and diabetes.
α-Glucosidases in the brush border of the small intestine are competitively inhibited by the pseudo-carbohydrates—acarbose, voglibose, and miglitol. The inhibition delays the digestion of complex carbohydrates in the upper and small bowel, subsequently retarding glucose absorption and blunting postprandial hyperglycemia. 12 In Asian countries, diabetes symptoms have been traditionally treated with mulberry leaves. This effect has been regarded as experimental proof of the presence of iminosugars, such as 1-deoxynojirimycin (DNJ), N-methyl-DNJ, and 2-O-α-galactopyranosyl-DNJ, in the mulberry leaf. Of all iminosugars, the DNJ group (the most abundant, accounting for 50% of all iminosugars) appears to have received the most attention. 13
Mulberry leaf extract has also been shown to inhibit α-glucosidase and to cause a hypoglycemic effect in normal and diabetic rats. 14 –17 Additionally, mulberries contain various functional ingredients besides DNJ, such as soluble dietary fibers, resveratrol, quercetin, rutin, astragalin, and γ-aminobutyric acid. 18,19 Thus, the mulberry leaf may be a promising functional ingredient for hyperglycemic agents.
Previous studies completed in our laboratory have shown that mulberry leaf aqueous extract (MLAE) standardized with DNJ at 3.6 mg/g causes a more potent hypoglycemic effect than the equivalent amount of DNJ alone, and that this effect is mediated by inhibition of glucose uptake at the intestinal brush border membrane and by inhibition of α-glucosidase in the intestinal lumen. 20 MLAE ameliorated insulin sensitivity in high-fat or high-sucrose, diet-induced obese rats. 21 More recently, in a preliminary human study, intake of 5 g of MLAE was found to dampen the postprandial glucose response in healthy volunteers. 22 Apart from the results of MLAE, there are several studies demonstrating the hypoglycemic effect of ethanol extract of mulberry leaf in subjects with prediabetes. 23 –25 Clinical trials have reported on acute postprandial glucose control or presented results for fasting blood glucose (FBG) levels during several weeks of supplementation. Therefore, evidence for postprandial glucose control with long-term supplementation is needed to substantiate the daily use of MLAE as a functional food or food supplement for individuals with prediabetes.
In the present study, as part of a continuing effort to ascertain whether MLAE improves postprandial glucose responses by increasing insulin sensitivity, we conducted a double-blind, randomized placebo-controlled trial in subjects with impaired FBG levels.
Materials and Methods
Preparation of test materials
The MLAE and color-matched placebo (lactose) tablets were prepared at the Jeonnam Biofood Technology Center (Naju, Jeonnam, Korea). The MLAE was prepared from dried mulberry leaves and was standardized to 3.6 mg/g of DNJ. Briefly, dry mulberry leaves were extracted with water for 1 h and then centrifuged at 12,000 g for 15 min to remove insoluble substances. The supernatant was freeze-dried. The DNJ was analyzed using a reversed-phase high-performance liquid chromatography system (RP-HPLC; Shiseido Co. Ltd., Tokyo, Japan) equipped with a fluorescence detector after derivatization with 9-fluorenylmethyl chloroformate (FMOC-Cl) according to the procedure of Kim et al. 26 Ten microliters of standard or sample solution was mixed with 10 μL of 0.4 M potassium borate buffer (pH 8.5) in a 1.5-mL microtube. Twenty microliters of 5 mM FMOC-Cl in CH3CN was added with immediate mixing and allowed to react at 20°C for 20 min. Ten microliters of 0.1 M glycine was added to terminate the reaction by quenching the remaining FMOC-Cl. The mixture was diluted with 0.1% aqueous acetic acid to stabilize the DNJ-FMOC and then filtered. The filtrate was injected into the RP-HPLC using a Unison US-C18 column (250×4.60 mm ID, 5 μm; Imtakt, Kyoto, Japan) with a flow rate of 1.0 mL/min and a fluorescence detector (excitation 254 nm, emission 322 nm). The analyte was eluted with a mobile phase of acetonitrile–0.1% aqueous acetic acid (1:1, v/v).
The MLAE was also characterized as containing various phytochemicals (listed in Table 1) using 15 Tesla Fourier transform ion cyclotron resonance mass spectrometry (FT-ICR MS) (lab-built at the Korea Basic Science Institute, Daejeon, Korea). We confirmed that the contents of DNJ and other specifications were in the safe ranges until 1 year at room temperature in the dark place (data not shown).
Subjects
Subjects were recruited from the health examination center of the CHA Bundang Medical Center. The following inclusion criteria were applied: FBG in the range of 100–125 mg/dL (at the screening visit in the 2 weeks before the intervention began), but normal hemoglobin A1c (HbA1c) values (<6.5%); aged 20–65 years; no consumption of herbal medicines for at least the previous 3 months. Patients were excluded from the trial if they had severe cardiac, hepatic, or renal function impairment, if they were pregnant or lactating, and if they used any drugs or supplements that could affect their blood glucose or lipid metabolism. Individuals who participated in weight reduction programs or had alcohol abuse problems were also excluded. Finally, subjects were excluded from the analysis if their FBG or HbA1c was not eligible at the beginning of the study (at week 0). A total of 67 subjects were recruited, and 42 subjects who were initially eligible were included in the study after providing their written informed consent to participate in the trial. Ethics approval for this trial was obtained from the Institutional Review Board (IRB) of Ewha Womans University (IRB No. 2011-6-14, Seoul, Korea) and the IRB of CHA Bundang Medical Center (IRB No. BD2010-122D, Seongnam, Korea). This clinical trial is registered with
Study design
A double-blind, randomized placebo-controlled design was conducted in two phases: a 2-week run-in period and a 4-week intervention phase. After the run-in period, the subjects were randomized to receive either MLAE (n=21) or a placebo (n=21). The randomization code was prepared by a staff member, who was not involved in running the trial, by using computer-generated random numbers. The group allocation was blinded for both investigators and participants. The principal investigator was provided with a sealed envelope for each subject that was to be opened only after entering all data into the computer or in a medical emergency. Allocation concealment was maintained successfully as no sealed envelope was opened voluntarily or accidently during the study.
At the beginning of the study, each subject received a pack of test material and was asked to take 6 tablets with each meal, for a daily total of 18 tablets (5 g MLAE). The MLAE and placebo were identically packaged to be indistinguishable. During the study period, the subjects were asked to maintain their regular diets and lifestyles and to avoid foods high in antioxidants and whole grains. The subjects were contacted weekly to evaluate the intervention compliance and to inquire about possible side effects. Three-day food records, including 2 weekdays and 1 weekend day, were collected at baseline and again after 4 weeks to monitor dietary compliance and to assess nutrient intakes using the Computer Aided Nutritional analysis program (CAN-pro 3.0; Korean Nutrition Society, Seoul, Korea). The participants were instructed to consume a meal of their own choosing the evening before each visit. At the beginning, and the end of the study, the participants consumed a high-carbohydrate meal in the morning, followed within 15 min by either MLAE or a placebo. The high-carbohydrate meal consisted of 76 g of white bread and 24 g of strawberry jam. The high-carbohydrate meal was calculated to contain 407 kcal, 80 g of carbohydrate (30 g of added sugar), 8 g of protein, and 9.7 g of fat using the Computer Aided Nutritional analysis program.
Outcome measures
Venous blood samples were obtained during fasting (t=0) and 30, 60, and 120 min after consuming a high-carbohydrate meal with MLAE or a placebo. The plasma samples were separated and frozen at −80°C until being analyzed to determine the levels of glucose, insulin, C-peptide, HbA1c, and other blood parameters. HbA1c was measured using HPLC (Bio-Rad Variant II; Bio-Rad Laboratories, Hercules, CA, USA). The plasma glucose concentration was measured using hexokinase with the G-6-phosphate dehydrogenase enzyme method (Wako Pure Chemical Industries, Ltd., Osaka, Japan). Plasma insulin and C-peptide were determined using a chemiluminescent immunoassay (Siemens, Munich, Germany).
Statistical analyses
All statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC, USA). Assuming a 20% dropout rate among the cases, the sample size was estimated at 21 subjects per group to provide a power 80% to detect a difference in the postprandial glucose level at 30 min as the primary outcome of interest between the two groups, which is in agreement with our previous preliminary human study, 22 with an α-level of 0.05. The normality of each variable was determined before statistical testing, and logarithmic transformation was performed on skewed variables. Baseline characteristics were tested for intergroup comparisons using Student's t-test or chi-square test. The incremental area under the curve (AUC) for each postprandial variable was calculated by the trapezium rule. 28 The postprandial blood glucose, insulin, and C-peptide time series data for each subject were normalized to the respective t=0 baseline value before the mean values were computed. The intergroup comparisons were analyzed using repeated measures and endpoint analysis of covariance (ANCOVA), with baseline levels as the covariate, followed by post hoc Duncan's multiple comparison tests. Subsequently, a one-way analysis of variance (ANOVA) was used for testing at individual time points and summary measures, such as the AUC, peak time, and peak height, with post hoc Duncan's multiple comparison tests. For descriptive purposes, the mean values of the untransformed and unadjusted variables are presented as the mean±standard deviation. A two-tailed P<.05 was considered to be statistically significant.
Results
From 67 screenings, 42 IFG subjects were enrolled. Fifteen subjects were ineligible for the study, and 10 subjects withdrew their consent because they had difficulty participating in this trial. The subjects consumed 5 g of standardized MLAE (3.6 mg/g of DNJ) or placebo per day with a meal for 4 weeks. Among the 42 subjects, 2 withdrew for personal reasons during the trial. The data for two subjects were excluded before the disclosure of treatment assignment because of inclusion criteria violations. Their HbA1c levels exceeded the limit set in the inclusion criteria. Finally, the data from 38 subjects (n=19 in the MLAE group and n=19 in the placebo group) (Fig. 1) were included in the statistical analysis. There were no significant differences in the baseline characteristics, including glycemic control parameters, anthropometric measurements, and serum lipid profiles, between the MLAE and placebo groups (Table 2). The average energy intake during the 3 days before the initial visit (at week 0) and at the last visit (at week 4), as calculated from self-reports, was not significantly different between the groups. Furthermore, intakes of each type of nutrient (carbohydrate, protein, fat, cholesterol, and fiber), alcohol consumption, and time spent exercising were not different between the groups (data not shown).
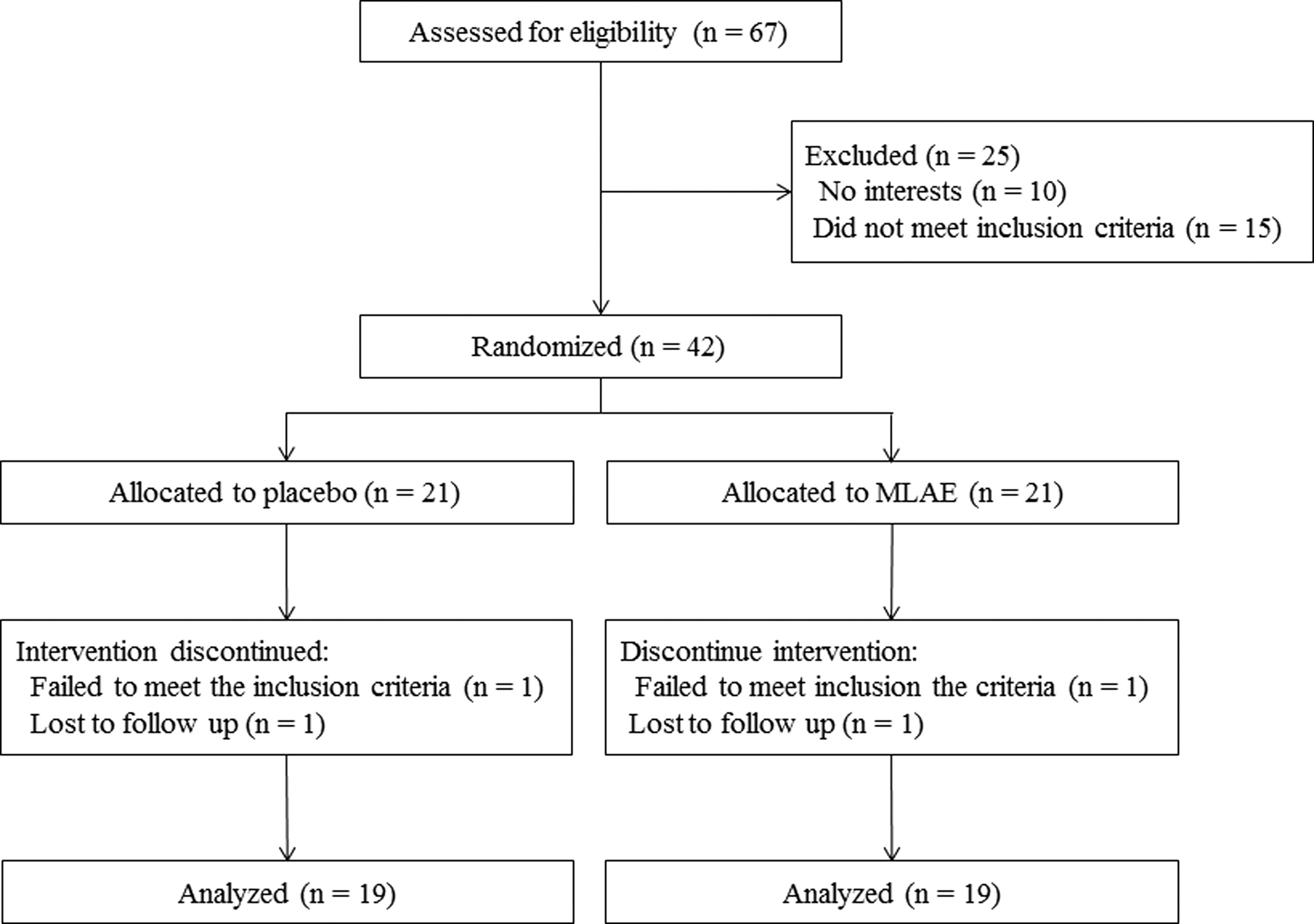
Flow chart of the main trial.
Mean±SD.
P-values derived from Student's t-test or chi-square test.
Tested after logarithmic transformation.
HbA1c, hemoglobin A1c; MLAE, mulberry leaf aqueous extract; SD, standard deviation.
The postprandial glucose, insulin, and C-peptide responses are presented in Figure 2. At the first visit, the postprandial meal tolerance was tested after a carbohydrate load with white bread and strawberry jam (80 g carbohydrate). Although there were significant variations in the postprandial blood glucose, insulin, and C-peptide levels over time (P<.0001 by repeated ANOVA), no significant interactions existed between the MLAE and placebo groups (P=.3219, .8358, and .9385, respectively). Conversely, after 4 weeks of MLAE or placebo use, the postprandial glucose, insulin, and C-peptide responses after the patient had been loaded using white bread, strawberry jam, and MLAE were significantly decreased (Fig. 2). There were significant variations in postprandial blood glucose, insulin, and C-peptide over time (P<.0001 by repeated ANOVA), which was significantly lower after the MLAE intake at 30 min and 60 min (P=.0003 and .0325, respectively, for glucose; P=.0005 and .0350, respectively, for insulin; and P=.0096 and .0156, respectively, for C-peptide after adjusting for the baseline values). The test group×time interaction for glucose and C-peptide responses was also significant (P=.0051 and .0449, respectively). The AUCs for postprandial glucose, insulin, and C-peptide are presented in Table 3. Before the MLAE supplementation, the AUCs for postprandial glucose, insulin, and C-peptide were unchanged following the MLAE intake. However, after a 4-week MLAE supplementation, the AUC for postprandial insulin was significantly reduced according to the MLAE intake (P=.0207). The AUC for postprandial C-peptide also showed a decreasing tendency (P=.0590). When the fasting and postprandial glucose/insulin ratios were analyzed, the postprandial glucose/insulin ratios at 30 min were significantly higher in the MLAE supplementation group (P=.0141) (Table 4). This difference remained significant even after adjusting for the baseline levels (P=.0039). The anthropometric and blood measurements, such as total cholesterol, low-density lipoprotein (LDL) cholesterol, triacylglycerol, glycated albumin, and ox-LDL, did not change during the study period in either group (data not shown). The differences in the safety measures, including hematological and biochemical parameters, between the two groups were not significant (Table 5), and no serious adverse events were observed during the study period (including the withdrawn and excluded subjects).

The plasma glucose
Mean±SD.
P-values derived from Student's t-test.
Tested after logarithmic transformation.
Mean±SD.
P-values derived from Student's t-test.
P-values derived from after adjusting for each baseline value.
Tested by logarithmic transformation.
Mean±SD.
P-values derived from Student's t-test.
P-values derived from after adjusting for each baseline value.
Tested by logarithmic transformation.
AST, aspartate aminotransferase; ALT, alanine aminotransferase.
Discussion
In the present study, on the basis of the positive result of the acute maltose tolerance test, we analyzed the efficacy of consecutive administrations of MLAE standardized to 3.6 mg/g of DNJ for improving postprandial glucose and insulin control in subjects with impaired glucose tolerance. Among the enrolled subjects (n=42), 4 dropped out for personal reasons or inclusion criteria violation and 38 subjects completed the study. According to a power calculation, 16 subjects per group were needed to detect significant differences. Assuming a 20% dropout rate, as we recruited 42 subjects in the present study, compliance was high (90.5%) enough to detect the differences in the outcome measures. Over the 4-week supplementation period, after a meal load, the postprandial responses for glucose, insulin, and C-peptide and the AUC for the postprandial insulin and C-peptide levels were significantly decreased in the supplementation group; however, this result was not observed during the first visit (0 week). Several clinical studies have reported controlling postprandial glucose levels by using DNJ or mulberry extract containing DNJ. 23 –25,29 The coingestion of mulberry extract with 75 g of sucrose significantly reduced the blood glucose increase, although the DNJ content of that extract was not accurately determined. 24 Mulberry leaf powder containing 1.5% DNJ significantly reduced postprandial glucose when sucrose or a complex carbohydrate (boiled white rice) was loaded. 23,29 Mulberry leaf ethanol extract containing 0.77% DNJ suppressed the postprandial blood glucose and insulin when ingested with sucrose in the form of confections, such as mizu-yokan, daifuku-mochi, and cake. 25 Among these reports, Asai et al. have reported the effects of long-term supplementation with mulberry leaf extract in subjects with impaired glucose metabolism. 23 They observed that the serum 1,5-anhydroglucitol concentration, a sensitive indicator of postprandial glycemic control, was significantly increased in the extract group compared with the placebo group over a 12-week treatment period. In this study, we investigated the amelioration of direct postprandial glucose and insulin control over a 4-week period of supplementation with MLAE containing 0.36% DNJ. Although the intake amount of DNJ differed and the study period was shorter in this study than in Asai's study, 23 we confirmed that postprandial blood glucose and insulin concentrations were significantly managed with only 4 weeks of MLAE supplementation.
The postprandial glycemic control was much more pronounced for the insulin response, for which there was a smaller peak (32% reduction at 60 min) after consuming MLAE, particularly after a 4-week supplementation period. Intakes of meals containing high levels of carbohydrates, such as sucrose, induce a higher response in postprandial glucose, simultaneously stimulating insulin secretion, thereby resulting in hyperinsulinemia. Repeated exposure to postprandial hyperglycemia and hyperinsulinemia may cause insulin resistance, β-cell dysfunction, and inflammation. 30,31 In the present study, although the serum insulin concentrations paralleled the plasma glucose concentrations, the postprandial glucose/insulin ratio was higher in the MLAE supplemented group than in the placebo group at 30 min, which was the peak time (Table 4). MLAE might inhibit glucose uptake in the small intestine and attenuate the postprandial glucose response, which stimulates a lower insulin response compared to the placebo. No signs of exaggerated insulin response were noted. This phenomenon was also confirmed in the postprandial C-peptide response.
In contrast, no significant differences in FBG, HbA1c, and glycated albumin concentrations were observed between the groups (data not shown). These results are consistent with another report. 23 The FBG, HbA1c, and glycated albumin levels reflect time-averaged glycemia in the past 2–3 months and last 2–3 weeks. A meta-analysis of α-glucosidase inhibitors drug trials in patients with type 2 diabetes showed that the FBG and HbA1c concentrations are lowered by acarbose and miglitol. 32 –34 Because the subjects in those trials had diabetes, their baseline HbA1c and FBG concentrations were higher than those of subjects in the present trial. Additionally, the majority of the trials were conducted for over a 12-week period. For the most part, the target population for food supplements is people with IFG tolerance similar to the participants in our study. Presently, we recruited relatively healthy IFG subjects having no medications for safety reasons and considering the target population. Thus, the absence of significant effects on the FBG and HbA1c concentrations in the present trial might be a result of, at least partially, the lower baseline concentrations of the subjects. Additionally, the supplementation duration might not have been sufficient to effectively decrease the longitudinal average of blood glucose.
α-Glucosidase inhibitors, such as acarbose and miglitol, have been associated with gastrointestinal side effects, such as bloating, gas, and diarrhea, likely because of fermented undigested carbohydrates in the bowel. 33 –36 These symptoms were not significantly observed with MLAE supplementation in this study or in previous studies. 23,25 In addition, it is well known that single-drug treatments may have greater negative side effects; therefore, a combinational strategy with two or more compounds could achieve additive or synergistic effects. A recent study indicated that the combination of dietary polyphenol with acarbose showed synergistic effects on α-glucosidases. 37 The present study indicates that MLAE consumption modulates glucose and insulin homeostasis in healthy and IFG subjects after the ingestion of a carbohydrate-rich meal. MLAE is a rich source of dietary fiber and antioxidants, as well as DNJ. 38,39 Our previous studies also confirmed that soluble dietary fiber as well as DNJ could be a functional ingredient in MLAE. 20 MLAE containing soluble dietary fiber and DNJ inhibited not only α-glucosidase activity but also glucose uptake in a small intestinal cell line, whereas DNJ alone did not. 20,40 Therefore, MLAE could be expected to be a combinational therapy, which might diminish the dose of α-glucosidase inhibitors, such as acarbose and miglitol, needed as well as functional food ingredients.
Control of blood glucose levels is a primary goal in the prevention or delay of diabetes onset. Especially, decreasing postprandial blood glucose excursions might be especially important in this regard. 41 One of the strategies for achieving adequate glycemic control could be using functional foods that lower postprandial glucose levels. The present result can be used as scientific evidence to support the use of MLAE as a functional food or dietary supplement to improve postprandial glycemic control in individuals who are at very high risk for progression to diabetes or who are unable to achieve adequate glycemic control by lifestyle modification alone.
Footnotes
Acknowledgments
The authors are grateful to the participants of this study. The authors also thank Dr. Kyung-Hee Chung and Dr. Ji-Hyang Wee for the preparation of MLAE. This work was supported, in part, by the Ministry of Knowledge & Economy (RITD Program, Project No. 2008-2769-2-3) and the Bio-Synergy Research Project of the Ministry of Science, ICT, and Future Planning through the National Research Foundation (NRF Project No. 2013M3A9C4078153).
Author Disclosure Statement
The authors declare that they have no competing interests.