
Abstract
This study investigated the effects of fucoidan (extract from Hizikia fusiforme) on symptoms and inflammatory cytokine activation in rats with monosodium iodoacetate (MIA)-induced osteoarthritis (OA). Forty male SD rats were divided into five groups, including normal, negative control (MIA), positive control (Lyprinol), and two experimental groups treated with 50 or 100 mg/kg fucoidan. Weight-bearing assessments were done after MIA injection into the right knee to induce OA. After 14 days of treatment, microcomputed tomographic (micro-CT) images were made of rat knee joints, and then animals were sacrificed for joint histology and inflammatory cytokine level assessments. MIA injection successfully induced OA by causing 40% weight-bearing imbalance, severe bone loss and cartilage degeneration, and markedly increased cytokine levels. However, fucoidan groups showed over 45% of imbalance and no articular cartilage surface lesions or change in subchondral trabecular bones in Micro-CT images. Histological analysis revealed that cartilage morphology and cell counts were also normal in the 100 mg/kg fucoidan group. In addition, the 100 mg/kg fucoidan groups exhibited lower serum tumor necrosis factor alpha (TNF-α) (30%), interleukin 1 beta (IL-1β) (48%), and matrix metalloproteinase-1 (MMP-1) (65%) compared to the MIA groups. These results suggest that administration of fucoidan prevents the progression of OA in a MIA-induced OA rat model.
Introduction
O
Little has been done clinically for OA, even though it is very difficult to restore cartilage once it is destroyed. The goals of treatment are to relieve pain, maintain or improve joint mobility, increase muscle strength, and protect cartilage and subchondral bone tissue from further degeneration. According to OA clinical guidelines, pharmacological management focuses on oral analgesics for relief of joint pain and stiffness, and improvement of joint function. However, guidelines do not include protection of cartilage and subchondral bone tissue. 4 Furthermore, most recommended nonsteroidal anti-inflammatory drugs have many adverse side effects, including gastrointestinal distress. When used for long periods of time these medications also have a harmful effect on collagen metabolism, which can aggravate OA. 5 For this reason, many studies have focused on functional foods, which may promote cartilage health and safety, even after long-term use.
The cause of OA is unknown, but several studies have suggested that OA joint degeneration results from a combination of mechanical stresses and biochemical factors, such as reactive oxygen species and matrix metalloproteinases (MMPs). 2
Previous studies have shown that MMPs and their tissue inhibitors play important roles in cartilage matrix turnover. 6 Matrix metalloproteinase binds to tissue inhibitors of matrix metalloproteinase (TIMPs) on a 1:1 basis by forming high-affinity complexes. 7 However, in OA subjects, upregulated MMPs are elevated to a much greater extent than TIMPs, which is thought to contribute substantially to extracellular matrix degradation. 8,9 Proinflammatory cytokines, such as interleukin 1 beta (IL-1β), which are produced directly by cartilage itself through activated synoviocytes or through other mediators, such as prostaglandin E2 (PGE2) and nitric oxide (NO), induce the biosynthesis and secretion of MMPs. 10,11
Articular cartilage damage and subchondral trabecular bone loss, which are seen in the case of OA, are caused by decreased elasticity resulting from structural deformation of cartilage matrix. Several kinds of irritants can cause the damage and bone loss, such as mechanical force and increase in matrix MMPs, which act as precursors to inflammatory cytokines, including IL-1β and tumor necrosis factor alpha (TNF-α). Increased MMPs and inflammatory cytokines are the chief causes of cartilage matrix degeneration. 12 Inflammatory cytokines and cartilage matrix degeneration combine to cause the symptoms of OA, including joint pain.
Intraarticular injection of monosodium iodoacetate (MIA) induces disorganization of articular cartilage by inhibiting the activity of glyceraldehyde-3-phosphate dehydrogenase in chondrocytes, resulting in the disruption of glycolysis and eventual cell death. These chondrocytes have similar histopathology to human OA, and the MIA-induced OA animal model closely mimics both the pain and structural changes associated with human OA. 13,14 Also, when MIA is injected into a joint capsule, TNF-α expression in the joint tissue is increased, and IL-1β is sequentially increased, which is similar in human OA. By recapitulating this phenomenon experimentally, MIA can be used to induce OA reliably, providing a good model for testing the effects of certain medical interventions on OA. 15,16
Fucoidan is a high-molecular weight polysaccharide contained in several species of popular edible brown sea algae such as Undaria pinnatifida, S. japonica and Hizikia fusiforme, which are mainly composed of fucoses and sulfate bases. 17 However, details of their structures are not fully known because they are complex, heterogeneous, and devoid of regularity.
Recently, it was discovered that fucoidan modulates diverse biological processes, including immunomodulatory, 18 anti-inflammatory, 19,20 and anticoagulant 21 effects. The osteoarthritic process may best be viewed as a chronic wound in which constant stimulation of innate inflammatory pathways by tissue damage can lead to a chronic remodeling response by all joint tissues. 22 For example, endocrine disruptors such as persistent organic pollutants markedly influence the immune system, 23 which could increase the risk of arthritis. 24 Therefore, the anti-inflammatory effect of fucoidan could provide a clue to prevent the progression of OA. With regard to arthritis, several recent studies already suggest a role for fucoidan in addressing the symptoms of arthritis. 25,26 However, very few studies have examined the precise role of fucoidans in modulating inflammatory processes and providing protection against OA.
This study investigates the effects of fucoidan on arthritic joint pain, degeneration of cartilage and subchondral trabecular bone, and changes in inflammatory cytokine activation in a MIA-induced OA rat model.
Materials and Methods
Preparation of fucoidan
Fucoidan extract was obtained from H. fusiforme (Wan-do Su-hyup). Hijiki was extracted for 2 h in hot water with a dried material to solvent ratio of 1:20 (5% w/v). Extract was collected by filtration (Whatman grade 2 filter paper; Whatman), and the solvent was evaporated under reduced pressure and stored at −20°C. 0.1 M HCl as described. 27 The extract was collected by filtration and fucoidan was precipitated from the extract by adding an equal volume of 2% cetyl trimethyl ammonium bromide (CTAB). A pellet of fucoidan was collected by centrifugation (Combi-514R centrifuge; Hanil Science Industrial) at 3430 g (3500 rpm, radius of rotor 250 mm) for 15 min, and dissolved in 100 mL of 2 M NaCl in 0.1 M Glycin-HCl pH 3.0. The fucoidan solution was further dialyzed with 4 L of water. Fucoidan precipitated from the solution with 5 volume of cool (−20°C) ethanol, and a pellet was collected by centrifugation, and then dried in a vacuum dessicator under KOH.
Carbohydrate content analysis of fucoidan
Total sugars were quantified for each polysaccharide fraction using the phenol H2SO4 method, 28 then the total carbohydrate content was calculated with reference to the sugar standard (200 μg/mL fucose) at 490 nm.
Sulfate content was estimated quantitatively using the BaCl2 gelatin turbidimetric method. 29 Test and control samples were assayed in triplicate, and absorbance (turbidity) measurements were made at λ=550 nm. The concentration of sulfate present was determined by reference to a sulfate standard curve using K2SO4 (300 μg/mL).
Molecular size analysis using gel permeation chromatography
Fucoidan molecular size analysis was determined by preparative gel permeation chromatography (GPC) as previously described. The GPC system consisted of three Ultrahydrogel Column Linear connections (1000-500-250; Waters), 0.2 M KNO3 eluant used to irrigate the columns at 0.7 mL/min, and a refractive index detector (Waters 410 PDA detector; Waters). Fucoidan structure was similar to the structure of dextran sulfate (5, 9–20, 500 kDa) purchased from Sigma-Aldrich.
Animal model preparation
Male SD rats (Daehan Biolink) weighing 270–280 g at the start of the experiment were used. Animals were housed two per cage in a room with controlled temperature conditions (21–22°C) and a reversed light–dark cycle (12 h:12 h). Animals had free access to sterile food and water. All experimental procedures were examined and approved by the Institutional Animal Care and Use Committee (IACUC) of the Kyung Hee University (IACUC No.: KHUASP(SU)-10-17). Rats were divided into OA-induced groups [OA group; n=8; (-) Control, Lyprinol, Fuco 50, and Fuco 100], and one control group which received no intervention (normal group n=8). To induce OA, 3 mg of MIA (Sigma-Aldrich) was dissolved in 0.05 mL sterile saline and injected into the right knee joint using a 27-gauge insulin syringe. After MIA injection, each group was treated with Lyprinol (100 mg/kg) or fucoidan (50 and 100 mg/kg) resolved to 0.5% CMC water was administered orally one time a day for 2 weeks.
Weight-bearing assessment
Hind limb weight-bearing was measured using an incapacitance tester (Linton Instrumentation), which included a dual-channel weight averager. Rats were carefully placed in a plastic chamber and positioned. The force exerted by each hind limb was averaged over 3 second periods. Each data point was the mean of three readings. The percentage of weight distribution onto the treated (ipsilateral) hind limb was calculated using the following equation: percentage of weight distribution=(weight on right leg/weight on left leg)×100. 13 A 50/50 weight distribution was considered normal for untreated animals.
Micro-CT analysis
Architectural changes in the subchondral trabecular bone of rat femur were analyzed with microcomputed tomography (Micro-CT) (Skyscan model 1076; Skyscan). Exposures were carried out at 60 kVp and 400 μA for 400 sec. Micro-CT data were obtained and analyzed using CT Analyzer V 1.8.0.5, software (Skyscan) and a three-dimensional (3D) and two-dimensional (2D) program. Three images from each category were selected based on image clarity and angle under naked eye observation resulting in ∼250 3D and 400 2D images.
Joint histology
Animals were perfused through the ascending aorta with 10% neutral buffered formalin (pH 7.4). Knee joints, including the patella and joint capsule, were dissected and kept in the same fixative for an additional 48 h at 4°C. Fixed specimens were decalcified with 5% formic acid decalcifier for 6 days at 4°C. After decalcification, specimens were embedded in paraffin. Standardized 7 μm sections were obtained at the medial and lateral midcondylar level in the sagittal plane and were stained with Safranin O or Toluidine blue to visualize proteoglycan content. Sections were counterstained with Mayer's Hematoxylin and photographed using an Olympus photomicroscope (Japan). A modified MANKIN system 30 was also used to score cartilage change on a scale of 0–6: 0=normal, 1=irregular surface, including fissures into the radial layer, 2=pannus, 3=absence of superficial cartilage layers (≥6), 4=slight disorganization (an absent cellular row and some small superficial clusters), 5=fissures into the calcified cartilage layer, and 6=disorganization (chaotic structure, clusters and osteoclastic activity). Cellular abnormalities were scored on a scale of 0–3, where 0=normal, 1=hypercellularity, including small superficial clusters, 2=clusters, and 3=hypocellularity. Matrix staining was scored on a scale of 0–4, where 0=normal/slight reduction of staining, 1=staining reduced in the radial layer, 2=staining reduced in the interterritorial matrix, 3=staining present only in the pericellular matrix, and 4=staining absent.
Inflammatory cytokine measurement in OA rat model
After sacrifice, whole blood was collected and serum obtained by centrifugation. Serum was analyzed using the commercial kits: TNF-α, IL-1β, and the MMP-1 ELISA Kits (Rat TNF-alpha DuoSet, Rat IL-1 beta/IL-1F2 DuoSet, Human Total MMP-1 DuoSet) to quantify expression of IL-1β and TNF-α, and indicators of inflammatory cytokine expression, and MMP-1 expression, which is an indicator of fibroblast collagenase that is involved in the breakdown of OA extracellular matrix.
Statistical analysis
Results were determined using the PRISM Statistical Analysis System. Analysis of variance (ANOVA) was used to identify statistically significant differences between groups (P<.05). Tukey's multiple comparison test was used for post hoc testing (P<.05). Values were expressed as mean±standard deviation.
Results
Carbohydrate content, sulfur content, and molecular size of fucoidan
Analysis of the carbohydrate content of fucoidan extracted from H. fusiforme showed that the proportion of fucose, which is the main component of fucoidan, was 61.48%. This value corresponded to typical fucoidan carbohydrate content. 28 In addition to L(−) fucose, fucoidan contained L(−) rhamnose (1.23%), D(+) galactose (24.53%), D(+) mannose (4.97%), and xylose (7.31%) (Fig. 1 and Table 1).

Carbohydrate content of the fucoidan. Fucose was identified as the main component of fucoidan. Rhamnose, galactose, mannose, and xylose were quantified as minor components.
Chemical composition of the purified fucoidan was Fucose, Rhamnose, Galactose, Mannose, and Xylose. Fucose was identified as a main component.
Total sulfate was estimated to be 11.6% by the BaCl2 gelatin method (Table 1). Molecular size analysis using size exclusion HPLC suggested that the fucoidan extracted from Hijiki was ∼30–50 kDa in size (Fig. 2).
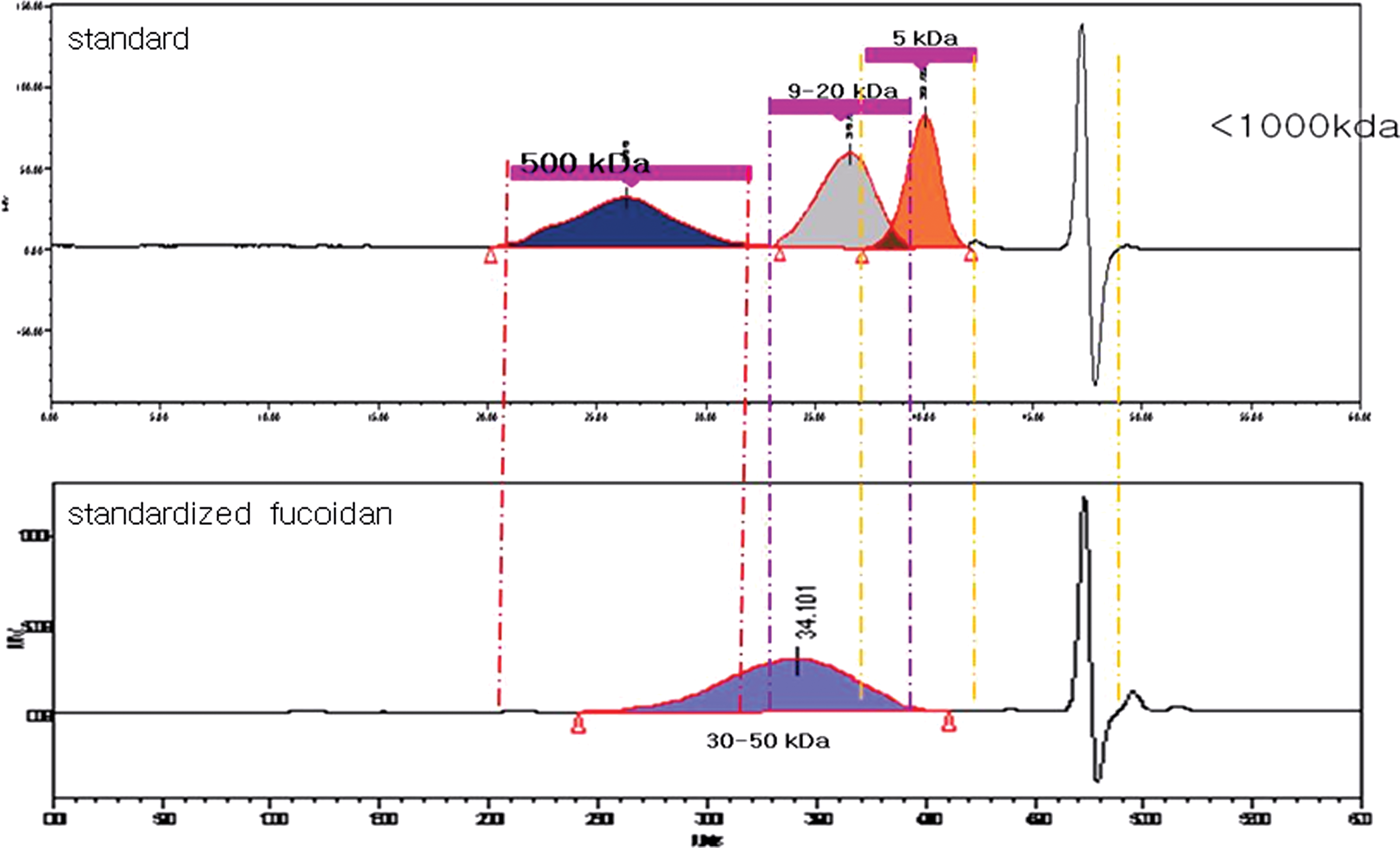
Molecular size analysis of fucoidan using size-exclusion HPLC. The molecular size of fucoidan was ∼30–50 kDa. Color images available online at
Weight-bearing exercise test
Since it is hard to bear weight on a MIA OA-induced knee, rats could not balance equally on both hind legs. The incapacitance test was able to quantify this side-to-side weight-bearing imbalance, which was used to quantify OA symptom level. 13
Results of the weight-bearing incapacitance test are shown in Figure 3. Graphs showed the differences between normal, negative control, and 50 or 100 mg/kg fucoidan groups. The value from the OA-induced side divided by the total weight-bearing value from both sides was calculated.
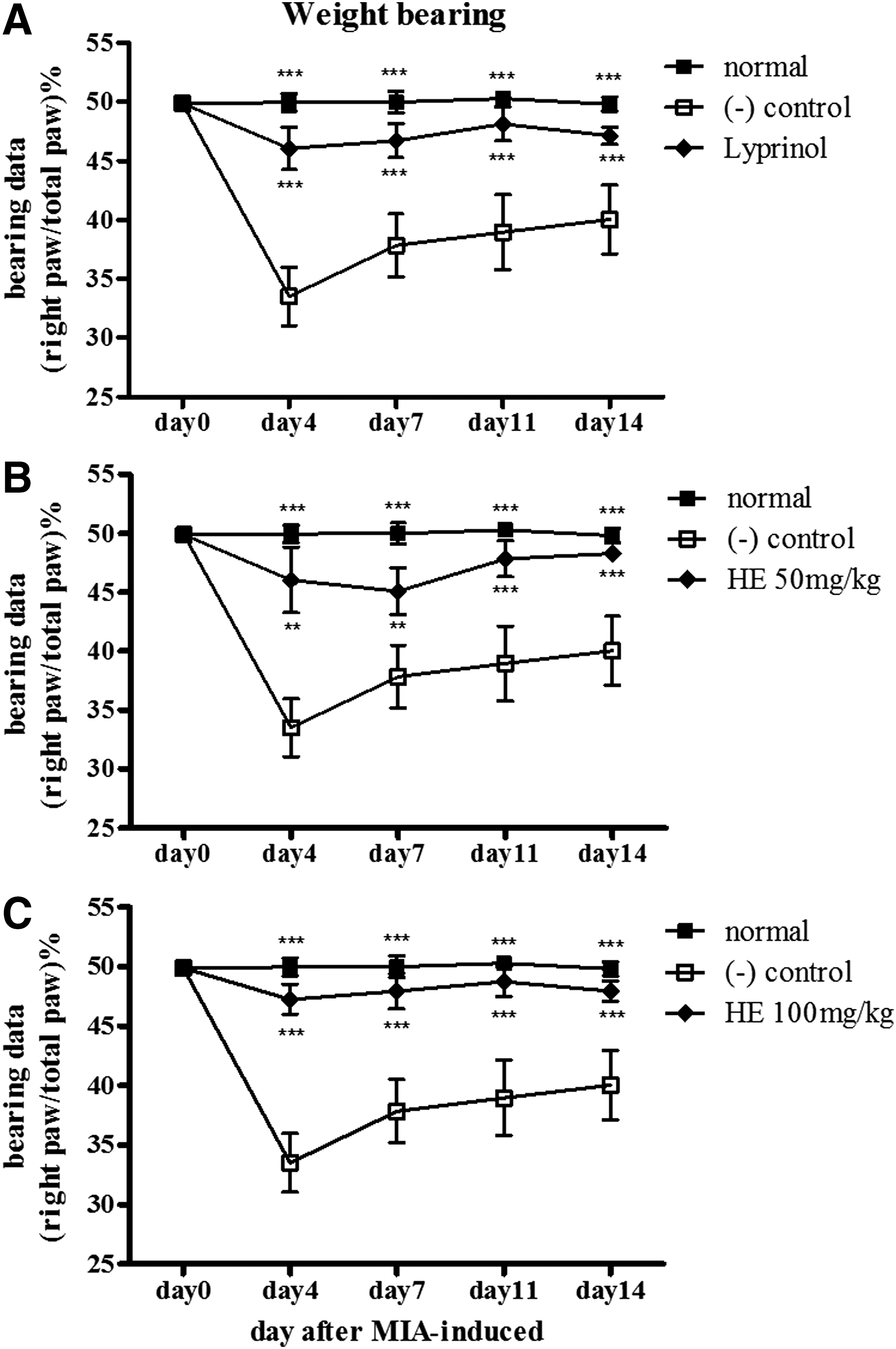
Effect of fucoidan in the weight-bearing test. The weight-bearing ratio was measured by an incapacitance tester and compared between the monosodium iodoacetate (MIA)-treated groups at 4, 7, 11, and 14 days after MIA injection.
In the MIA-induced OA group with no intervention (negative control group), after day 4, the ratio of the weight-bearing imbalance of the OA-induced group was 32%, which suggested a strong imbalance in weight bearing. Subsequently, the ratio recovered to ∼38% at day 14, perhaps due to recovery from inflammation.
By contrast, in the Lyprinol- and fucoidan-treated groups (50 and 100 mg/kg), there were slight weight-bearing imbalances of ∼45–48% on day 4 on the OA-induced side. After that, there was full recovery and the balance between both hind legs returned to normal in the 100 mg/kg fucoidan group (Fig. 3).
Micro-CT assay for articular cartilage and subchondral trabeculae bone degeneration
Mirco-CT scans were carried out to observe morphological features of articular cartilage and subchondral trabeculae bone in rat knee joints with MIA-induced OA 31,32 (Fig. 4).
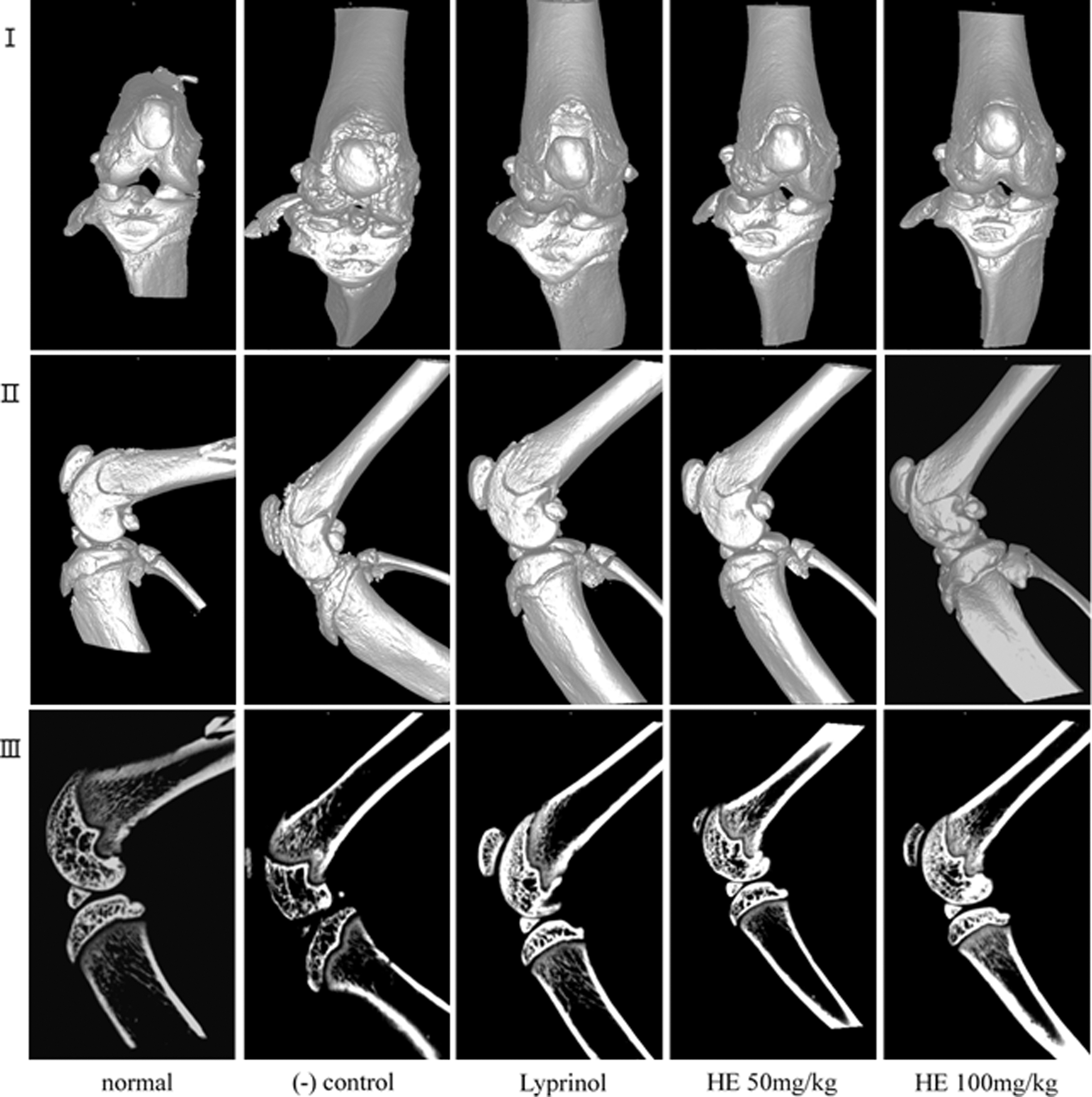
Micro-CT images of osteoarthritis (OA) joints after treatment with fucoidan in MIA-induced arthritis. Tissue from OA rat knee joints rats treated with fucoidan or vehicle were analyzed: 3D front image of knee joint (I), three-dimensional side image of knee joint (II), and two-dimensional image of knee joint (III).
Micro-CT scans showed severe subchondral trabecular bone loss and cartilage degeneration in the negative control group. In addition, patellar bones were deformed and meniscus cartilages were shifted slightly from the normal site.
In the 100 mg/kg fucoidan group, there was almost no articular cartilage surface lesioning. In the 50 mg/kg fucoidan group, the observed articular cartilage lesions were larger than that of the 100 mg/kg group, but smaller than that of the negative control. In the Lyprinol group, there was also almost no articular cartilage surface lesioning.
Histological analysis
Tissue from rat knee joints was stained with Hematoxylin and eosin, Toluidine blue, and Safranin O (Fig. 5). Histopathological analysis of each stained slide was conducted. Numerical grading of cartilage degeneration, cell abnormalities, and degree of matrix staining was carried out using the following scales: 0–13, 0–6, 0–3, and 0–4, respectively in each experimental group (Fig. 6). No significant lesions or abnormal staining were observed in any samples from the normal group 30,33 (Fig. 5).
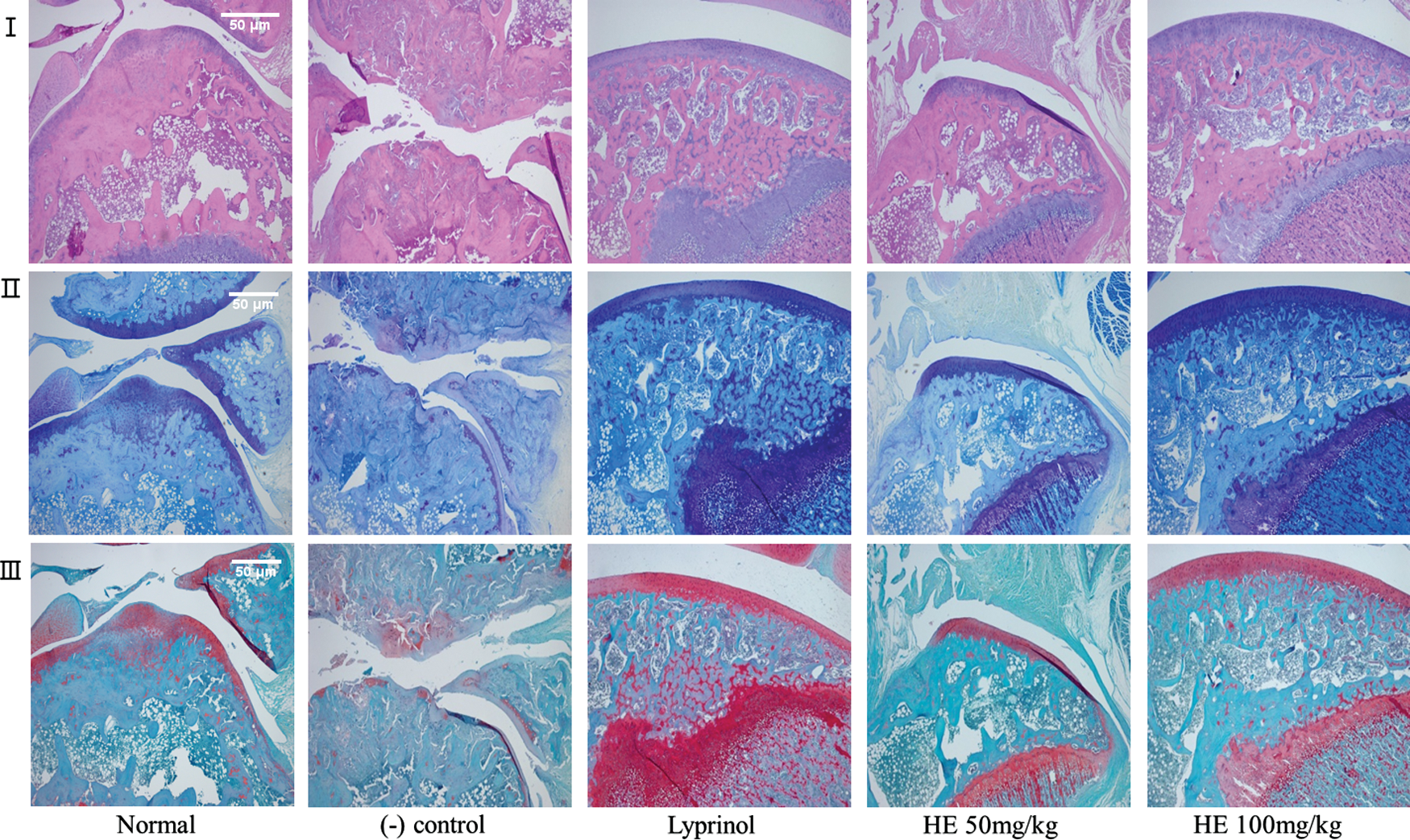
Histological analysis of the OA joints after treatment with Fucoidan in MIA-induced arthritis. Tissue from OA rat knee joints rats treated with fucoidan or (-) control were stained with Hematoxylin and eosin (I), Toluidine blue (II), and Safranin O fast green (III). Quality of staining on the femur end cartilage surface corresponded to better joint cartilage condition. Original magnification×40 and scale bar was 50 μm. Color images available online at
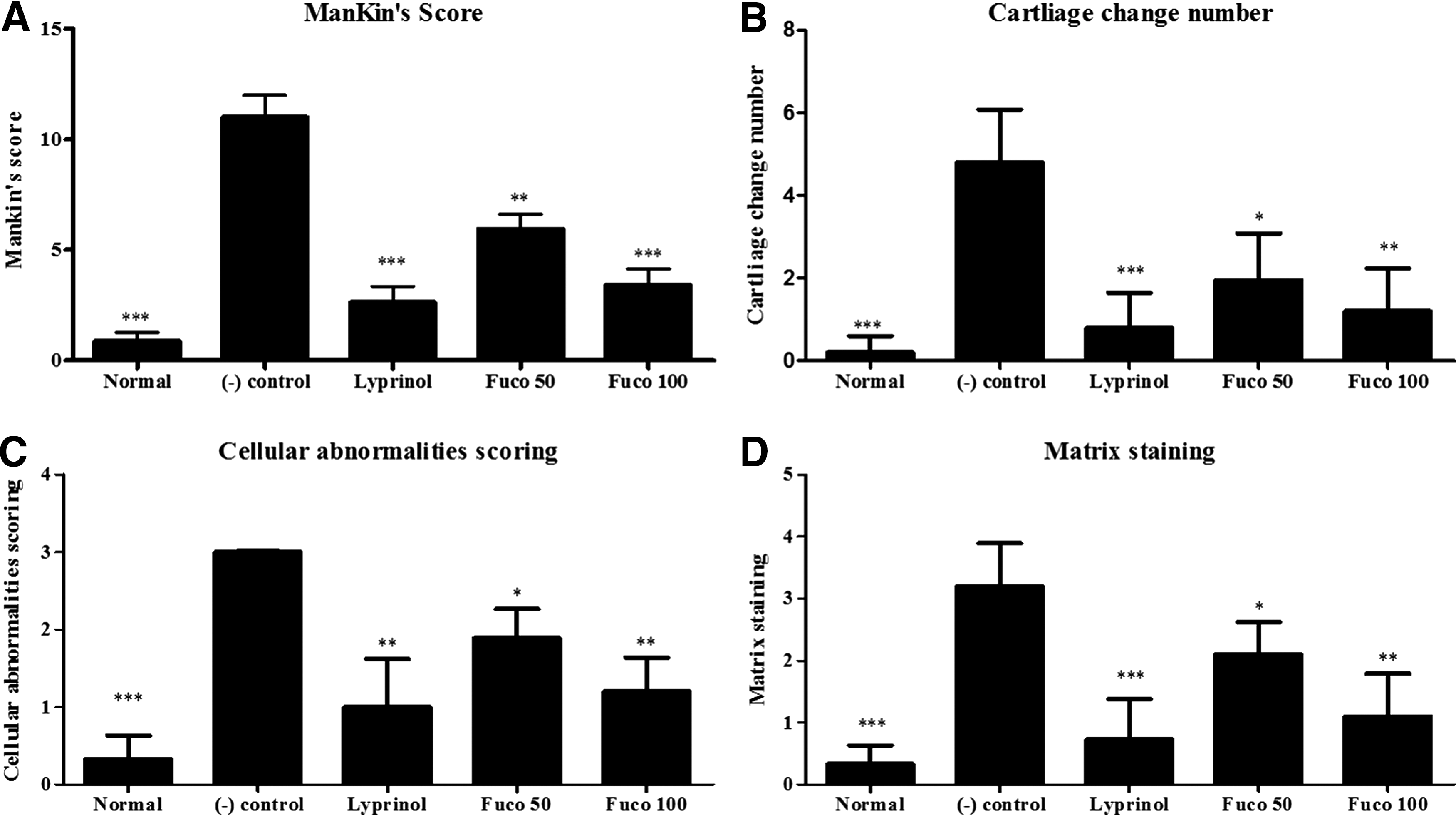
Histological analysis of OA joints after treatment with fucoidan in MIA-induced arthritis. OA lesions were graded on a scale of 0–13 using the modified MANKIN system
In the negative control group, disappearance of cartilage surface with disorganization was observed, followed by a decreased stained cell count. Staining was only observed in the matrix around cells.
On the other hand, in the 100 mg/kg dose fucoidan group, disorganization of cartilage was rarely observed, and there was almost no staining figure loss. This suggested that the cartilage morphology was maintained, although there was a rare decrease in stained cell count. In the 50 mg/kg fucoidan group, disorganization of articular cartilage was observed. Stained cell count was decreased in some cases and the staining figure was also decreased. In the Lyprinol-treated group, disorganization of cartilage was rarely observed and there was almost no staining figure loss.
Serum cytokine analysis
Serum TNF-α level was measured in each rat using ELISA. TNF-α level was almost twice (203.10%±6.82%) as high in MIA-induced OA compared to the normal group. Although the rats in the group treated with fucoidan also received a MIA injection, serum TNF-α levels of the fucoidan 50 mg/kg dose group and of the 100 mg/kg dose group were 21.5% and 31.0% less than the negative control groups. Lyprinol-treated groups were 36% less than the negative control groups (Fig. 7A).

Effects of fucoidan on the expression of tumor necrosis factor alpha (TNF-α)
Serum IL-1β level was also assessed with ELISA. IL-1β level in the negative control group was 2.2 times higher (218.10%±1.32%) than the normal group. However, serum IL-1β level in the fucoidan 50 mg/kg and 100 mg/kg groups were 36.2% and 47.8% less than that of the negative control groups. Lyprinol-treated groups were 36% less than the negative control groups (Fig. 7B).
MMP-1 expression level analysis showed that MMP-1 expressions in negative controls were 3.5 times higher (347.99%±24.56%) than that of the normal group. However, serum MMP-1 expression levels in the fucoidan 50 and 100 mg/kg groups were 57.6% and 65.5% less than the negative control groups. Lyprinol-treated groups were 36% less than the negative control groups (Fig. 7C).
Discussion
Fucoidans show many biological benefits for cardiovascular health, gastrointestinal health, 34 immunomodulation, 18 anti-inflammatory processes, 19,20 and anticoagulation. 21 Fucoidan is a commonly known high-molecular weight polysaccharide (200–500 kDa). In our study, we utilized the low-molecular weight (30–50 kDa) fucoidan from Hizikia (Fig. 2). This low-molecular weight fucoidan has the advantage of increased absorption compared to the high-molecular weight fucoidan. 35 In addition, the effect of oral administration of high- and low-molecular weight fucoidan on the progression of collagen-induced arthritis has been tested. A daily oral administration of high-molecular weight fucoidan exacerbates arthritis by the proinflammatory activation of macrophages, whereas low-molecular weight fucoidan decreases arthritis through the suppression of Th1-mediated immune reactions. 25 For this reason, the low-weight fucoidan utilized in this study could be expected to produce significant beneficial effects on MIA-induced OA in SD rats.
OA is common among the elderly population, but its cause is unknown. Several studies associated with OA have suggested a combination of mechanical stress and biochemical factors (MMPs, IL-1, and TNF-α). 2,6
Recently, injection of MIA into rat knee was developed to induce OA-like symptoms. 13,14 The rat MIA model has advantages over spontaneous or surgical models in larger animals. Smaller amounts of inhibitor and shorter time periods are beneficial. 1 This study investigated the effect of fucoidan on changes in behavioral (or physical) and biochemical factors associated with MIA-induced OA in SD rats.
These results showed that fucoidan significantly protected weight bearing in MIA-induced OA rats (Fig. 3 and Table 1) suggesting fucoidan could be useful for treating OA pain.
Micro-CT scans were carried out to observe morphological features of articular cartilage and subchondral trabecular bone in MIA-induced OA rat knee joint (Fig. 4). Fucoidan groups showed very small or no lesions on the articular cartilage surface, even though positive control groups still showed greater morphological changes, including rough cartilage edges, bone lysis, and a tendency to patellar displacement. Rat knee joint tissue was stained with Hematoxylin and eosin, Toluidine blue, and Safranin O, then histopathological analysis of each stained sample was conducted. In the MIA-injected groups, joint cartilage showed an irregular surface accompanied by fibrillation. Fucoidan-treated groups showed rare disorganization of cartilage, and there was almost no staining figure loss. This suggested that cartilage morphology was protected, and there was decreased inflammatory cell count in some cases. These results suggest that fucoidan was more beneficial than the positive controls. This suggests that fucoidan suppressed bone loss and prevented articular cartilage inflammation, resulting in the prevention of OA progression.
Also, when MIA was injected into the joint capsule, TNF-α expression in joint tissue increased, and IL-1β sequentially increased, which experimentally recapitulated normally developed OA. Therefore, MIA can be used to induce OA experimentally, providing a good model for testing the effects of OA medical interventions. 15,16 We observed OA-related biochemical factors, such as TNF-α, IL-1β, and MMP-1. Our results showed that serum TNF-α and IL-1β levels were almost twice as high in MIA-induced OA groups, compared with normal controls (Fig. 7). However, fucoidan decreased TNF-α expression by 30% compared to the negative control group (Fig. 7A). Moreover, fucoidan decreased serum IL-1β levels by 48% compared to the negative control group (Fig. 7B). These results suggest that fucoidan protected articular cartilage by regulating levels of TNF-α and IL-1β. In addition, MMP-1 expression level analysis showed that fucoidan decreased the MMP-1 expression by 65.5% compared with negative control (Fig. 7C). Therefore, fucoidan suppressed the expression of MMP-1 at the articular surface and inhibited collagen disorganization. Overall, the administration of fucoidan prevents the progression of OA in a MIA-induced OA rat model.
Joint health has been an important dietary supplement category for decades. The main ingredient used in most products is glucosamine sulfate, with a few other minor competitors. There has been a modest decline in joint care supplementation due to a lack of new supplement candidates. In the United States and Asia, fucoidan has been categorized as a food and is considered safe for the vast majority of people to ingest. Even in high doses (2000 mg/kg), there are few side effects (i.e., a small delay in blood clotting time at 1500 mg/kg). 36 Therefore, a fucoidan dietary supplement may be of interest to consumers either as a stand-alone product or within a matrix of ingredients.
This study suggests fucoidan could become an effective botanical supplement for OA. It relieved joint pain and stiffness, improved joint function, and protected cartilage and subchondral bone tissue with few adverse side effects in an OA rat model. Thus, future clinical trials of fucoidan as an aid in OA prevention will be undertaken in human subjects. 37
Footnotes
Acknowledgment
This work was conducted under the industrial infrastructure program (No. N0000888) for fundamental technologies, which is funded by the Ministry of Trade, Industry, and Energy (MOTIE, Korea).
Author Disclosure Statement
No competing financial interests exist.