
Abstract
Lifestyle, especially diet, is a prominent risk factor that affects the formation of calcium oxalate stones. Urinary oxalate excretion is directly related to the amount of oral intake and intestinal absorption rate of oxalate. This work evaluated the possibility of increasing oxalate ingestion, which could lead to secondary hyperoxaluria, associated with the intake of herbal remedies and dietary supplements containing plant extracts. A wide variety of 17 commercially available drugs and dietary supplements were analyzed using ion chromatography. The results showed remarkable differences in oxalate contents of the extracts. Total oxalate concentrations ranged from 0.03 to 2.2 mg/g in solid samples and from 0.005 to 0.073 mg/mL in liquid samples. The selected herbal remedies and dietary supplements containing plant extracts represent only a low risk for calcium oxalate stone formers, if the recommended daily dose is not exceeded.
Introduction
C
Oxalate is generally found in nearly all plants, in variable concentrations, and all vegetable tissues accumulate oxalate. Although not precisely defined, some suggested roles of oxalate in vegetables are calcium regulation, protection against predators by dermal irritation, and control of toxic heavy metals. 9 –11 Therefore, the consumption of vegetables, included in every healthy diet, is a remarkable source of oxalate as many studies have pointed out by determining the oxalate content in a wide variety of products with vegetal origin, such as spinach, rhubarb, beetroot, 12 nuts, 13 cereals and cereal products, 14 tea, 15 or pasta. 16
Herbal remedies and dietary supplements are very common in Europe and widely applied today. Given the high interest on the characterization of food and plant components, various methodologies have been used for the determination of oxalate content in such samples, including enzymatic reactions coupled to chromatography 17 or linked to spectrophotometric techniques. 18 This work has considered a simple and also robust technique, ion chromatography, which yields low detection limits and can perform the quantification of organic ions in aqueous matrices with little sample preparation. 19 The goals of this work were to assess and quantify the oxalate content of herbal remedies and dietary supplements based on plant extracts because data on the oxalate content are not available. As some of the products may be used on a daily basis, the duration of treatment with herbal drugs and dietary supplements could represent a risk for calcium oxalate stone formers.
Materials and Methods
Sample description
A selection of 17 herbal remedies and dietary supplements containing plant extracts commercially available in Germany was performed to cover a wide range of plant families. They are generally used for the treatment of general physical discomfort related to cold and flu, diarrhea, vertigo, and emotional stress and for the recurrence prevention of stone disease, and so their use is remarkably widespread. Although all the samples are plant extracts, the collection included different intake formats, for example, capsules, liquids, and tablets, as described in Table 1.
The commercial names and manufacturers correspond to the German market, from which the samples were purchased.
Sample preparation
To determine the soluble and total oxalate contents, two different conditions were used for the sample preparation. The soluble oxalate fraction was obtained using Milli-Q water (18.3 MΩ filtered), whereas 2 M HCl (Merck, Darmstadt, Germany) was used for the quantification of the total oxalate content. The acid treatment was selected to imitate the conditions that samples would experience in the stomach. Two units of each sample, that is, capsule or tablet, were independently weighed (duplicate) and dissolved in 4 mL water or HCl and stirred for 15 min at room temperature using a magnetic stirrer. The resulting solutions were filtrated at gravity, and immediately afterward, the samples were placed in the analyzer. For those samples in a capsule format, only the inner content was used for the analyses since the composition of the capsule did not contain oxalate or any precursor, according to the manufacturer's information. Liquid samples were only diluted with Milli-Q water before analysis.
Ion chromatography analysis
The equipment used in the present work was a Dionex ICS2100 (ThermoFisher Scientific, Waltham, MA, USA), served by a Dionex AS-AP Autosampler. After a 1:50 to 1:200 dilution, adapted to each sample, in 0.3 M H3BO3 (Sigma-Aldrich, Steinheim, Germany), the sample was injected through a 25-μL loop into the separation system. This part of the equipment consisted of a precolumn Dionex IonPac AC11 (2 × 50 mm), followed by an anionic separation column Dionex IonPac AS11 (2 × 50 mm), operated at 35°C. The detector used was an ion suppressor, Dionex ASRS-300. The software Chromeleon (Dionex) allowed the experiment performance and data recording.
The conditions were adapted from the existing bibliography. 19,20 The mobile phase used was KOH (flow 1.5 mL/min) with a concentration gradient as follows: 0.2 mM during 6 min and, then, KOH concentration increased up to 5 mM at 0.8 mM/min (total run 12 min). After 12 min, the separation gradient was followed by a cleaning sequence (5 min running 100 mM KOH) and a stabilization time of 5 min.
A six-point calibration curve was measured, covering oxalate concentrations in the range 0–10 μM. The set of standards was prepared from a concentrated 2 mM sodium oxalate solution (Sigma-Aldrich). All samples, including both oxalate extraction methodologies, were analyzed in duplicate.
Quality assurance and quality control were performed by checks on the samples. A standard was checked each 10 processed samples, and a spiked sample was added every four analyses. Spikes were done on the samples before and after the dissolution with water and HCl. The spiked samples were prepared by adding 2 μM oxalate to the dilution. The recovery was then calculated by comparing the spiked sample to the plain sample. Spike recoveries were considered acceptable if the criteria listed in Table 2 were met. In all cases, the signal of the spiked samples was quantified within the dynamic range of the analytical method. The absence of oxalate contamination was checked by measuring a blank sample (containing only 0.3 M H3BO3) after the last calibration point and after each run. The values for the calibration curve are shown in Table 2. Limit of detection (LOD) and limit of quantitation were calculated as the concentration associated with the blank signal plus its standard deviation multiplied by 3 and 10, respectively. The methodology reproducibility, calculated as relative standard deviation, was measured by repeatedly running the same sample in the same and different batches.
LOD, limit of detection; LOQ, limit of quantitation; RSD, relative standard deviation.
Results
Methodology
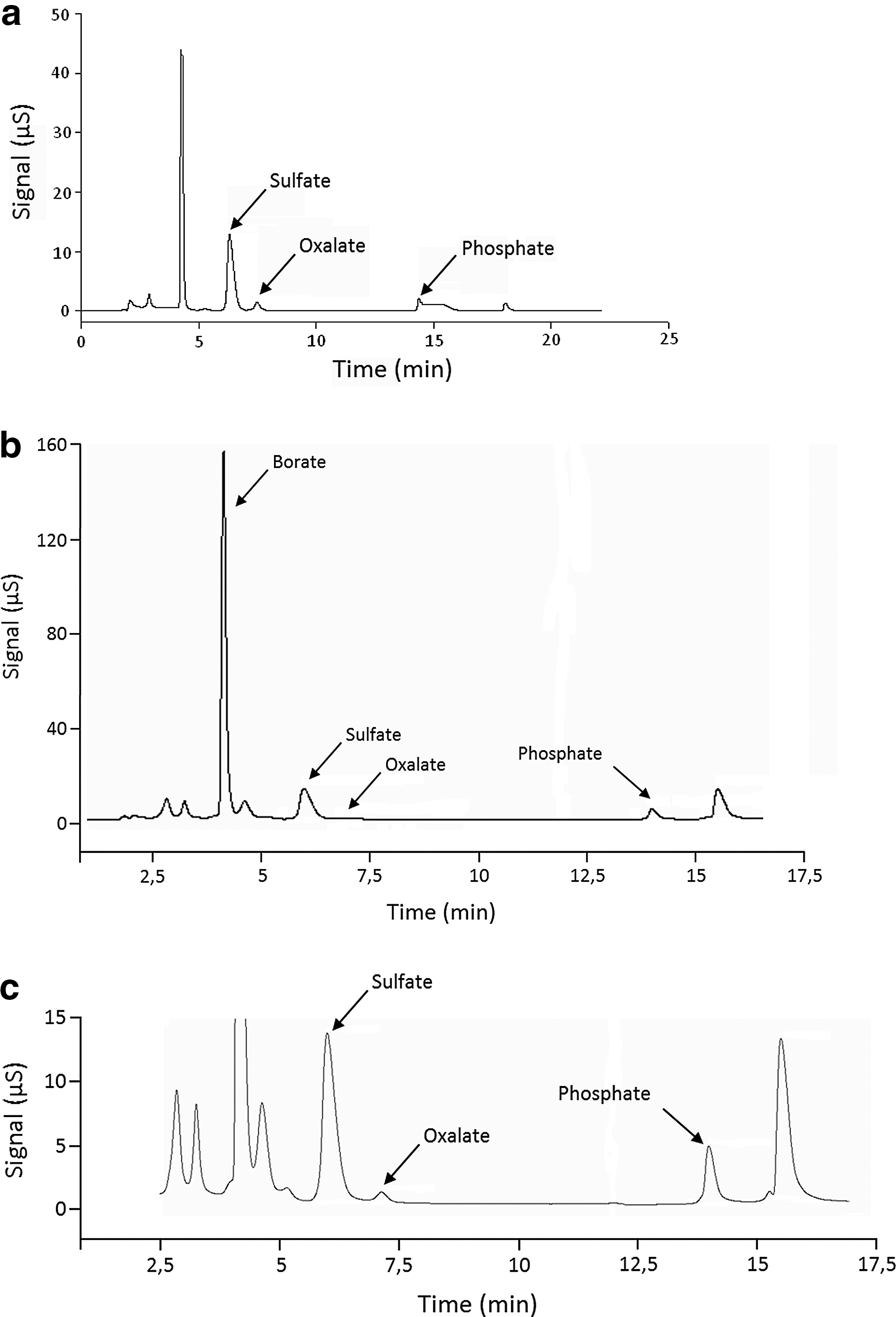
The methodology yielded good results in terms of component separation and, especially, oxalate quantification. A standard solution containing possible interferences, which might induce overlapping peaks, was also measured. Sulfate and phosphate ions, usually occurring in natural samples, were added to a standard solution as a test. Figure 1a shows a standard solution containing 10 μM oxalate, spiked with 20 μM sulfate and phosphate. As observed, the resolution of the oxalate peak was satisfactory, and the baseline nicely reached after the sulfate peak. A chromatogram of a sample is presented in Figure 1b and its magnification in Figure 1c. The natural sulfate content showed a high peak that did not interfere with the analysis of the oxalate content.
The validation of the methodology and control of the quality parameters of the analysis were performed as described in the previous section and satisfactorily met the required criteria. As seen in Table 2, the parameters concerning the suitability of the chromatographic method for the analysis of the plant extract samples laid within acceptable quality, reproducibility, and recovery limits.
Sample analysis
The oxalate concentrations of the analyzed solid samples are listed in Table 3. According to the different plant species the samples belong to, the oxalate content varied within a wide range, that is, between 0.03 and 2.2 mg/g extract. The two samples, which showed the highest total and high soluble oxalate contents, respectively, were green tea (1.9 and 1.8 mg/g) and the mixture containing vervain–gentian–sorrel–elder–cowslip (2.2 and 0.22 mg/g). All other analyzed solid samples contained small amounts of total oxalate, that is, below 0.6 mg/g extract.
N/A, not applicable; LOD, concentration below the limit of detection.
With regard to the extracts in liquid format, the oxalate content range was not as wide as for the solids (Table 4). Nevertheless, three groups could be defined. The concentration for ivy leaves and uzara extracts was around 0.005 mg/mL. The oxalate content of echinacea extract laid over 0.070 mg, and the rest ranged from 0.010 to 0.023 mg oxalate per mL.
Based on the concentration values, the daily oxalate intake, according to the manufacturer's recommended dose, was calculated (Table 5). In this sense, only three of the analyzed plant extracts (green tea and the mixtures birch–orthosiphon–goldenrod and vervain–gentian–sorrel–elder–cowslip) resulted in a total daily amount close to or greater than 3 mg oxalate. The oxalate content determined in the rest of the samples was rather low.
In liquid samples, the whole oxalate fraction was assumed to be in soluble form or as very small particles in suspension but not as crystals.
N/A, not applicable.
The calculation of the soluble to total oxalate ratio is listed in Table 5. The soluble to total oxalate ratios ranged generally from values higher than 65% in black cohosh to nearly 95% in green tea. A few exceptions were found, namely, iceland moss extract and the mixture containing vervain–gentian–sorrel–elder–cowslip, for which low soluble oxalate contents were determined.
Discussion
As expected, the dietary supplement containing green tea extract was among the samples with the highest oxalate concentration. According to the manufacturer's information, two capsules of the green tea extract Praevent loges® correspond to the intake of 10 cups of green tea. Assuming that a cup may hold 150 mL, two capsules are equivalent to 1.5 L of a high-quality green tea supplying 1.8 mg total and 1.7 mg soluble oxalate. Green tea is known to contain high amounts of oxalate. 15,21 A previous study revealed that the soluble oxalate content of green tea ranged from 8.3 to 139.8 mg/L or 12.45 to 209.7 mg/1.5 L, which is far above the oxalate content detected in the dietary supplement. 15 As the green tea preparation has been decaffeinated by the manufacturer, it is suggested that the low oxalate content may result from the extraction or decaffeination process.
Interestingly, the herbal remedy that showed the highest oxalate content was that containing the most complex mixture of plants, that is, vervain–gentian–sorrel–elder–cowslip. Indeed, the amount of oxalate in this case was even higher than that for the tea. The component in this mixture, which has been reported to have high oxalate content, is sorrel. 12 It is suggested that the high oxalate concentration of this herbal remedy can be attributed to the content of sorrel.
In contrast, some of the analyzed extracts showed small amounts of oxalate. In fact, the solid samples, for example, black cohosh, vitex, and ginkgo, had an oxalate concentration below 0.1 mg/g, and all liquid samples, for example, chamomile, thyme, and ivy leaves, had an oxalate concentration below 0.1 mg/mL. As these plants have not been analyzed so far, data on the oxalate content are not available. For the activated carbon, this value was even below the LOD, fact that fits to its nature, based on elemental carbon.
The total oxalate content is not the only important factor when its influence on the metabolism is assessed. With regard to the stone formation risk, the quantification of the soluble fraction is also necessary. It has been widely reported that oxalate behavior in the intestinal tract is highly dependent on its chemical form. 7,12,14 It is known, as well, that oxalate absorption is also linked to the calcium intake since it forms a stable complex, and this prevents oxalate from being assimilated. Although this behavior of calcium and oxalate is known, the estimation of the amount of oxalate lost in the stool as calcium oxalate is complex. Still, the calculation of the soluble to total oxalate ratio is a rather good approach to guess its bioavailability. 22,23 The difference in the soluble to total oxalate ratios could perhaps be explained by the different techniques used for extracting bioactive compounds from plants. However, information on the effect of different extraction methods on the total and soluble oxalate contents is lacking.
The oxalate concentration of the herbal remedies and dietary supplements containing plant extracts analyzed in this work showed a high variability. Considering the manufacturer's recommended daily dose of the herbal remedy or dietary supplement, the daily total oxalate intake did not exceed 4 mg. Taking into account an intestinal oxalate absorption in calcium oxalate stone formers exceeding 10% of the intake, the intake of the herbal remedy and dietary supplement with the highest oxalate content, that is, green tea and the mixtures of vervain–gentian–sorrel–elder–cowslip and birch–orthosiphon–goldenrod, would add only 0.4 mg or 0.004 mmol oxalate per day to urinary oxalate excretion.
In conclusion, the sensitivity of the technique used allowed the quantification of the low oxalate concentrations measured in the plant extract samples studied. The results obtained describe a representative selection of the commonly used herbal remedies and dietary supplements containing plant extracts. While the variety of products available in the market is broader, the general trend seen in the selected plant extracts is that they represent a low risk for calcium oxalate stone formation.
Footnotes
Acknowledgments
The project was funded by the Department of Urology, University Stone Centre, University of Bonn, Germany, and the Spanish Ministerio de Educación through the programs Becas FPU (Ref. AP2009-3245) and Estancias Breves (Ref. EST2012-0940) and supported through MINECO (Project Ref. CTM2012-30970).
Author Disclosure Statement
Roswitha Siener is a consultant to Bionorica SE. For all other authors, no competing financial interests exist.