
Abstract
Essential to human health, selenium (Se) has enzymatic functions of fundamental importance to human biology due to its effects on DNA damage repair, its antioxidant properties, and cancer prevention. The best studied relationships between Se and the immune system is its role in the functions of neutrophils and of lymphocytes. Despite these observations, it is not yet clear by which mechanism Se is able to modify the immune status. This was a double-blind, crossover study: Group 1 received Se and Group 2 received placebo (30 days). After this, Group 1 received placebo and Group 2 received Se (30 days). Every 30 days, blood samples were collected for white blood cell count, red blood cell count, and Ig level measurement (IgA, IgG, IgE, IgM). Of the 36 patients, 17 were suffering from leukemia/lymphomas (LL) and 19 from solid tumors (ST). In the ST group's leukogram, a significant increase in neutrophils was observed after Se usage (P = .0192). During the analyzed period, Se minimized the triggering of neutropenia cases in both groups. IgA and IgG levels in ST patients were significantly higher than those identified in LL patients after Se usage (P = .0051 and P = .0055). For IgA, a significant increase in its production, after Se usage, was observed in the ST group when compared to the LL (P = .0011). The same did not occur to the IgM and IgE immunoglobulins. In our study, the supplementation with Se reduced the neutropenic cases (LL and ST patients) and reduced IgG and IgA levels in LL and increased in ST group.
Introduction
E
According to some studies, Se has been recommended as an adjunct in the treatment of cancer in high doses (200 and 400 μg Se/day). 10,15,16 In addition to its antioxidant and antitumor function, Se also acts as a liver and kidney protector. 17 Such effect most likely stems from or is associated with a decrease in the levels of the enzymes aspartate aminotransferase—AST and alanine aminotransferase—ALT and creatinine and urea. The decrease of these biochemical markers (nephrotoxicity and hepatotoxicity) end up determining improved health quality of patients undergoing chemotherapy and radiotherapy treatment. 18 Studies in mice corroborate the findings obtained with human studies, in which it is clear that Se deficiency influences the levels and activity of liver enzymes directly linked to diseases resulting from oxidative stress and detoxification of carcinogens. 19
Found and stored in significant amounts in tissues such as the liver, spleen, and lymph nodes, plasmatic levels of selenium can influence the activation ability and quality of the cellular immune response (e.g., lymphocyte proliferation, response to mitogens, macrophage activation, synthesis of leukotriene B4, chemotaxis of neutrophils) and humoral immune response, decreasing the amounts of IgM, IgG, and IgA (murine models), and IgG and IgM (human studies). 4,17,20
One of the best studied relationships between Se levels and the immune system is the role of this micronutrient in the functions of neutrophils. In situations where a decrease in the action of Se-dependent antioxidant enzymes is observed, a concomitant reduction in the bactericidal capacity of neutrophils can be identified, most likely as a result of a decreased activity of GPx1, of the control of free radicals formation, and hindrance of the peroxide generating system. 20 Several studies in patients undergoing bone marrow transplantation or patients with chronic neutropenia 21,22 have shown that selenium supplementation can reverse or minimize the development of febrile neutropenia cases, which are highly compromising from the infectious point of view.
In a review carried out by Hoffmann and Berry, 23 it is possible to evaluate a series of studies about the relationship between selenium and the immune system. In general, the authors were able to point out that the use of selenium is able to increase the number of circulating lymphocytes, the lymphocyte functions, and provide greater protection against viral infections. Despite these observations, it is not yet clear by which mechanism selenium is able to modify the immune status of a particular host, mainly due to the various conflicting results from studies in human and animal models. 24 –29
Thus, the objectives of this study were to evaluate the effects of daily supplementation of selenium on the hematological cellularity and the immunoglobulin synthesis (IgA, IgE, IgM, and IgG) in infant patients with leukemias, lymphomas, and solid tumors (ST).
Patients and Methods
Patients
Patients with leukemias and lymphomas or ST were recruited from the Serviço de Oncologia Pediátrica da FMABC (ABC Medical School's Pediatric Oncology Outpatient Unit). They were of both sexes, aged up to 18 years. Patients who broke the protocol, who withdrew spontaneously, or who died were excluded. The study was approved by the Ethics Committee of the ABC Medical School (CAAE-05139812.9.0000.0082). All the patients' legal guardians (parents, grandparents, or tutors) were informed about the risks involved in the research and signed the term of informed consent.
Study design
This was a randomized, double-blind, placebo-controlled, crossover study. On accepting to participate in the study, patients were then randomized into two groups: Group 1 received daily supplementation of Se according to the age group presented and Group 2 received placebo capsules. In both cases, administration lasted 30 days (Fig. 1). Both groups underwent a washout period (without supplementation for 7 days). After this period, Group 1 received placebo and Group 2 Se for 30 more days. Each patient received 80% plus dietary recommendation intake (DRI). Every 30 days, blood samples were collected for white blood cell (WBC) count, red blood cell (RBC) count, and immunoglobulin level measurement (IgA, IgG, IgE, and IgM). When the research was concluded, the scores for each parameter were calculated, followed by the calculation of the statistical significance between the obtained scores: initial versus placebo, initial versus Se, and placebo versus Se.

Study design: randomization in selenium and placebo groups during 30 days; 7-day washout; group inversion (for 30 more days).
Supplementation
Group I received a daily supplementation of selenium glycinate (selenium molecule was chemically bound to glycine to ameliorate the intestinal absorption) and Group II received glycine starch capsules (placebo). The capsules used in both groups were identical in size and glycine dose amount, with no difference in the storage containers.
Dosage administration of selenium corresponded to the daily value intake recommended by the DRI for children within the studied age group. Such recommendations are elaborated by the National Research Council (NRC), Food and Nutrition Board in the United States. 30 For each DRI, an 80% overload was added and the following doses were established: 27, 36, 54, 72, and 100 μg of selenium (selenium glycine) as presented in Table 1.
Source: OMS.
Institute of Medicine/Food and Nutrition Board, US National Academy of Sciences. DRIs for selenium.
DRI, dietary recommendation intake.
Biological material analysis
From the collection of venous peripheral blood, the blood profile of each patient was drawn, with complete blood count and determination of serum levels of immunoglobulins (IgE, IgM, IgA, and IgG).
The WBC and erythrocyte count were performed in the automated hematology counter Abx Pentra 120 (Horiba). For this analysis, 5 mL of peripheral venous blood was used, collected with EDTA (ethylenediaminetetraacetic acid). The concentration of IgM, IgA, and IgG was determined by the single radial immunodiffusion technique and the concentration of IgE by the chemiluminescence method (Immulite 1000, Siemens). The normal values established for each age group assessed were used for the interpretation of the data.
All analyses were performed at the Clinical Analysis Laboratory of the Faculdade de Medicina do ABC (FMABC) following the best practices in clinical analyses.
Statistical analysis
The result analyses were performed by adopting a significance level of 5% (P ≤ .05) or, whenever possible, of 1% (P ≤ .01) in compliance with the following models: • Descriptive statistics. • Measures of central tendency. • Equality of means test (Student's t-test). • Equality of medians test (Mann–Whitney). • The software used was Prism version 3.0.
Results
A total of 74 patients were invited to participate. As a result of protocol breaks, spontaneous withdrawal, or the patient's death, only 36 individuals finished the study. Of the 36 patients who completed the protocol, 17 were suffering from leukemia/lymphomas (LL) and 19 from ST. Among the LL carriers, the average age was 7.6 years and in the ST group was 8.0 years. As for distribution according to gender, the LL group comprised 7 female and 10 male patients. In the ST group, there were 6 female and 13 male patients (Table 2).
GT, gastrointestinal tract tumor; LL, leukemia/lymphomas; ST, solid tumors.
Erythrogram and leukogram
Quantitative and qualitative analyzes of peripheral venous blood cells were performed (erythrogram, leukogram, and thrombogram), both in patients with LL and ST. Only in the ST group's leukogram, a significant increase in neutrophil count was observed when these patients were supplemented with selenium compared to the placebo usage period (P = .0192, Table 4). For all other evaluated parameters and groups studied (LL or ST), there was no significant difference during selenium supplementation compared to the intake of placebo (Tables 3 and 4).
When the average difference of the period in which the patients were supplemented (Se or placebo) was evaluated, compared to the start of the study (Se- beginning and placebo-beginning), it was observed that during the selenium usage period, there was a slight increase in the WBC count, neutrophils, circulating platelets, hematocrit, and hemoglobin in LL patients. When the same patients were given placebo, a slight decrease of the evaluated parameters was observed (Fig. 2). However, at no time the differences were significant. The same profile was detected in patients with ST, except for hematocrit percentage and hemoglobin levels. These last two parameters vary, very similarly, regardless of the supplementation used—Se or placebo (Fig. 3).
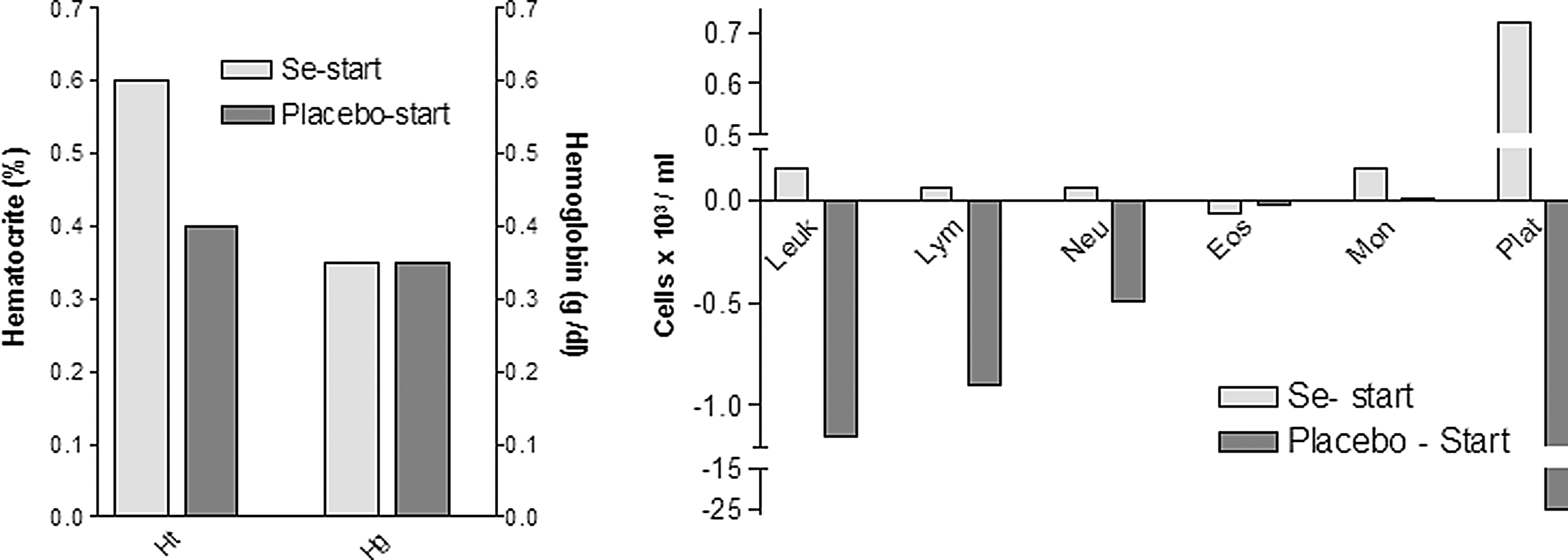
Mean differences during supplementation in patients with LL. Mean differences of hematological parameters in patients with leukemias and lymphomas. The values presented reflect the differences between what was observed after 30 days of supplementation (selenium or placebo) compared to the beginning of the study (D30 minus D0). LL, leukemia/lymphomas.
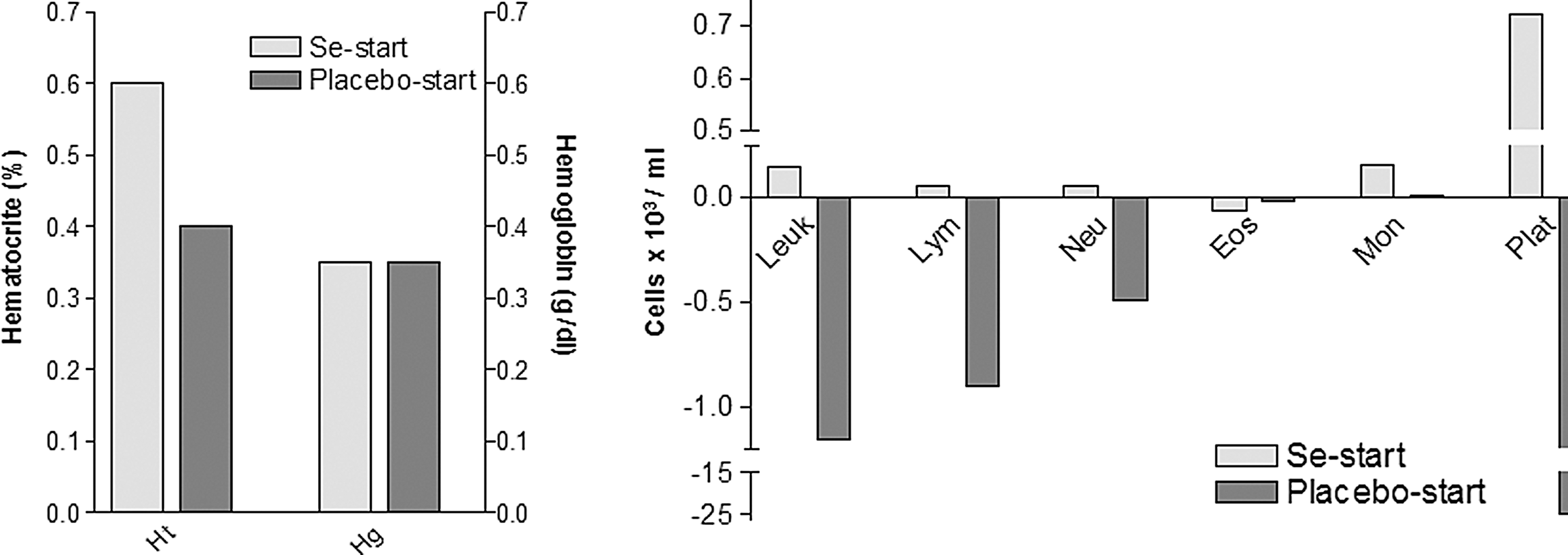
Mean differences during supplementation in patients with ST. Mean differences of hematological parameters in patients with solid tumors. The data presented reflect the differences between what was observed after 30 days of supplementation (selenium or placebo) compared to the beginning of the study (D30 minus D0). ST, solid tumors.
Considering the number of patients within the range considered normal for the age group in question, although treatment with selenium did not present any significant difference compared to placebo or to the beginning of treatment in the LL Group, it was observed that selenium supplementation provided an increased percentage of patients within the normal range compared to placebo, as follows: hematocrit (44%-Se ×27%-placebo), hemoglobin (48%-Se ×33%-placebo), leukocytes (23%-Se ×20%-placebo), lymphocytes (52%-Se ×46%-placebo), eosinophils (47%-Se ×33%-placebo), monocytes (52%-Se ×26%-placebo), and platelets (94%-Se ×80%-placebo). The number of patients with circulating neutrophils and erythrocytes within the normal range did not differ with either supplementation.
The ST group also showed an increase in the number of patients within the normal range after supplementation with Se for the following evaluated parameters: hemoglobin (23%-Se ×17%-placebo), neutrophils (59%-Se ×35%-placebo), monocytes (52%-Se ×29%-placebo), and platelets (65%-Se ×53%-placebo). The analysis of the number of patients who were within normal values for the parameters, hematocrit, erythrocytes, leukocytes, and lymphocytes, did not differ after either supplementation.
During the analyzed period, Se supplementation was able to minimize the triggering of febrile neutropenia cases (characterized by counts equal to or <500 neutrophils/mL) in both groups. Without any supplementation (beginning of study), 02 ST patients with neutropenia were observed, after supplementation with Se, no patient experienced neutropenia, and with the use of placebo, five patients presented the condition. In patients with LL, neutropenia was observed in 01 patient at the beginning, 01 patient during Se supplementation, and 03 patients during supplementation with placebo. Interestingly, the patient in the LL group who presented neutropenia at the beginning was the same who remained neutropenic after supplementation with Se. Despite this, there was a significant increase in the number of circulating neutrophils during supplementation: from 20 neutrophils/mL (beginning of the study) to 320 neutrophils/mL (supplementation with Se).
The levels of immunoglobulins (IgA, IgE, IgM, and IgG) from 36 patients were assessed at the beginning of the study (D0), after placebo usage and after supplementation with Se. At the beginning of the study, the 17 patients with LL showed the following immunoglobulin levels: IgM (33% within the normal range and 67% below normal); IgA (26% below normal and 74% within normal); IgG (100% above or within normal); and IgE (6% below normal and 94% normal). Patients with ST (n = 19) evaluated at the beginning of the protocol presented the following immunoglobulin levels: IgM (66% below normal and 34% normal), IgG (100% above or within the normal range), IgA (100% normal or above normal), and IgE (100% were above or within the normal range).
Regardless of the supplementation used (Se or placebo), no significant changes in the production of IgA, IgE, IgM, or IgG were detected, either in ST or LL patients, when the values obtained were compared to the ones detected at the beginning of the protocol. Of all the immunoglobulins produced by patients, irrespective of the disease in question (LL or ST), IgM was the only immunoglobulin that presented a decrease in its production to levels considered inferior to the established normal range. All the other immunoglobulins were produced within or above the values considered normal to the studied group.
Although no significant differences in the production of immunoglobulins after using selenium were observed, it was possible to identify that some patients had their levels of serum antibody altered when subjected to this supplementation. The changes observed in patients with LL were as follows: IgM (55% increased production after supplementation and 27% decreased); IgA (63% increased production and 27% decreased); IgG (27% increased production and 63% decreased); and IgE (72% increased production and 28% decreased). On the contrary, in ST patients the following changes were observed: IgM (37% increased production after supplementation and 37% decreased); IgA (28% increased production and 56% decreased); IgG (88% increased production and none decreased); and IgE (37% increased production and 63% decreased).
It was noted that the IgA and IgG levels produced by patients with ST were significantly higher than those identified in patients with LL only after supplementation with Se (P = .0051 and P = .0055, respectively). For IgA, a significant increase in its production after placebo usage was also observed in the ST group when compared to the LL (P = .0011). The same did not occur to the IgM and IgE immunoglobulins. No significant changes in the levels of these antibodies were noted among the groups, regardless of the group evaluated and of the treatment used (Se or placebo).
As indicated in Figure 4, it can be noted that even though the IgA and IgG levels are not statistically different from levels obtained at the beginning of the study and after use of Se supplementation, ST patients showed an inclination toward an increase in the levels of these immunoglobulins when receiving the micronutrient supplementation. The opposite happened with the LL patients, who presented an inclination toward a decrease in the production for both IgA and IgG after having been supplemented with Se.
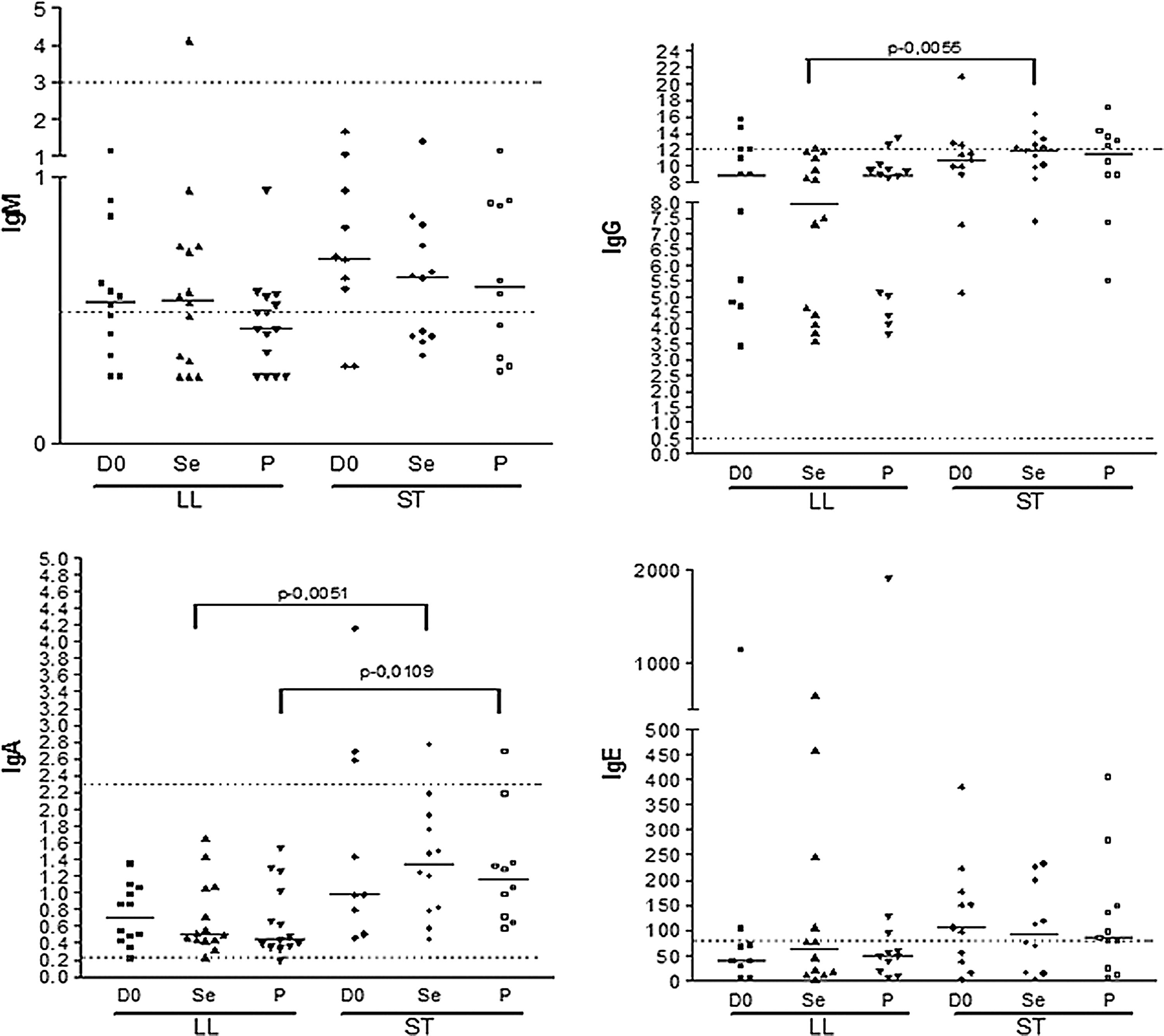
Total levels of immunoglobulins after supplementation. Immunoglobulin levels (IgM, IgG, IgA, and IgE) of 36 patients with LL (n = 17) and ST (n = 19) at the beginning of the study (D0), after 30 days of supplementation with selenium (Se), and after 30 days of supplementation with placebo (P). The dotted lines represent the normal range for each isotype evaluated.
Discussion
In our study, we observed a significant increase in the number of circulating neutrophils in patients with ST after supplementation with selenium. In patients with LL, the increase observed in cell counts of peripheral neutrophils was not significant; however, an inclination toward an increase in the population is clearly noticeable. What is even more important is the individual increase observed in several patients, who had their neutrophil counts raised to values considered normal after Se supplementation. Of the four individuals who showed an increase of neutrophils while using placebo when compared to their supplementation with Se, three received first Se supplementation and later began using placebo. This suggests that there may have been a residual effect from the previous supplementation with the micronutrient in these individuals, thus justifying the sustained neutrophil count. Thus we can say that, as noted by other authors, 22,31,32 selenium usage is able to perform a beneficial role on the viability of neutrophils in patients undergoing conditions of increased oxidative stress, such as the patients we studied. It is noteworthy that new studies should be conducted to assess the function of these cells and identify whether this supplementation influences the chemotaxis and digestion of the material phagocytosed by the cell.
Although we have not evaluated the oxidative burst of polymorphonuclear cells, we believe that the increased blood count of these cells may be associated with an increase in antioxidant enzymes (glutathione peroxidases), which provides added protection against the action of free radicals, a fundamental fact for an increased cell survival. 21,22,32
The decrease in serum levels of selenium can not only lead to the fall in the number of circulating neutrophils but can also cause changes in lymphocyte functions due to a lower bioavailability of the micronutrient. Through studies in mice, it was observed that deprivation of selenium can cause decreased proliferation of T lymphocytes, which can be reversed after restoring levels of the micronutrient. 33 Shrimali et al. 33 demonstrated the fundamental role of selenoproteins on the function of T lymphocytes. According to the authors, individuals subjected to conditions where large amounts of free radicals are produced present functional T-lymphocyte alterations (fall in mitosis), which are reversed after administration of antioxidants. In our study, only the ST patients had positive mean changes (average increase of 100 lymphocytes/mL) after supplementation with selenium. The fact that we have not observed the increase of these cells in the LL group patients is not surprising, as the neutralization of free radicals formed in the tumor tissue (lymphocytes in this case) does not occur or is compromised since the tumor cell is unable to synthesize and concentrate glutathione, even if their precursors (such as cysteine) are present in high amounts. 34 This inability is probably linked to the existence of a blockage in the action of the enzyme that recycles glutathione, oxoprolinase, a situation that makes the lymphocyte cell incapable of neutralizing the acidic environment established as a result of chemotherapy. 35,36
Anemia is a common complication faced by the patients with neoplasms. In cancer patients, the most common causes that tend to be associated with this cytopenia are myelosuppression induced by the cytotoxic treatment, the iron sequestration that makes the metal unavailable for the effective synthesis of the hemoglobin molecule, cell damage caused by oxidative stress, increased RBC destruction (autolysis and splenic hemocatheresis), death of hematopoietic stem cells, and hindrance of erythropoietin-producing cells. 37,38 The analysis of the erythrograms from patients in both groups showed that supplementation performed with neither placebo nor Se was able to promote significant changes in the quantity of hemoglobin, erythrocyte count, or hematocrit percentage. Nevertheless, more than 40% of patients with LL had their levels of hematocrit and hemoglobin raised to values considered normal; and the mean difference (Se-beginning) observed for the group pointed to a slight increase in hematocrit percentage and levels of hemoglobin during the supplementation with Se. Throughout the supplementation with placebo, fewer patients were within normal values for the erythrocyte series and the mean difference (placebo-beginning) had a discreet decrease. For patients with ST, supplementation with Se did not point to an increase in the aforementioned parameters, since supplementation with placebo had the same effect as the one presented by the micronutrient.
Kaushal et al. 39 showed that proper levels of Se are able to prevent autolysis of erythrocytes and formation of methemoglobin in hosts under conditions of great oxidative stress, similar to that identified in our patients, considering the chemotherapy all were undergoing. Thus, the authors indicate that supplementation with the micronutrient can have a positive impact on the number of circulating erythrocytes and, hence, on anemia associated to pathologies in which high concentrations of oxidative radicals and inflammatory conditions coexist. These authors' findings corroborate our data, especially in patients with LL after supplementation with Se. We may have seen only discrete positive results in erythrogram parameters due to the elapsed time of supplementation (30 days) and/or dose of Se used (80% of the daily recommended). According to the review by Almondes, 40 supplementation with the micronutrient must be performed for longer times (more than 60 days) and in much higher doses (at least 200 ug/mL or 2 ug/Kg of patient weight).
There was no significant difference in the production of any of the immunoglobulin isotype (IgE, IgA, IgM, and IgG) in patients with LL or ST after supplementation with Se, compared to the beginning of the study or to when patients received placebo. Despite this, it was observed that the levels of IgG and IgA, after using Se, presented an inclination toward an increase in patients with ST. In contrast, the opposite occurred to the LL patients, who showed an inclination toward a decrease in the production of both IgA and IgG, after supplementation with the micronutrient. Our study is the first to demonstrate that pediatric patients with different tumor types and under chemotherapy respond quite differently; the production of IgG and IgA is statistically different between the two evaluated groups when patients are supplemented with Se.
In the research conducted by Pettingale 41 and the study of Roberts et al., 42 it is clear that patients with breast tumors had elevated circulating IgA levels. As proposed by the authors, the elevation of this antibody may be related to or an indication (marker) of metastasis development. De Souza et al. 43 showed that patients with mouth and oropharyngeal cancers produce IgA serum concentrations equivalent to normal subjects. At no time did these authors identify a modification in the production of this immunoglobulin despite the disease. At first, the concept proposed by the authors did not apply to our patients, since the pediatric cancer cannot be compared to that precipitated in adults and we did not identify any correlation between clinical deterioration of the patients and IgA levels detected.
In a comprehensive review of literature on the immune response in patients with leukemia, Martín Ibáñez et al. 44 showed that, in general, production of antibody of all classes appears preserved in patients at the moment of diagnosis. However, these authors state that several patients progress to production of immunoglobulin serum levels considered abnormal (below the normal range). In our study, we observed that the global production of immunoglobulins, except for IgM, was preserved in all patients with LL and ST, despite supplementation or chemotherapy. It is noteworthy that the production assessed in our study did not aim to detect antigen-specific antibodies, particularly for vaccine antigens to which patients had already been sensitized. In future studies, it would be important to identify the specificity of antibodies found to establish whether their production is due to nonspecific polyclonal stimulation and associated to the inflammatory response resulting from chemotherapy and/or stimulation associated with exposure to tumor antigens arising from the death of the target cells for the applied treatment.
Epidemiological studies have suggested a positive association between atopy and protection against the development of malignancies. 45 –47 The inverse association between IgE production levels and risk for developing diseases, such as leukemia, lymphoma, glioma, pancreatic cancer, among others, has been extensively evaluated. 48 –53 Jensem–Jarolin et al. 45 showed that, in conditions where serum IgE are directed against tumor-associated antigens, these immunoglobulins could be considered as mediators of cell–cell contact where the tumor cell would be recognized by the immune effector cell resulting in an immune synapse known as antibody-dependent cytotoxicity (ADCC). Another antitumor mechanism attributed to IgE is the facilitation of phagocytosis known as antibody-dependent cellular phagocytosis. Given that the binding of IgE to its FceRI receptor (expressed in effector cells such as eosinophils and basophils) is considered of high affinity when compared to other receptors with the same function, binding of the antitumor antigen IgE to its cellular receptors could be more effective than the action itself of antibodies such as IgG or IgM. Thus, the simple observation that increased levels of IgE antibodies can be understood as a beneficial control mechanism of the development of tumors leads us to ask whether there is any correlation between a better disease prognosis (in this case, the evolution of the tumor diagnosed) and levels identified in the evaluated patients.
In this study, median levels of IgE production in patients with LL, regardless of the treatment (placebo or Se), were below the maximum detection limit considered normal; however, with an inclination to increase after using Se. The supplementation has also identified an extremely high negative correlation (r = −1) between IgA and IgG levels when compared to IgE levels.
Patients with ST showed the median IgE production, regardless of the group in question (supplemented with selenium or placebo), above the limits considered normal; about more than half of the patients had their IgE levels considered high (77% at the beginning of the protocol, 50% with selenium, and 88% with placebo). According to study by Fu et al., 54 IgE production must have a much broader biological effect than the actions already known in atopic and parasitic diseases. After evaluating the production of IgE in patients with pancreatic cancer, the authors identified not only a raise in the production levels of the immunoglobulin but also elegantly demonstrated the role of this immunoglobulin in the ADCC mechanism. In fact, in previously conducted researches, the authors noted that IgE has antiviral action, acting effectively. 55 Similarly, in two of his studies, Karagiannis et al. showed that IgE antibodies are able to increase the survival of animals bearing ovarian carcinoma through the ADCC mechanism against tumor cells. 56,57
In our study, we did not assess the specificity of IgE antibodies, and thus, it is not possible to associate the production of this antibody to protection mechanisms against tumor cells in the patients studied. Analyzing the IgE levels we can suggest that, despite not pointing to statistically significant differences, supplementation with Se appears to induce elevation of the IgE molecule production in LL carriers and not affect the concentration of this immunoglobulin in ST patients. It is made extremely relevant to research the targets for these immunoglobulins to determine whether this tendency to increase could favor the immune effector mechanisms directed against the tumor, as well as the impact of this mechanism on the disease control.
All individuals from the LL group who had raised IgE production during supplementation with placebo, when levels were compared to the supplementation period with Se, had first been supplemented with the micronutrient. This leads us to suppose that it is a residual effect of restoring the levels of Se in the body of these patients, an effect that may have even perpetuated during the placebo group stage. In patients with ST, something similar was also observed, since of the six patients with increased production of immunoglobulins while using placebo, four had started their treatment using Se.
Conclusion
In our study, we observed that supplementation with Se for only 30 days is able to reduce the advent of neutropenic cases in patients with LL and ST during chemotherapy, can promote immunomodulation of the humoral immune response differently in patients with LL and patients with ST, reduces levels of IgG and IgA, increases levels of IgE in patients with LL, and determines a mild increase in hematocrit and hemoglobin of patients.
Footnotes
Acknowledgment
Support by FAPESP grant n. 2012/13871–7.
Author Disclosure Statement
No competing financial interests exist.