
Abstract
The aim of this study was to examine the efficacy of combined grape pomace and omija fruit ethanol extracts (GO) on metabolic disorders in overweight or obese subjects. Seventy-six subjects (30–70 years, body mass index ≥23.0 kg/m2) were divided into control (starch, 4 g/day, n = 24), low-GO (low dose GO, grape pomace extract [342.5 mg/day] + omija fruit extract [57.5 mg/day], n = 26), and high-GO (high dose GO, grape pomace extract [685 mg/day] + omija fruit extract [115 mg/day], n = 26) groups. Body composition, nutrient intake, plasma lipid profiles, inflammation, antioxidant capacity, and hepatotoxicity markers were assessed in all subjects at the baseline and 10 weeks after taking the supplements. The body weight and body fat of overweight or obese subjects was not significantly altered in the low-GO and high-GO groups. However, the high-GO supplement significantly decreased the baseline-adjusted final plasma total-cholesterol, low-density lipoprotein (LDL)-cholesterol, and non–high-density lipoprotein (HDL)-cholesterol levels and increased the baseline-adjusted final plasma apolipoprotein (apo) A-1 level compared with that of the control group. In addition, the high-GO supplement significantly lowered apo B, apo B/apo A-1, lipoprotein a (Lp[a]), atherogenic index, interleukin (IL)-1β, tumor necrosis factor-α, and elevated erythrocyte antioxidant capacity compared with the control group or the baseline levels. The low-GO supplement decreased the plasma IL-1β level and elevated erythrocyte superoxide dismutase activity compared with that at baseline. However, in general, high-GO exerted a greater effect than low-GO. There were no significant differences in activities of plasma glutamate oxaloacetate transaminase and glutamate pyruvate transaminase between the groups. This study is a preliminary clinical study to verify that GO could be beneficial for amelioration of obesity-related dyslipidemia, inflammation, and oxidative stress without side effect in the overweight or obese subjects.
Introduction
O
In recent years, the importance of biologically active substances in foods used as nutraceuticals has been recognized. Recently, several antiobesity drugs have been withdrawn from the market due to potentially hazardous side effects. 6 Some nutraceuticals have been reported to modulate adipocyte apoptosis and differentiation, and ameliorate inflammation and oxidative stress in obesity. 7 Grapes are generally cultivated for the wine industry, which generates large amounts of grape pomace that consists of skins, seeds, and stems as industrial waste. About 70% of the grape polyphenols remain in the pomace making it a beneficial source of health-promoting nutraceuticals. 8 Several studies have reported that grape pomace contains antioxidants and alleviates oxidative stress and chronic inflammation. 9 –11 Moreover, grape seed extract supplements decreased body weight and lipid levels in the plasma and liver by altering lipid metabolism. 12,13 Furthermore, grape skin extract protected against diet-induced adiposity by regulating lipogenesis and fatty acid oxidation. 14 Several clinical studies have reported that grape seed extract significantly improved markers of inflammation and oxidative stress and influenced vascular function in human, which suggest it may have a therapeutic role in inflammation-mediated disease such as cardiovascular disease. 15 –17 Schizandra chinensis Baillon, which is known as omija in South Korea, is another potential source of antiobesity nutraceuticals. The seeds and fruits of omija have been used in traditional alternative medicines for dry cough, asthma, night sweats, nocturnal seminal emissions, and chronic diarrhea. 18 –20 A recent study has reported that phenolic phytochemicals from omija displayed high antioxidant activity and anti-inflammatory effects in in vitro and in vivo models. 21,22
The results of our recent studies have demonstrated the mechanisms of antiobesity and antidiabetic actions of combined grape pomace and omija fruit ethanol extract (GO) in high-fat diet-induced obese mice and type 2 diabetic db/db mice. 23,24 This study is a preliminary clinical study to examine the efficacy of GO on metabolic disorders in overweight or obese subjects. Therefore, we investigated the effect of two doses of GO supplementation for 10 weeks on body composition, plasma lipids, inflammation, or oxidative stress.
Materials and Methods
Preparation of GO
Grapes (Vitis vinifera) and omija (S. chinensis Baillon) were purchased from Gyeongsangbuk-do, Korea. GO was prepared according to the method of Cho et al. 23 GO powder was carefully mixed, purified, and coated for clinical study. Table 1 presents yields and compositions of the functional ingredients in GO.
Subjects and design
Male and female volunteers aged 30–70 years old were recruited in Daegu city and its suburbs in the Republic of Korea. After an initial screening, 76 subjects with body mass index (BMI) ≥23 kg/m2 were selected. All selected participants had no chronic disease, infectious diseases, pregnancy, or recent surgery. The study was performed in accordance with the Declaration of Helsinki. The study was approved by the Kyungpook National University Human Research Committee (KNU 2012-6).
This study was a randomized, double-blind, placebo-controlled trial to determine the effectiveness of GO on body composition, plasma lipid profiles, inflammation, and antioxidants in overweight or obese subjects. All subjects were randomly divided into three groups: (1) control (placebo, starch, 4 g/day, n = 24); (2) low-GO (low dose GO, grape pomace extract [342.5 mg/day] + omija fruit extract [57.5 mg/day], n = 26); and (3) high-GO (high dose GO, grape pomace extract [685 mg/day] + omija fruit extract [115 mg/day], n = 26). They were instructed to maintain their routine food intake and physical activity during the study and consumed two capsules containing the supplements twice daily for 10 weeks. The doses of GO were decided based on a previous animal study. 23
Study protocols
Fasting blood samples collected at the baseline and after 10 weeks of supplementation were drawn into heparin-coated tubes, centrifuged at 1000 g for 15 min at 4°C, and stored at −70°C. Body compositions were measured using the X-Scan plus II body composition analyzer (Jawon Medical Co. Ltd., Daejeon, Korea). Waist and hip circumferences were measured with an anthropometric tape. For the analysis of abdominal fat, seven subjects in each group were randomly chosen. Abdominal fat was measured using multi-detector computed tomography (Sensation 16/64; Siemens, Munich, Germany). Blood pressure (BP) was measured using an automatic BP monitor (Omron, Osaka, Japan). Food intake was recorded before and during the nutritional intervention trial using a 24-h dietary recall. Nutritional analysis was performed using CAN-Pro 3.0 software (The Korean Nutrition Society, Seoul, Korea).
Analysis of plasma markers
Plasma triglyceride, total-cholesterol, HDL-cholesterol, aspartate transaminase (AST), alanine transaminase (ALT; Asan, Seoul, Korea), apolipoprotein (apo) A-1, and apo B (Nittobo, Tokyo, Japan) were determined using commercial kits. Plasma lipoprotein (a) (Lp[a]; Elabscience, Beijing, China) and C-reactive protein (R&D Systems, Inc., Minneapolis, MN, USA) were determined using a Sandwich-ELISA kit. The LDL-cholesterol level was calculated using the Friedewald formula
25
:
The non–HDL-cholesterol was calculated as (total cholesterol – HDL-cholesterol). The atherogenic index (AI) was calculated as
Analysis of erythrocyte markers
The activities of superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GSH-Px), and glutathione reductase (GR) were determined according to the methods of Marklund, 26 Aebi, 27 Paglia and Valentine, 28 and Pinto and Bartley, 29 respectively. The erythrocyte thiobarbituric acid-reactive substances (TBARS) and H2O2 levels were measured using the methods of Tarladgis et al. 30 and Wolff, 31 respectively.
Statistical analysis
All data are presented as mean ± SD. Statistical analysis was performed using SPSS software (version 11.5, SPSS, Inc., Chicago, IL, USA). Significant changes within each group between baseline and 10 weeks were assessed using paired t-test. Differences between the three groups at baseline and 10 weeks were analyzed using one-way analysis of variance (ANOVA), followed by post hoc Duncan's multiple range tests. Differences were considered statistically significant at P < .05.
Results
Baseline clinical characteristics and nutrient intakes
In both males and females, there were no significant differences in age, height, systolic BP, diastolic BP, and fasting blood glucose (FBG) between the groups before the trial (Table 2). Analysis of 24-h dietary recalls from the subjects indicated no significant differences in nutrient intakes between the three groups at baseline or after 10 weeks of supplementation (Table 3).
Mean ± SD.
Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts; BP, blood pressure; FBG, fasting blood glucose; SD, standard deviation.
Mean ± SD.
Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts.
Body composition
There were no significant differences in body weight, BMI, body fat percentage (BFP), muscle weight, waist circumference, hip circumference, or waist-hip ratio (WHR) between the groups before and after 10 weeks of supplementation (Table 4). However, after 10 weeks of supplementation, the BFP of the high-GO group was lower than baseline levels (P = .100). There were no significant differences in total abdominal, subcutaneous and mesenteric fat areas before and after 10 weeks of supplementation between the three groups or within each group (Table 5). Representative abdominal fat computed tomography (CT) scans in each group revealed that the two doses of GO tended to lower the total abdominal, subcutaneous, and mesenteric fat compared with the baseline values (Fig. 1).

Effects of high and low dose of grape pomace and omija fruit extract on changes in abdominal fat assessed by computed tomography in subjects after a 10-week intervention trial. Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts.
Mean ± SD.
ANOVA among the three groups.
t-Test between before and after trial in each group.
Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts; ANOVA; analysis of variance; BMI, body mass index; BFP, body fat percentage; WHR, waist-hip ratio; BP, blood pressure.
Mean ± SD.
ANOVA among three groups.
t-Test between before and after trial in each group.
Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts.
Plasma lipid profiles
Optimal values of plasma lipids defined by the National Cholesterol Education Program (NCEP) 32 were as follows: triglyceride <150 mg/dL (1.7 mmol/L), total-cholesterol <200 mg/dL (5.17 mmol/L), and LDL-cholesterol <130 mg/dL (3.36 mmol/L). In this study, at baseline and after 10 weeks supplementation, the plasma triglyceride concentrations of the three groups were lower than optimal value. The total-cholesterol and LDL-cholesterol levels of the three groups were higher than optimal value.
Plasma triglyceride, total-cholesterol, non–HDL-cholesterol, LDL cholesterol, and apo A-1 concentrations were not significantly different between the three groups at baseline and after 10 weeks supplementation (Fig. 2). However, after 10 weeks supplementation, total-cholesterol (P = .040), non–HDL-cholesterol (P = .026), LDL-cholesterol (P = .042), and apo A-1 (P = .045) concentrations of the high-GO group were significantly decreased compared with the control group by Student's t-test analysis. The HDL-cholesterol was not significantly different between the groups at baseline and after 10 weeks supplementation.
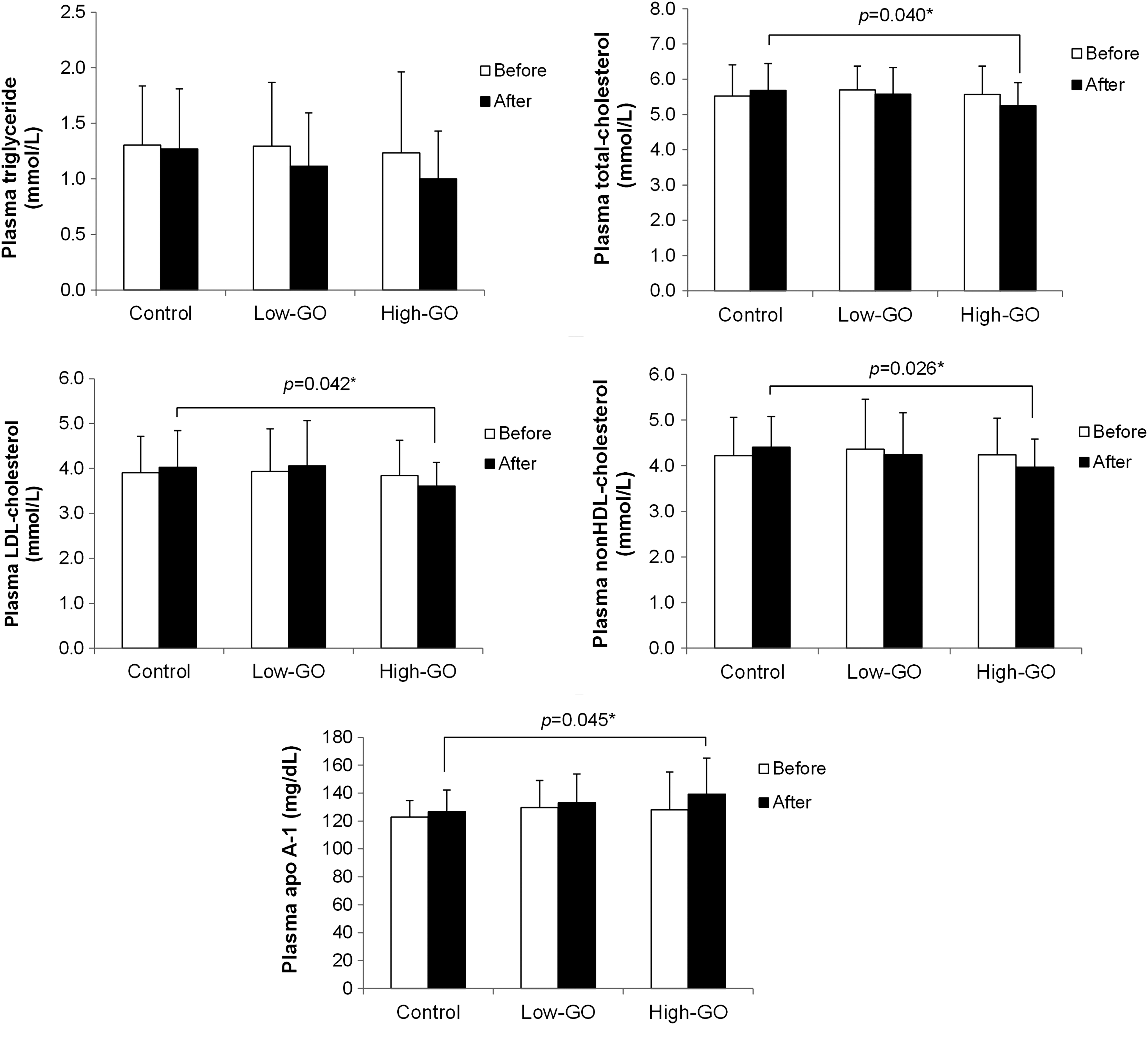
Changes in plasma lipid concentrations by high and low doses of grape pomace and omija fruit extract in subjects after a 10-week intervention trial. Mean ± SD. Significant differences between high-GO group versus control group are indicated as P value (*P < .05). Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts.
The baseline-adjusted final concentrations of total cholesterol, non–HDL-cholesterol, and LDL-cholesterol were significantly lower in the high-GO group compared with the control group (Fig. 3). The baseline-adjusted final concentration of apo A-1 significantly increased in the high-GO group compared with the control group. Furthermore, the plasma apo B concentrations and apo B/apo A-1 ratios significantly decreased in the high-GO group compared with the control and low-GO groups (Table 6). After the 10-week trial, plasma Lp(a) concentrations were significantly reduced in the high-GO group compared with the baseline levels. There was no significant difference in the AI levels between the three groups before or after the trial. However, AI levels were significantly lower in the high-GO group compared with the control group, based on a Student's t-test analysis (P = .046).

Effects of high and low dose of grape pomace and omija fruit extract on changes in plasma lipid profiles in subjects after a 10-week intervention trial. Mean ± SD. abMeans not sharing common letters that are significantly different among groups at P < .05. Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts.
Mean ± SD.
ANOVA among three groups (abmeans not sharing common letters are significantly different between three groups before and after trial at P < .05).
t-Test between before and after trial in each group (significant differences are indicated; * P < .05).
Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts; Apo, apolipoprotein; Lp(a), lipoprotein (a); AI, atherogenic index.
Antioxidant enzyme activities and lipid peroxidation contents in erythrocytes
After 10 weeks of supplementation, the activity of SOD in erythrocytes was significantly elevated in the low-GO and high-GO groups compared with the baseline (Fig. 4). In particular, the high-GO significantly elevated GSH-Px and GR activities compared with the baseline values and the control group. Erythrocytic TBARS and H2O2 concentrations also significantly decreased in the high-GO group compared with the baseline values and the control group.

Effects of high and low dose of grape pomace and omija fruit extract on changes in erythrocytic antioxidant activities in subjects after a 10-week intervention trial. Mean ± SD. Significant differences between before and after trial within each group are indicated as P value (*P < .05, **P < .01, ***P < .001), absignificant differences among the three groups before and after trial at P < .05. Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extracts; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extracts; SOD, superoxide dismutase; CAT, catalase; GSH-Px, glutathione peroxidase; GR, glutathione reductase; TBARS, thiobarbituric acid-reactive substances.
Plasma inflammatory cytokine and hepatotoxicity markers
Supplementation of high-GO for 10 weeks significantly decreased plasma IL-1β and TNF-α, and tended to lower IL-6 levels by 36% compared with the baseline values (Table 7). Low-GO also significantly decreased plasma IL-1β after 10 weeks of supplementation compared with the baseline values. The levels of hepatotoxicity markers, such as plasma AST and ALT, were not significantly different between the groups.
Mean ± SD.
ANOVA among three groups.
t-Test between before and after trial in each group (Significant differences are indicated; * P < .05, *** P < .001).
Control, Starch; Low-GO, low-dose mixture of grape pomace (342.5 mg/day) and omija fruit (57.5 mg/day) ethanol extract; High-GO, high-dose mixture of grape pomace (685 mg/day) and omija fruit (115 mg/day) ethanol extract; IL, interleukin; TNF, tumor necrosis factor; AST, aspartate transaminase; ALT, alanine transaminase.
Discussion
This study was a preliminary clinical study to verify that GO could improve plasma lipid profiles, inflammation, and antioxidant capacity without causing side effects in overweight or obese subjects.
The control, low-GO, and high-GO groups had similar baseline characteristics such as age, BMI, BFP, WHR, and FBG. There were no significant differences in energy and nutrient intakes between the three groups during the trial. Therefore, GO supplementation may not affect energy and nutrient intakes in subjects. To investigate the antiobesity effect of GO, anthropometric parameters and body composition of all subjects were measured. BMI has been used by many investigators for estimating body fat. 33 However, BMI is unreliable for estimating body fat since body weight is the sum of fat, muscle, visceral organs, and bone. 34 Individuals with the same BMI can have a wide variability in body fat. For example, Asians have a lower BMI but higher BFP than Caucasians of both sexes. 35 WHR and waist circumference are beneficial markers of abdominal fat compartments and are used in the diagnosis of metabolic syndrome. 36 In this study, there were no significant differences in the body weight, BMI, waist circumference, or WHR between the three groups. However, BFPs of the high-GO supplemented group were lower than the baseline levels (p = .100), but this difference was not statistically significant. In addition, a CT scan indicated that in the high-GO group, the total abdominal fat decreased by 11% compared with the baseline values, whereas the total abdominal fat of the control group increased by 4% compared with the baseline values. An optimal technique for an accurate assessment of abdominal fat is a CT scan directly measured at the umbilicus. 36 CT is expensive and complicated, requiring expert skills; however, for assessing body composition, CT has proven to be more accurate than the results from anthropometry. 37
Lipid profiles, including levels of HDL-cholesterol, LDL-cholesterol, and triglycerides, aid the assessment of CHD risk. 38,39 In particular, a review of clinical studies reported that LDL-cholesterol was a strong predictor of cardiovascular disease (CVD) and a 10 mg/dL increase in LDL-cholesterol was associated with an ∼12% increase in CVD risk. 40 In a previous study, supplementation with grape polyphenols (using lyophilized grape powder 36 g/day) for 4 weeks was effective for lowering plasma triglyceride, LDL-cholesterol, and apo B levels in pre- and postmenopausal women. 41 In another study, supplementation with omija extract (3, 6 g/kg) for 5 weeks reduced total lipid, total-cholesterol, triglyceride, phospholipid, very low density lipoprotein, and LDL levels in diet-induced hyperlipidemic rats. 42 In this study, the baseline-adjusted final total-cholesterol and LDL-cholesterol levels were significantly lower with high-GO supplementation. In contrast, the low-GO supplementation appeared to be ineffective in reducing plasma total-cholesterol and LDL-cholesterol levels compared to the control group.
Non–HDL-cholesterol has been proposed as a substitute for apo B measurements and is a better marker for cardiovascular risk than LDL-cholesterol. 43,44 In this study, the high-GO supplementation significantly reduced the baseline-adjusted final plasma non–HDL-cholesterol and final plasma apo B levels compared with the control group. Similarly, a previous study reported that supplementation with grape extract (one capsule with 350 mg containing 8 mg resveratrol/day) for 6 months decreased oxidized LDL and apo B levels in patients undergoing primary prevention of CVD. 45 In addition, we found that the high-GO group significantly increased the baseline-adjusted final plasma apo A-1 concentrations and decreased final plasma apo B/apo A-1 ratios compared with the control group. Levels of plasma apo A-1, the major HDL protein constituent, is more useful than HDL-cholesterol for assessing coronary-artery disease, 46 and the apo B/apo A-1 ratio is an important clinical indicator of metabolic syndrome and cardiac risk. 47,48 Lp(a) is closely linked to coronary atherosclerosis and is an independent risk factor for myocardial infarction. 49,50 A high AI also predicts obesity, hyperinsulinemia, diabetes, and vascular events. 51 In this study, supplementation with high-GO significantly decreased plasma Lp(a) and AI levels compared with the baseline or control group. Taken together, our findings suggest that high-GO may have a beneficial role for preventing obesity-related CVD.
Obesity is a low-grade inflammatory state. Increased production of IL-6, which is an inflammatory cytokine, is associated with obesity and plays a role in the development of CVD. 52 Plasma IL-6 levels were lowered with high-GO supplementation compared with the baseline values in our study. Furthermore, production of TNF-α and IL-1β by adipose tissues was increased in obesity and these cytokines contribute to CVD. 53,54 In this study, the high-GO supplement significantly decreased plasma TNF-α and IL-1β concentrations compared with the baseline values. Additionally, the low-GO supplement significantly reduced plasma IL-1β concentrations compared with the baseline. A previous study demonstrated that in high-fat diet-induced obese mice, GO significantly reduces mRNA expression of inflammatory genes (NF-κB, MCP-1, TNF-α, and IL-6) in the liver and epididymal white adipose tissue, along with levels of plasma inflammatory cytokines (MCP-1, TNF-α, and IL-6), suggesting that this may be one potential mechanism for preventing diet-induced obesity. 24
Increased oxidative stress in adipose tissue has been implicated as an initiator of metabolic syndrome associated with obesity. 5 Reactive oxygen species (ROS)-induced oxidative stress promotes tissue injury, but tissues can be protected from ROS damage by antioxidant enzymes. 55 Among the antioxidant enzymes, SOD catalyzes the dismutation of the superoxide anion to H2O2, so that CAT and GSH-Px can break down H2O2. GSH-Px also oxidizes glutathione to glutathione disulfide (GSSG). The reduction of GSSG to GSH can then be catalyzed by GR. In general, levels of plasma TBARS, a marker of lipid peroxidation caused by oxidative injury, are significantly correlated with BMI and waist circumference. 5 The evidence for the antioxidant capacity of grape pomace is largely derived from animal studies 9,56 and human trials. 57 In addition, omija exhibits antioxidant activity. 58 In this study, the high-GO supplement significantly elevated erythrocyte SOD, GSH-Px, and GR activities and lowered TBARS and H2O2 concentrations compared with the control group or baseline levels.
AST and ALT are clinical markers for liver function and are elevated in obesity, fatty liver disease, metabolic syndrome, and CVD. 59 –61 In this study, no subjects reported adverse side effects due to GO supplementation. Plasma AST and ALT levels were within normal ranges before and after the trial in all of the groups; the GO supplement did not significantly alter plasma hepatotoxicity marker levels in any subjects.
Several limitations of this clinical study should be emphasized. Subjects of this study were restricted to volunteers, and it is difficult to represent the general population in this small sample size. During the 10-week period, we instructed the subjects to maintain routine food intake and physical activity, but we had no monitoring system except for telephone conversations. In addition, sex differences may influence plasma lipid levels due to hormonal changes during this study. Plasma cholesterol, triglyceride, and HDL-cholesterol are reported to vary between 5% and 8% in the follicular phase of the menstrual cycle compared with the luteal phase. 62 Moreover, the present clinical study used a smaller dose of GO than an extrapolated dose from our previous animal study due to handling problems during the encapsulating procedures. These may partly contribute to the lack of effectiveness of GO on body composition in the human trial.
In conclusion, despite these limitations, we have demonstrated that GO could be beneficial for amelioration of obesity-related dyslipidemia, inflammation, and oxidative stress in overweight or obese subjects. Further larger-scale and longer-term studies are needed to establish long-term effectiveness and the optimal dose of GO in humans.
Footnotes
Acknowledgment
This research was supported by the High Value-added Food Technology Development Program (No. 110129-3), the Ministry for Food, Agriculture, Forestry, and Fisheries.
Author Disclosure Statement
No competing financial interests exist.