
Abstract
Ulcerative colitis and Crohn's disease are two major forms of the inflammatory bowel diseases (IBDs). Vitamin A (VA) and vitamin D (VD) may be associated with reduction in inflammation in these disorders. The aim of this review was to show the current evidence that may associate VA and VD with IBDs. Data linking VA, VD, and IBDs were studied. Both VA and VD may be related to the immune system in different manners. The active form of VA, retinoic acid, may be related to the growth factor-β and release of interleukin-10 (IL-10), thus involved with the resolution of the inflammation. Its deficiency is associated with the increase of disease activity. The active form of VD is 1,25(OH)2D3 that produces biological effects via the nuclear hormone receptor named VD receptor (VDR), which may interfere with the immune cells and macrophages leading to the suppression of the inflammatory process by decreasing the release of TNF-α, IL-1, IL-6, and IL-8, IL-12, and IL-23. VDR may also activate nucleotide-binding oligomerization domain 2 expression and stimulate the production of the defensin and cathelicidin that are important to the homeostasis of the mucosal immune barrier. The use of VA and VD could be helpful in the treatment and prevention of IBDs but more studies are necessary to establish the precise role of these compounds in the prevention or remission of these inflammatory processes.
Introduction
T
IBDs have been increasing over the past 50 years and pieces of evidence show that the incidence is higher in developed countries. Aspects such as genetics, excessive intake of sugars, fats, food additives, reduction in the consumption of fibers, smoking, infections, and psychological factors may work as a trigger for the occurrence and recurrence of these conditions (Fig. 1). 2 –5

Triggering factors for IBD and some of the major symptoms related to the patients. IBD, intestinal bowel disease.
As we may see in Figure 1, the consequences of the chronic inflammatory condition trigger abdominal pain, diarrhea, bleeding, higher risk of bowel cancer, and extra intestinal manifestations. This panorama may occur in young and adults, leading to a prolonged course and recurrence, which interferes directly in the quality of life. 6 –8
The heterogeneous nature of IBDs makes necessary a multidisciplinary approach for the treatment of the patient. The importance of pharmacotherapy is indisputable, but many patients require other kinds of interventions to induce and maintain remission and improve the quality of life. The use of some compounds such as antioxidants and vitamins may help in this scenario. 9
Some authors have shown that vitamin A (VA) decreases inflammatory process in many diseases as well as in bowel inflammation progression. Other studies show that vitamin D (VD) also plays a role in the inflammatory conditions and may deeply influence the incidence and progression of IBDs. 1,2,5,9 –14 Based on these findings, the aim of this review was to make some reflections about IBDs and the role that VA and VD may play in the inflammatory process.
Materials and Methods
This review was performed using articles linking VA, VD, and IBDs. Databases such as Medline, Scielo, and Lilacs were consulted and a retrospective search was done to find relevant studies with humans and animal models.
Ulcerative colitis, Crohn's disease, and activation of the immune system
Ulcerative colitis (UC) and Crohn's disease (CD) are the major forms of IBDs and include a chronic and complex relapsing inflammatory process that may deeply interfere in the gastrointestinal homeostasis. They may be considered as possessing multifactorial autoimmune aspects but with similar risk factors such as the imbalance in the bowel epithelial barrier, genetic predisposition, stress, clinical, endoscopic, and histological aspects, and may differ, for example, in the area of the gastrointestinal tract that may be affected. Figure 2 shows the similarities and the differences between CD and UC. 2,5,7,15 –18

Comparison between Crohn's disease and ulcerative colitis: similar and nonsimilar aspects.
Although CD may manifest from mouth to anus, the inflammation of the ileum is the most common and occurs possibly by an idiopathic transmural inflammation process that affects all the wall layers. The pattern of skipped areas of inflammation may be observed and may result in ulcerations with “fistulizing, stricturing, or inflammatory pattern in the perianal region and abdominal wall.” 19,20
In UC, inflammation may be seen as a polymorphonuclear infiltration with cryptic abscesses, edema, and congestion and it may start in the rectum and extend uniformly throughout the colon. It is normally restricted to the mucosal surface, and the pattern of this condition is stratified by the extension of the colon that is involved, resulting in proctitis, left colitis, or pancolitis, and rarely affecting the terminal ileum. 21
In UC patients, T-helper 2 (TH2) cells are activated in the lamina propria, resulting in activation of B cells, macrophages, and inflammatory leukocytes. In CD patients, TH1 cells are mainly responsible for the immunological reaction that is induced by the release of interleukins and gamma-interferon (IFN-γ). 22
The inflammatory process initiates after the disruption in the homeostasis of the gastrointestinal system, resulting in the imbalance in mucinous layer and activation of the toll-like receptor leading to an increase of the permeability and consequent bacterial translocation into the intestinal mucosa. This drives to an activation of the immune system with involvement of dendritic cells, macrophages, neutrophils, T and B cells, and activation of the proinflammatory transcription factor known as nuclear factor kappa beta (NFκβ) that initiates many transduction signs, leading to the overproduction of inflammatory mediator cytokines and chemokines such as the tumor necrosis factor-α (TNF-α) and interleukin-1β (IL-1β), IL-5, IL-6, and IL-13 (Fig. 3). This chronic inflammatory process is responsible for the main symptoms of CD and UC (Fig. 2). 2,5,22 –25
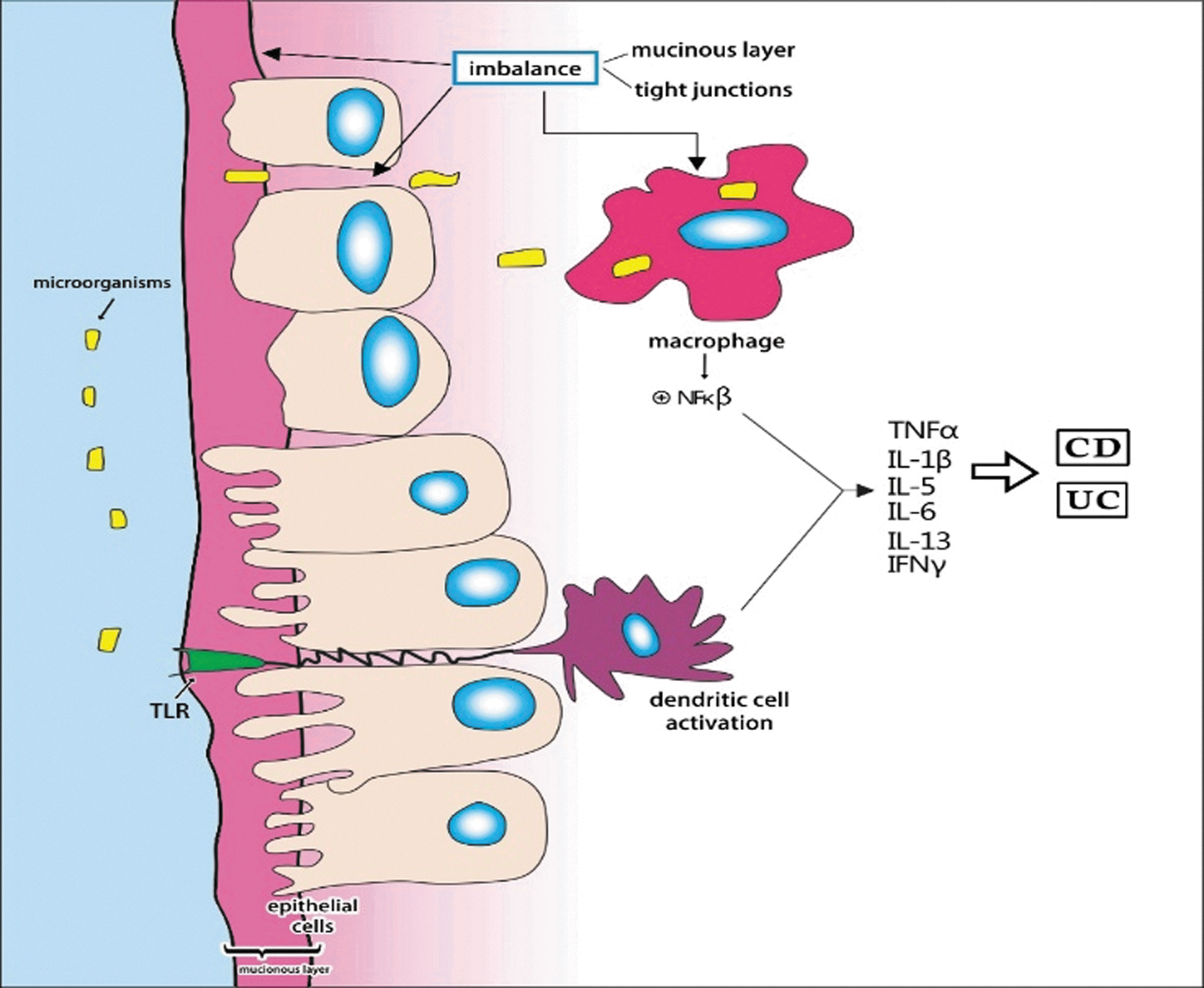
Pathophysiology in the inflammatory bowel disease: the imbalance in mucinous layer increases the uptake of the microorganisms with activation of the TLRs, dendritic cells, macrophages, and NFκβ, resulting in higher release of the proinflammatory mediators such as TNF-α, interleukins (IL-1β, IL-5, IL-6, IL-13), and IFN-γ. IFN-γ, gamma-interferon; NFκβ, nuclear factor kappa beta; TLRs, toll-like receptors; TNF-α, tumor necrosis factor α. Modified from Ordas et al. (2012) and Neurath (2015). 5,24
Vitamin A
VA is one of the fat-soluble vitamins critical for health in humans and other mammals. It includes retinol and retinyl esters that are not biologically active and need oxidation by enzymes to produce retinoic acid (RA). Typically, VA is involved in a wide range of biological processes, including the immune system and development and function of almost every cell linked to protective or regulatory adaptive or innate immunity. Most effects of VA are produced by its metabolite, RA, that is capable of binding to nuclear receptors and promote transcriptional expression of RA target genes. It may exert a protective role against free radicals and oxidative stress and has a potential role in the inflammatory processes. RA includes five chemical isomers from which the all-trans-RA (atRA) is considered to be the biologically active form. 12,25,26
Some studies have found that patients with CD possess increased incidence of VA deficiency. Furthermore, deficiencies in this kind of antioxidant may enhance the imbalance between the formation and destruction of free radicals in the intestinal mucosa of CD patients. 27
In UC patients, the authors have observed that serum levels of VA were related to increased disease activity and it is established that VA can inhibit TH17 (T helper 17) responses both in mice models and in humans. 9
Reifen et al. 10 verified that an animal model for colitis treated with VA preserved the colonic tissue architecture, and did not present vasculitis or necrosis. They also observed reduction in the myeloperoxidase activity and protection of the mitochondria (in colitis there is arrest of mitochondrial respiration, decrease in the mitochondrial DNA, and production of proteins). The authors have concluded that this vitamin may play an important role as therapeutic agent in IBDs.
Research using cells from UC patients and in vivo mouse studies showed that higher amounts of atRA may overcome the imbalance in the immune system and improve the inflammatory process by decreasing activation of NFκβ and releasing TNF-α. It may also improve the symptoms of inflammation by reducing the neutrophils infiltration and downregulated IL-17, returning to the immunologic balance. The nuclear receptor RARα was implicated in regulating these RA effects, suggesting that higher levels of atRA are effective in stopping the acute inflammatory response in IBDs. 12,13,28
As already mentioned in IBDs, the proinflammatory and anti-inflammatory cytokines may be released by many cells of the mucosal immune system after a trigger situation (macrophages, neutrophils, dendritic cells, TH1, TH2, TH17, and T regulatory cells, Tregs). The inflammation process in the patients depends on the balance between proinflammatory and anti-inflammatory cytokines. RA may be related to the production of the transforming growth factor-β (TGF-β) and IL-10, helping in the resolution of the inflammation condition. 24,29
Vitamin D
VD is a fat-soluble hormone known as playing an important role in the bone metabolism. However, many studies have shown that it is associated with the immune response and gastrointestinal function. This hormone may be ingested with the diet or may be synthesized in the skin under exposure to sunlight. It may be found in two forms called ergocalciferol (VD2) when synthesized by plant and fungus and cholecalciferol (VD3: 1,25-dihydroxyvitamin D3 (1,25(OH)2D3) when produced in the skin. In this last case, a compound known as 7-dehydrocholesterol is activated by the ultraviolet light, resulting in pre-VD and after VD3. Further modifications in the molecule are provided in the liver and kidney (Fig. 4). The active form of VD (1,25(OH)2D3) is related to the biological effects, thanks to a member of the nuclear hormone receptor named VD receptor (VDR). 2,30,31
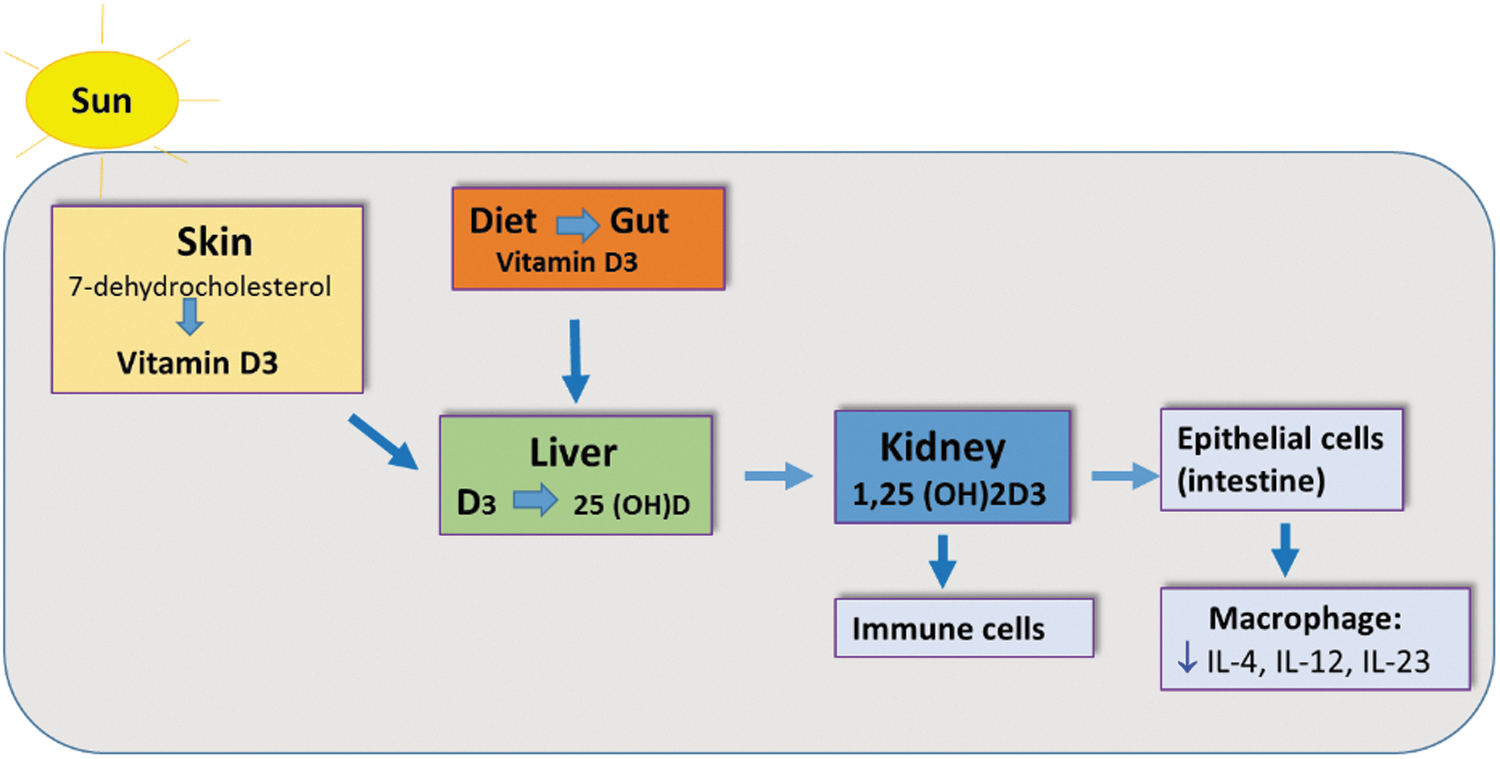
Vitamin D may be obtained from diet or under exposure to sunlight by the conversion of 7-dehydrocholesterol to previtamin D3 and vitamin D3. The active form (1,25(OH)2D3) may suppress inflammation process by reducing the production of proinflammatory interleukins. Modified from Reich et al. (2014). 31
VDR plays roles such as immune-modulating, anti-inflammatory, prodifferentiating, and antimitotic, possibly because of the several genes that express VD responsive elements. The literature gives many studies showing that VD may influence the immune cells and macrophages, leading to the suppression of the inflammatory process by decreasing IL-6, IL-12, and IL-23. Furthermore, it may lead to modifications in the gut microbiome in the upper gastrointestinal tract (gastric corpus, antrum, and duodenum), reducing abundance of gammaproteobacteria such as Pseudomonas spp. and Escherichia/Shigella spp. and increasing bacterial richness and CD8+ T cell fraction in the terminal ileum. This could explain how VD3 interferes positively in the IBDs and other inflammatory disorders. 2,8,29 –36
The VDR is present in practically all immune cells (macrophages, dendritic cells, B cells, neutrophils, activated CD4+, and CD8+ T cells) and consequently it may influence modifications in the antimicrobial barrier of the mucosa of intestine, interfering in the gut barrier function, antigen presentation and response, and regulation of immune system. 29,35
VDR may also directly activate the nucleotide-binding oligomerization domain (NOD2) expression leading to the stimulation of NFκβ and production of the antimicrobial peptide named defensin β2 and cAMP (cyclic adenosine monophosphate) that are related to the codification of cathelicidin. This gut antimicrobial peptide is important in the mucosal immune barrier and its decrease may be a link to CD development. This mechanism mediated by VDR also leads to the downregulation in the release of proinflammatory cytokines (TNF-α, IL-1, IL-6, and IL-8) and influences the function of T lymphocytes and IFN-γ and improves the response mediated by TH2. Activated VD may result in the inhibition of dendritic cells and reduce the TGF-β1, fibroblasts, peripheral blood mononuclear cell, and lamina propria mononuclear cell, reducing the production of proinflammatory cytokines. Furthermore, VD is necessary for the production of regulatory cells such as Tregs and invariant natural killer T cells, leading to the disconnection among TH1 and TH17 cells resulting in the imbalance of the gastrointestinal tract (Fig. 5). 22,23,30,36 –38

Role of VD (1,25(OH)2D3) in the inflammatory process in IBD patients. The action of VD in Paneth cells results in activation of the NOD2 and release of cathelicidin and β-defensin. VD inhibits dendritic cells, fibroblasts (reducing TGF-β1, PBMC, and LPMC, and thus in the cytokines release. LPMC, lamina propria mononuclear cell; NOD2, nucleotide-binding oligomerization domain; PBMC, peripheral blood mononuclear cell; TGF-β, transforming growth factor-beta; VD, vitamin D. Modified from Ardesia et al. (2015). 35
The deficiency of this vitamin may reach 30–50% in the population worldwide, which could influence the increase in the incidence of IBDs. Several authors have shown that it may be related to higher disease activity in UC and CD patients with mild-to-moderate activity both in human and in animal models. The VDR is significantly higher in areas near genes known to be linked with autoimmune disease and cancer. This happens with PTPN2 that is a gene implicated in CD and UC once it plays an important role in the homeostasis of the epithelial barrier. The lower expression of these genes in patients with insufficient levels of VD may be because of the decreased VDR ligand. Alteration in VDR also decreases its effects in Paneth cells, resulting in reduction of the host defense because of the decrease in the effects of cathelicidin and defensing. 1 –5,30,35,38,39
The literature shows that IBD patients are normally VD deficient, mainly CD individuals. The use of this hormone may influence the IBD therapeutic approach because patients with higher levels of this vitamin exhibit better outcomes before starting anti-TNF-α than patients with lower levels. Blood levels are also related to the intensity of the symptoms. Furthermore, VD may help in the management of CD leading to the decrease in the activity index scores of the disease. In VD-deficient animal models, it is possible to see a greater bacterial translocation to extraintestinal tissues, and higher inflammatory cell infiltrates and higher release of inflammatory cytokines such as TNF-α, IL-1β, IL-6, TGF-β, IL-17A, and IL-17F. Thus, it is important to point that the precise VD levels for the management of IBDs are still controversial. 10,40 –43
The insufficiency of VD results in imbalance in the gastrointestinal tract with increase in the inflammation process and modification in the microbiota because of host injury. It may regulate the microbiota and thus interfere in the homeostasis of the gastrointestinal tract. For this reason, it may play many attributions in the prevention of IBDs and maintenance of remission. 1,29,37,40
Conclusion
Several studies have showed that the insufficiency of VA and VD may be related to IBDs. Vitamin supplementation could be helpful in the treatment and prevention of these inflammatory processes, but more studies are necessary to establish the precise needs of these compounds to obtain benefits regarding the prevention or maintenance of remission to the improvement of the quality of life.
Footnotes
Authors' Contributions
S.M.B., M.D.B., and K.Q. designed the study and wrote the final version of the article. R.A.G., R.G.G., A.C.A.C., and A.M.R.F. contributed to literature search, helped in writing, and corrected the final version of the article. All authors accept equal responsibility for the accuracy of the contents of this article.
Author Disclosure Statement
No competing financial interests exist.