
Abstract
This randomized crossover study compared the impact of virgin coconut oil (VCO) to safflower oil (SO) on body composition and cardiovascular risk factors. Twelve postmenopausal women (58.8 ± 3.7 year) consumed 30 mL VCO or SO for 28 days, with a 28-day washout. Anthropometrics included body weight and hip and waist circumference. Fat percent for total body, android and gynoid, fat mass, and lean mass were measured using dual-energy X-ray absorptiometry. Women maintained their typical diet recording 28 days of food records during the study. Results were analyzed with SPSS v24 with significance at P ≤ .05. Comparisons are reported as paired t-test since no intervention sequence effect was observed. VCO significantly raised total cholesterol, TC (+18.2 ± 22.8 mg/dL), low-density lipoprotein (+13.5 ± 16.0 mg/dL), and high-density lipoprotein, HDL (+6.6 ± 7.5 mg/dL). SO did not significantly change lipid values. TC and HDL were significantly different between test oils. The TC/HDL ratio change showed a neutral effect of both VCO and SO. One person had adverse reactions to VCO and increased inflammation. VCO decreased IL-1β for each person who had a detected sample. The impact of VCO and SO on other cytokines varied on an individual basis. This was the first study evaluating the impact of VCO on body composition in Caucasian postmenopausal women living in the United States. Results are suggestive that individuals wishing to use coconut oil in their diets can do so safely, but more studies need to be conducted with larger sample sizes, diverse populations, and more specific clinical markers such as particle size.
Introduction
C
Nevertheless, confusion about VCO continues because it is a highly saturated fat (93%) food. While researchers have suggested that saturated fat may not be detrimental for health, 12,13 the most recent 2015 Dietary Guidelines for Americans still suggest limiting saturated fats, including tropical oils. 14 VCO is a unique saturated fat because it is rich (65%) in short and medium chain fatty acids that metabolize rapidly without depositing in arteries and fat cells. 8,15,16 The most substantial medium-chain fatty acid, lauric acid, has antimicrobial, antifungal, and antiviral properties giving a unique benefit to VCO compared to other oils. 6,15 The question remains what impact the resulting 35% long-chained fats would have on health outcomes.
Although the evidence pointing to the benefits of VCO is increasing, few human studies exist exploring VCO's impact on measurable health outcomes. The most recent review on VCO and heart disease highlights the need for more studies. 17 Most studies that highlighted beneficial impacts of VCO were in vitro animal studies that used medium-chain triglycerides (MCTs) or were conducted in Pacific Islander/Asian populations. The human data in existence are not generalizable to most Western societies due to different diets, lifestyles, and genetic predispositions.
The purpose of this study was to compare the health impacts of VCO to “heart healthy” safflower oil (SO) in postmenopausal women living in the Rocky Mountain region of the United States. To our knowledge, this is the first study to examine VCO in an older U.S. population.
Materials and Methods
Study design and participants
This study was approved by the Institutional Review Board at the University of Colorado Colorado Springs. Fourteen women were recruited from the Colorado Springs community through fliers, email blasts, and word of mouth. Of these 14 women, 12 completed the study. One woman dropped out during the first month due to loss of the oils while travelling and the second dropped out due to enrollment in another study before the beginning of the first testing phase of this study.
Inclusion criteria included the following: (1) postmenopausal women between the age of 45–65, (2) not taking any hormone replacement therapy, (3) not taking medication or supplements that could alter lipids, (4) normal fasting lipid levels (total cholesterol [TC] <240 mg/dL at screening), and (5) willing to ingest two tablespoons of VCO and SO each day for two nonconsecutive 28-day periods.
This randomized, crossover clinical trial included two 28-day dietary supplementation interventions consisting of daily ingestion of either two tablespoons (30 mL) of VCO or SO distributed throughout the day. Testing was done in 1 day and women were selected into alternating oil intervention groups based on their arrival times. Participants were instructed to add oils to already-prepared foods as a topping, into smoothies, or to make dressings out of them. Participants were instructed not to cook with the oils to avoid chemical breakdown; however, upon evaluation of dietary records, participants did lightly sauté their food when using VCO. Each subject received 28 plastic containers with premeasured doses of the designated oil in each container. They were instructed to ingest one container per day throughout the supplementation period and return all containers (used and unused) at the next measurement period. Participants were instructed to continue their normal diet and exercise routine throughout both supplementation periods as well as the 30-day washout period to replicate normal living conditions.
Origin and composition of oil supplements
The intervention oils were Organic VCO (Tropical Traditions, Gold Label, West Bend, WI) and Organic High Heat SO (Spectrum; The Hain Celestial Group, Inc., Boulder, CO). The VCO was made in the Philippines from USDA certified organic coconuts using the traditional fermented method. Shredded coconut meat is added to water from inside the coconut to make coconut milk. After sitting for about 12 h, the oil naturally separates from the heavier water. The oil is heated for a short time and filtered from the curds. Each oil was measured by weight (1 oz/30 mL/2 Tbs) using an electronic kitchen scale (Salter Model 3001) and packaged in individual portions. Oil composition was tested at the UCCS Department of Chemistry laboratory.
Anthropometric evaluation
Measurements were collected before and after each supplementation period. Body mass was measured using a Tanita BF679W scale to the nearest 10th of a ounce. Height was measured using a stadiometer at commencement of the study. Body mass index was calculated by dividing the body mass (kg) by the square of the height (meters). Hip and waist circumference were measured with a standard tape measure to the nearest quarter of an inch and converted to centimeters. Waist was measured at the smallest circumference and hip at the widest circumference. Dual-energy X-ray absorptiometry (DXA) scans were completed at the beginning and conclusion of each testing period to determine percent body fat and distribution. Two participants declined to be measured by DXA.
Dietary evaluation
Upon commencement into the study, participants were shown how to complete a detailed food journal. Participants completed four food records during a 2-week wash-in period before starting the first intervention. During each intervention and the washout period, participants recorded all food consumed for eight assigned days per month (about 2 days each week) for a total of 28 food journals. Data were entered and analyzed using Food Processor Software (ESHA Research, Salem, OR).
Biochemical evaluation
Blood samples for the measurement of cytokines and cholesterol concentrations were collected before and after supplementation of VCO and SO. Blood was taken in the morning following a 12-h overnight fast.
Blood samples were collected in 4 mL ESTA and 7.5 mL serum separator tubes for cholesterol and cytokine evaluation, respectively. Samples were immediately spun in a centrifuge for 20 min, aliquoted, and frozen to −80°C. Cholesterol (high-density lipoprotein [HDL], low-density lipoprotein [LDL], triglycerides, and TC) was measured using a Beckman Coulter AU400 Chemistry analyzer. Inflammatory markers (TNF-α, IL-1β, IL-10, and IL-6) were measured using a high sensitivity multiplex kit by Randox. All biochemical data were processed at the Colorado Clinical and Translational Sciences Institute (CCTSI: Denver, CO; CCTSI is supported, in part, by Colorado CTSA Grant UL1 TR001082 from NIH/NCATS).
Statistical analysis
Data were analyzed using SPSS (Version 24; IBM, Armonk, New York) to determine normal distributions of continuous variables (visually and Shapiro–Wilk's test), descriptive statistics, and repeated-measures mixed model ANOVA using sequence of oil intervention as a covariate. The intervention sequence was not determined to be significant. Therefore, paired t-tests were conducted to determine difference before and after oil supplementation on the following: weight, waist circumference, hip circumference, total fat%, android fat%, gynoid fat%, android-to-gynoid ratio, fat mass, lean mass, and bloodwork. Differences from premeasures and postmeasures were calculated and paired t-tests were used to compare difference between oils. Significance was set to P ≤ .05.
Surveys
Before supplementation, all participants completed a medical history survey and a demographic survey. Upon completing each supplementation period, a short survey was completed regarding experiences with ingesting the oils.
Results
Twelve women successfully completed the study. One woman completed a total of about 2 weeks of the coconut protocol after suspicion that she was having an intolerance to the oil. Complaints included a scratchy throat and feelings of being unhealthy. After stopping the oil, her symptoms disappeared. She restarted the oils in the fourth week and symptoms returned. Upon closer inspection, all her inflammatory markers were elevated after coconut oil consumption markedly more than other subjects (Subject 1). One subject completed the coconut oil protocol for 3 weeks, due to a work-related trip. Other participants successfully used all oils as instructed. Excluding these two women from analyses did not change findings; however, they were excluded from group analyses to provide more reliable data.
The composition of the oils is presented in Table 1. As expected, VCO was rich in short- and medium-chain fatty acids, together comprising about 70% of the oil. SO normally has the highest linoleic acid content of any vegetable oil in the market. However, due to recent changes in the market, this type of oil is difficult to find. We used an oil that is typical of what is found on store shelves: high-oleic SO, which is hybridized to withstand high-heat cooking. This oil contained 80% oleic acid.
Samples were analyzed by GC/MS using a Hewlett Packard 6890 Series II Gas Chromatograph with 5973 Mass Selective Detector.
The energy and macronutrient contents of the diet are presented in Table 2. Since one of the purposes of the study was to test the feasibility of consuming 30 mL of oil, diet was not altered. An objective was to observe the impact of the oils in a way that people would normally consume the oils, within their own regular diets, and whether the oils impacted their dietary intake. Variations in consumption were due to illness and vacation. Results showed that women ingesting coconut oil ate 318 kcal more per day (P = .05) and had significantly more protein consumption.
Δ Change calculated as postintervention minus preintervention.
Statistically significant (P ≤ .05) between pre and post oil, paired t-test.
Statistically significant (P ≤ .05) between the change of VCO compared to SO, paired sample t-test.
Descriptive characteristics at baseline are presented in Table 3. Data not shown in the table include age and general lifestyle characteristics. Women on average were 57.8 ± 3.7 years old. There was a wide variation in exercise habits and intensity with women reporting about 229.1 ± 224.2 min per week of exercise (33% light activity, 42% moderate activity, and 25% intense activity). Women tended to be light drinkers consuming predominantly wine on an occasional to weekly basis (66%). Only one woman reported heavy drinking. Four women took daily medications (blood pressure and SSRI antidepressants). All women consumed dietary supplements. These consisted of vitamin/mineral supplements or bone support supplements such as glucosamine, chondroitin, or calcium.
BMI, body mass index; DXA, dual-energy X-ray absorptiometry; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Neither oil affected anthropometry significantly (Table 4). Although not statistically significant, the small increase in lean mass after VCO consumption and decrease after SO may be potentially clinically meaningful.
Δ Change calculated as postintervention minus preintervention, rounded to nearest 10th decimal. No statistical significance (P ≤ .05).
Table 5 shows results of lipid changes after oil interventions. Results show that VCO significantly raised TC, LDL, and HDL (P < .05), while decreased TG (P = NS). Conversely, SO decreased TC, LDL, and HDL and increased TG, but changes were not significant. The ratio of TC to HDL showed no changes to risk profile with either oil, while the TG/HDL showed a small improvement after VCO and small worsening after SO.
Δ Change calculated as postintervention minus preintervention.
Statistically significant (P ≤ .05) between pre and post oil, paired t-test.
Statistically significant (P ≤ .05) between the change of VCO compared to SO, paired sample t-test.
Figure 1 presents results of inflammatory markers IL-1β, TNF-α, and IL-6 as well as the anti-inflammatory marker IL-10. These markers were not detected in some samples. Due to the small numbers available, results are presented individually by subject number and only those results where we had markers detected are shown. Subject 1 (intolerant reaction to VCO) showed dramatically increased inflammation after coconut oil. IL-1β, aside from Subject 1, showed varying levels of decreased inflammation after coconut oil consumption in every subject. TNF-alpha and IL-6 showed variability of inflammation with some women showing decreased inflammation, while others showed increased inflammation on each oil. IL-10, an anti-inflammatory cytokine, revealed small, but mostly inconsequential, variability.
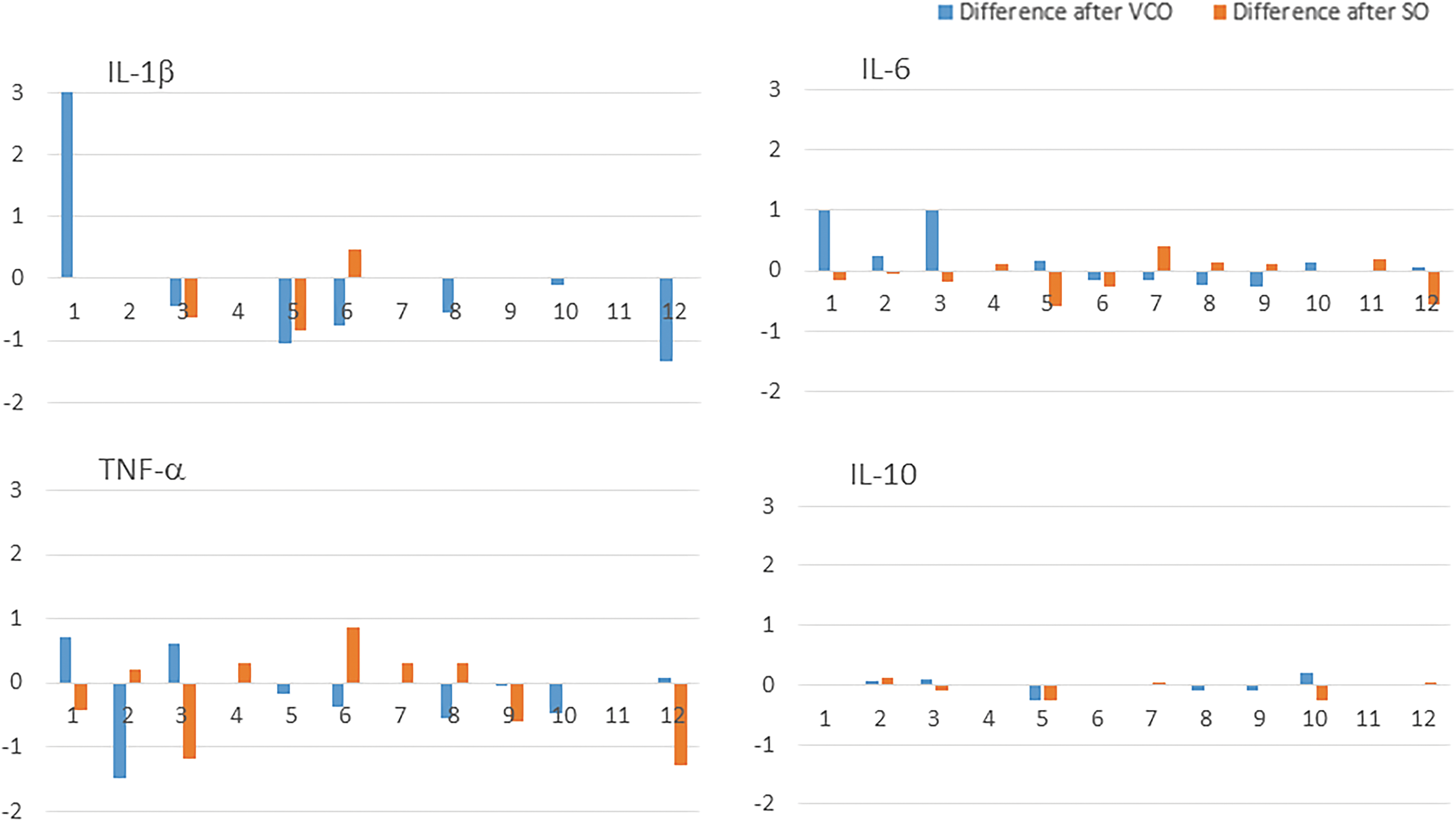
Differences in inflammatory markers after VCO and SO by subject. VCO, virgin coconut oil; SO, safflower oil.
Discussion
The results of this study show that VCO contributes negligible changes to body composition and the cardiovascular risk profile in Caucasian postmenopausal women living in the United States. Previous studies reported that VCO decreased waist circumference in both men and women. Many of these studies used MCT oil making the comparison irrelevant. 18,19 Of the studies using VCO as an intervention, VCO contributed to smaller waist circumferences and weight loss in three studies. 4,5,20 In this study, participants consumed an extra 318 kcal on average when consuming the VCO, offsetting any weight loss that may have occurred had caloric intake stayed the same in both oils. Despite reporting they felt “fuller” quicker with VCO, participants reported adding VCO to more smoothies with whey protein (replacement of breakfast drinks) and to meat-based dishes (predominantly eggs at breakfast and meat at dinner). When consuming SO, women tended to add the oil to salad dressings (at dinner) and oatmeal (at breakfast) due to ease of working with the flavor and textures of the oils. Although small and not statistically significant, VCO also slightly increased lean mass by +0.4%, while SO decreased lean mass by −0.3%. This may be clinically meaningful in the postmenopausal years, particularly if the addition of weight training regimen is added. In light of the excess calories consumed with no changes in body composition, combined with the well-known impact of VCO on faster energy expenditure, using VCO can potentially contribute to weight maintenance/loss efforts.
Animal models have suggested that using coconut oil as a fat source in the diet may increase lipolysis and decrease lipogenesis in the liver as well as other tissues. 21 –23 Mice fed coconut oil plus conjugated linoleic acid (CLA) experienced a more rapid onset of lipolysis and decreased lipogenesis compared to mice fed a soy oil/CLA combination. 22 Deol et al. reported that mice fed coconut oil instead of a soy/coconut oil combination had less adiposity, including less fat accumulation in the liver. 23 The increased oxidation of fatty acids and decreased lipogenesis may be mediated, in part, by coconut oil influencing the PPARα-dependent pathways. 21 However, to date, these findings have not been explored in humans.
VCO significantly raised TC, LDL, and HDL, while safflower decreased all lipids, but not significantly. The total/HDL and TG/HDL ratios have been suggested to be good predictors of cardiovascular risk in addition to individual lipid values. 24 –26 In this study, women had a relatively low risk of cardiovascular disease based on the Total/HDL ratio, which also remained unchanged in both oil interventions. More notably, TG's and TG/HDL ratio improved with VCO (bringing it down to optimal levels of 2.0 or less), but worsened with SO. Although LDL increased with VCO and decreased with SO, this value was offset by the increases and decreases in HDL with VCO and SO, respectively. Results on lipids have been mixed in other studies. While all human studies examined show significant increases in HDL (including in coronary artery disease patients), 4,5,7,20,27 only one study showed a neutral impact on LDL 5 and others showed an elevation. 4,7,20,27 While an elevated LDL may be concerning, numerous animal studies show that VCO lowers oxidation and inflammation, explained by the increases in antioxidant status. 28 –34 Several studies show that fat increases LDL particle size from small oxidizable phenotype B to a less atherogenic large phenotype A, although these diets were also lower in carbohydrates. 35 –37 The effect of diet on LDL alone is insufficient evidence for an increased cardiovascular risk. 38 There are no human studies conducted examining oxidation or particle size after VCO consumption. However, Voon et al. compared olive, palm, and VCO and found no differences in thrombogenicity and cell adhesion between the oils. 9 Other studies found lowered Lp(a) after VCO intervention. 27,39 Palazhy et al. found no difference in plaque concentrations between sunflower oil and VCO. 16 These findings suggest that labeling VCO as atherogenic may be premature.
This was the first study to examine inflammatory markers in a U.S. population on VCO. Of note, Subject #1, who displayed sensitivity to VCO, also had every cytokine increase, indicating inflammation. Of the VCO results, all participants showed a lowering, to various degrees, of IL-1β, a marker associated with neurodegenerative disease. To our knowledge, this is the first human American study to show IL-1β results after VCO ingestion. A study in healthy Malaysians indicated that VCO's impact on IL-1β was also lowered after VCO, in addition to other cytokines. 27 TNF-α and IL-6 are both master regulating cytokines for inflammation. Both were fairly well detectable by testing procedures, unlike IL10 (the anti-inflammatory cytokine). While some participants showed a decreased inflammation with VCO, others showed a small increase. In addition, the opposite effect was seen in each individual when consuming SO (if VCO lowered these cytokines, SO increased them and vice versa). Some possible explanations may include epigenetic and dietary factors. More research needs to be done to explore how diet quality in conjunction with VCO use may impact inflammation (since inflammation is an underlying cause of heart disease). Additive effects of other lifestyle choices such as sleep and exercise should also be explored against the use of VCO.
There were strengths and limitations of this study. One limitation was the small sample size; however, the sample was very homogenous, limited to postmenopausal Caucasian women. A highly motivated population, a high rate of compliance, randomization of the oils, and a crossover design were also strengths of the study. The fermented nature of VCO used contains the highest amounts of antioxidants compared to other methods of extraction. 3,40,41 Nonblinding, however, was a limitation. The texture and strong scent of VCO may have impacted how the oils were ingested, even though women were asked not to alter diets. Previous human studies using VCO also were unblinded and incorporated the oils into subjects’ regular diets. A blinded trial using VCO is difficult to conduct. To ingest 1 oz. of oil per day in supplement form, a total of about 47 capsules would be required per day, which is unfeasible for most people, especially for an extended amount of time (personal communication with Capsugel Company). It is possible to mask the oils in a beverage or food with the use of thickeners and coconut oil extract, but the feasibility would be very costly.
In summary, this study showed VCO had mostly neutral effects on cardiovascular disease and body composition, although more studies need to be performed, determining its effects on oxidation and particle size in relation to dietary factors. This was the first study done in a Caucasian U.S. population examining inflammatory markers. VCO may be anti-inflammatory for some people, but more research should be done exploring epigenetic, dietary, and lifestyle factors. We conclude that VCO is neutral and possibly beneficial for some people, when incorporated into everyday use. However, intolerance to VCO is possible and should be monitored individually.
Footnotes
Acknowledgments
This research was supported by The University of Colorado, Colorado Springs’ Committee on Creative and Research Works Seed Grant Program. We would like to thank Tropical Traditions for voluntarily donating the oils upon our inquiry for pricing before the study. We kindly thank CCSTI for the processing of our bloodwork (CCSTI is supported, in part, by Colorado CTSA Grant UL1 TR001082 from NIH/NCATS) and Dr. Janel Owens and Luis Lowe of the UCCS Chemistry Department for oil chemistry testing. We would also like to thank the graduate and undergraduate health promotion and nutrition students for their volunteer contributions in helping with the coordination and data entry activities throughout this study.
Author Disclosure Statement
No competing financial interests exist.