
Abstract
Stevia rebaudiana (SR) is often used by the food industry due to its steviol glycoside content, which is a suitable calorie-free sweetener. Further, both in vitro and in vivo studies indicate that these glycosides and the extracts from SR have pharmacological and therapeutic properties, including antioxidant, antimicrobial, antihypertensive, antidiabetic, and anticancer. This work reviews the antiobesity, antihyperglycemic, antihypertensive, and antihyperlipidemic effects of the majority of glycosides and aqueous/alcoholic extracts from the leaves, flowers, and roots of the SR. These compounds can serve as a natural and alternative treatment for diseases that are associated with metabolic syndrome, thus contributing to health promotion.
Introduction
M
Cardiovascular disease is the first cause of morbidity and mortality in Mexico, where endocrines diseases such as AO, DM, and AHT, along with an abnormal lipid metabolism, are risk factors for CVD. Moreover, CVD is currently among the first 10 causes of death worldwide. 3,4 Currently, there are several chemically synthesized pharmaceuticals for treating these diseases. However, many of them have secondary undesirable effects such as lactic acidosis, metallic taste, and vitamin B12 deficiency. Therefore, there is a demand for new natural-based medicinal compounds, 4,5 with Stevia rebaudiana (SR) Bertoni being a potential source for these compounds.
SR is native to the Amambay Mountains, which are located between southern Brazil and northern Paraguay. Guaraní Indians live there and since ancient times have consumed SR as a sweetener and a medicinal plant that they call ka'a he'ё or sweet herb. 6 The presence of steviol glycosides in SR is responsible for its sweet taste. These compounds are 200–300 times sweeter than saccharose-based candies and get advantage for not containing calories. 7 Besides containing natural sweeteners, SR has also a complex mixture of other compounds, including terpenes, tannins, sterols, volatile acids, vitamins, carotenes, flavonoids, enzymes, organic acids, polysaccharides, hormones, and microelements. 8 Further, interesting biofunctional properties have been found in phytochemicals that are present in SR, which encourages the study of its properties. Thus, this work aims at reviewing the antiobesity, antihyperglycemic, antihypertensive, and antihyperlipidemic effects of the majority glycosides and aqueous/alcoholic extracts from the leaves, flowers, and roots of SR. These glycosides and extracts can serve as a natural and alternative treatment for the diseases that are associated with metabolic syndrome.
Metabolic Syndrome
Metabolic syndrome is a set of risk factors that are characterized by the presence of AO, high arterial pressure (AP), and disorder in the carbohydrate and lipid metabolism. Under AO, the functionality of adipose tissues (AT) decreases, causing a misbalance of reactive oxygen species and proinflammatory cytokines such as tumor necrosis factor-α (TNF-α), interleukin 6 (IL-6), adiponectin, leptin, and plasminogen activator inhibitor (PAI1). This systematically triggers inflammatory processes that will eventually increase the risk of developing cardiovascular diseases (Fig. 1). 1,2,9 –11 Metabolic syndrome has other names, including IR syndrome, plurimetabolic syndrome, and deadly quartet. However, in 1998, the World Health Organization (WHO) proposed a unifying definition for the syndrome and decided to call it metabolic syndrome. 1,12,13

General mechanism of the development of metabolic syndrome. IL-6, interleukin-6; LDL, lipoprotein low density; ROS, reactive oxygen species; TNF-α, tumor necrosis factor-α; VLDL, very low-density lipoprotein.
Prevalence and diagnosis of metabolic syndrome
The prevalence of metabolic syndrome depends on some factors such as gender, age, and ethnicity and ranges between 15% and 40% of the total world population, being more latent in Hispanics. This syndrome is present in 22–34% of the U.S. population; whereas in Mexico, this percentage increased from 28% to 40% between 1994 and 2000 and was about 42% from 2006 to 2012, being more often in women than men according to the National Health and Nutrition Survey (NHNS). 11,14
As this condition is a syndrome and not a disease, relatively simple biochemical and anthropometric parameters are required for its diagnosis. Table 1 shows the diagnostic criteria for metabolic syndrome proposed by the WHO, the National Cholesterol Education Program–Expert Panel on Detection, Adult Treatment Panel III (NCEP-ATP III), and the International Diabetes Federation (IDF). 13,15,16
Abdominal circumference.
Refer to Ref. 9.
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; IDF, International Diabetes Federation; NCEP-ATP III, National Cholesterol Education Program–Expert Panel on Detection, Adult Treatment Panel III; WHO, World Health Organization.
The WHO considers IR as a needed component of metabolic syndrome, whereas the IDF considers AO as more relevant. 9 The NCEP-ATP III selected three out of five parameters that generated controversy. Also, highlighting five parameters only (and no more) is highly questionable. However, the NCEP-ATP III is also highly accepted and has a great clinical use due to the routine nature of its parameters that can be measured in a medical consulting room. Therefore, this review took the parameters stated by the NCEP-ATP III as a reference to determine the factors involved in metabolic syndrome (AO, fasting blood sugar level, dyslipidemia, hypertriglyceridemia, low high-density lipoprotein [HDL], and AP). 9
Abdominal obesity
Obesity is the accumulation of AT that increases the corporal weight. Adipocytes act as a dynamic tissue in response to nutritional adaptation and suffer a misbalance that is characterized by an increase in their capacity to expand. Therefore, the plasticity of the AT is a key factor for understanding obesity. 17 The existence of a dysfunctional metabolism in the organism, along with an increase in the size of the adipocytes in the waist and hip areas (i.e., AO), leads to a misbalance of the cytokines that decreases adiponectin and increases the release of leptin, IL-6, and TNF-α. This situation contributes significantly to the inflammatory state, IR, DM, dyslipidemia, arterial hypertension (AHT), and metabolic syndrome. 17 –19 Fat accumulation in the abdomen (android model) has increased during the past decades due to changes in lifestyle and diets. 14,20 –22
Genetic predisposition, diet, lifestyle, and environmental factors are some of the causes of AO. These factors favor energetic misbalance, inflammation, and the increase in AT. AO is currently a public health problem due to the alarming increase in the number of people with this disease. 23
Mexico holds the first place at the global level in overweight and obesity, with 71.3% of its adults (people older than 20 years) suffering these conditions, that is, 48.6 million people. The prevalence of AO in women and men is 82.8% and 64.5%, respectively. It is lower in people aged between 20 and 29 years (53.3%) than in adults who are 40+ years (80%). 14
Diabetes mellitus
Besides AO, DM (fasting blood sugar level higher than 100 mg/dL) also constitutes part of the set of diseases that are associated with metabolic syndrome. In fact, DM is currently the most relevant metabolic disorder as it affects almost all the organs of the body. This disease affects a high percentage of the productive population and therefore, the Health Sector considers it as a nosological problem that deserves priority attention. 24
DM is a set of biochemical, physiological, and anatomical abnormalities that are derived from a disturbance of glucose homeostasis and a deficiency in the secretion of insulin by beta-type cells in the pancreas. It is frequently associated with AO and other diseases that are associated with metabolic syndrome, triggering a set of difficulties in the long term that increase cardiovascular mortality and ischemic cardiomyopathy by three to four times. 25,26
DM can be classified into two groups: (1) The first (type 1 group) is frequently used to describe the appearance of the diabetes derived from the inability of the pancreas to produce enough insulin to catch all the glucose, and (2) the second (type 2 group) is mainly associated with IR. 27,28
Several researchers agree that the increase in abdominal fat and the deterioration of insulin signaling are the main responsible factors for type 2 diabetes. IR has been very related to the reduction in the metabolic capacity to return to its normal circulation, implying an abnormal biological answer to the body systems. This pathologic feature of the disease is a key factor of metabolic syndrome. 3 –5,29
In Mexico, about 10% of the population suffer from DM and it is estimated that 90% of these cases are of type 2 diabetes, which is more frequent in older adults and obese people. Thus, this disease has become the main mortality reason, with 12% of the total deaths. 30
Data provided by the NHNS (2012) identified 6.4 million Mexican adults suffering diabetes, that is, 9.2% of the adults in the country who have already been diagnosed with diabetes. The prevalence of diabetes in 40–49 year-old people increased by 50% from 2000 to 2012—not counting diabetic people who are not aware about their condition. 14
The WHO estimated that the number of people suffering diabetes worldwide in 1995 was 30 million and that this number increased up to 347 million in 2014. The same institution projected that 366 million people worldwide would suffer diabetes by 2030. 31,32
Arterial hypertension
AHT is a chronic and degenerative disease that is associated with metabolic syndrome and it is defined as a steady, high systemic AP. It is generally diagnosed by means of three separate measurements of elevated systolic and/or diastolic pressures (higher than 120 and 80 mmHg, respectively). The seventh report of the Joint National Committee for the Prevention, Detection, and Evaluation of AHT (JNC7) established new treatments for normal and prehypertension levels as well as two stages for AP (Table 2). 33,34
Refer to Ref. 34.
JNC7, Seventh Report of the Joint National Committee for the Prevention, Detection, and Evaluation of AHT.
The JNC7 recommends keeping an AHT lower than 140/90 mmHg for most of the patients and lower than 130/80 mmHg for patients suffering DM or renal disease. Currently, AHT affects about 26.4% of the adult population and 60–70% of the people in their 70s. This disease is very prevalent in Mexico as, according to the NHNS, about 31.5% of the population older than 20 years suffer this condition, being more frequent in obese adults (42.3%) and diabetic adults (65.6%). Further, more than 50% of men and 60% of women older than 50 years suffer AHT. The prevalence of AHT in Mexico increased from 19.7% to 31.5%, affecting one out of three adults. 32,35
Metabolic syndrome increases the harmful effects of the AHT on arteries by increasing their stiffness and intensifying any cardiovascular problem. Hence, the physiopathological association between metabolic syndrome and AHT leads to an increase in cardiovascular risks. 12
AHT is an extremely frequent co-mobility in diabetic people that affects 20–60% of the population suffering DM. The prevalence of hypertension in the diabetic population is 1.5–3 times higher than in nondiabetics, thus contributing to the development of chronic complications of the disease. Extensive epidemiological evidence indicates that diabetic people with hypertension have a significant increased risk of suffering cardiovascular diseases, renal insufficiency, and diabetic retinopathy. 34
Dyslipidemia (hypertriglyceridemia and cholesterolemia)
Dyslipidemias are considered an alteration in the lipid metabolism that is characterized by an excess of triglycerides, total cholesterol (hypercholesterolemia), both of them (hyperlipidemia), and/or a low content of HDL-cholesterol particles. These dyslipidemias are one of the factors of metabolic syndrome and emerge when the lipid metabolism gets affected by OA, DM, AHT, or others. The rise of visceral fat in the human body increases lipolysis speed, leading to a greater mobilization and an increase of the circulating free fatty acid levels. 36
Insulin regulates the abnormal lipolysis effect on AT and also the free fatty acid release. Thus, insulin inactivity leads, in general, to an increase in lipolysis with a negative effect on arteries. This generates a lot of complications, including endothelial dysfunction, inflammatory processes, stimulation of platelet aggregation, metalloproteinase expression, and thrombogenesis. 37,38
Genetics and environmental factors (diets rich in saturated fats and sedentarism) lead to an increase in the lipid content in blood. This triggers the accumulation of atheromatous plaques on the vascular endothelium, which are the prelude of organic consequences such as cardiovascular diseases and CVDs. In Mexico, the prevalence of dyslipidemia in women and men is 28.8% and 26.5%, respectively. 14
Treatment and prevention of metabolic syndrome
Currently, there are several medicaments available to treat the disruptions that are associated with metabolic syndrome. These are chemically synthetized drugs that will have, in the long term, secondary and undesired effects such as lactic acidosis, metallic taste, and vitamin B12 deficiency. 3,5,39 There is then a new demand of new products based on medicinal plants for the treatment of diseases that are associated with metabolic syndrome, with SR being a potential alternative. 40
SR Bertoni: An Alternative for the Prevention and Treatment of Metabolic Syndrome
The genre Stevia has at least 110 identified species, and SR is particularly popular due to its sweetening capacity that made it known as the Sweet Herb of Paraguay. 6 The fame of the SR has increased due to its absence of toxicity, and it is considered an edible plant worldwide. 7 SR is a herbaceous perennial plant that belongs to the Asteraceae family. It grows as a wild shrub reaching up to 65–80 height, has sessile leaves arranged oppositely, and is often asexually propagated (Fig. 2). 6

Stevia rebaudiana Bertoni. Perennial herbaceous plant belonging to the Asteraceae family, originating from the spontaneous flora in the semi-arid habitat of the mountainous slopes of Paraguay. Color images available online at
Phytochemicals of SR
Currently, SR is commercially cultivated to extract its sweeteners. However, it contains other compounds (including phytochemicals) that provide beneficial properties to health. 41 The compounds responsible for the sweetness of this plant were reported in 1931 when the French chemists, M. Bridel and R. Lavieille, isolated the steviol glycosides (Fig. 3) that provide its taste. These compounds were called stevioside and rebaudioside and are used by the food industry as sweeteners. 7 Stevioside and rebaudioside A (the sweetest compound) represent 5–10% and 2–4% w/w (dry basis) of the leaves. There are also other minority glycosides such as rebaudiosides B, rebaudiosides C, rebaudiosides D, rebaudiosides E, rebaudiosides F, dulcoside A, rubusoside, and steviolbioside. 42,43 Rebaudioside A is used by the food industry as a substitute for saccharose, whereas stevioside has therapeutic applications for the treatment of DM, obesity, caries prevention, and AP decrease. 44 –47
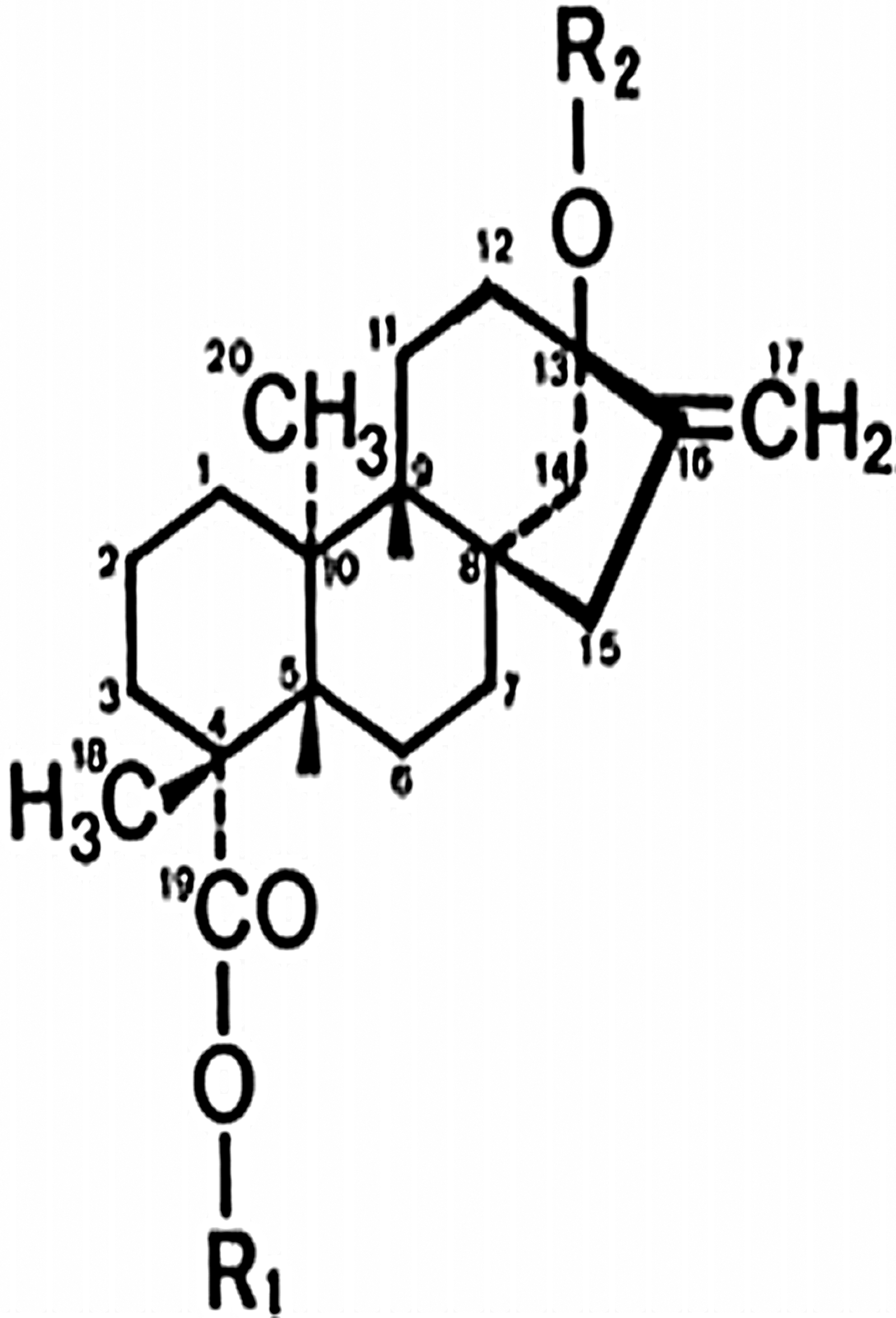
Chemical structure of the steviol molecule.
Besides steviol glycosides, SR has more than 100 phytochemicals and other compounds with antioxidant and medicinal properties. 48 The leaves have a complex mixture of compounds, including diterpenes, labdabos, triterpenes, stigmasterol, tannins, ascorbic acid, alkaloids, steroids, saponins, flavonoids, β-carotene, chromium, cobalt, magnesium, iron, potassium, phosphorus, riboflavin, thiamine, tin, zinc, apigenin, austroinilina, avicularin, β-sitosterol, caffeic acid, campesterol, caryophyllene, centaureidin, chlorogenic acid, chlorophyll, kaempferol, luteolin, and quercetin. 8
Biological effects of SR Bertoni
The extract from SR leaves is stable at 200°C, does not contain calories, does not ferment, does not generate dental plaque, is anti-caries, does not caramelize, and does not crystallize. Thus, the extract from SR leaves has multiple uses in several industries. 45,49 –54 SR has also several biological properties, including antacid, cardiotonic, anti-caries, anti-rotavirus, anti-bacterial, anti-hypertensive, anti-fungal, anti-inflammatory, anti-viral, anti-yeast, diuretic, antioxidants, hypotensive, antihyperlipidemic, and anticancer. Further, its antihyperlipidemic and insulinotropic effects contribute to the treatment of type 2 diabetes by stimulating the secretion of insulin by beta-type cells of the pancreas. 7,32,42,55 –57
SR and AO
Diets with a high glycemic index and high sugar consumption induce a set of metabolic complications, including IR, hyper insulin, DM, HTA, and AO. Therefore, substituting sugars with calorie-free sweeteners is an efficient strategy. 58 In the past years, SR glycosides have become attractive substitutes for sugar. They are intense calorie-free sweeteners that are helpful to control the ingestion of calories in diet, reduce weight, do not have adverse effects when consumed, and reduce AO (which is associated with a set of diseases, including abnormal metabolism of lipids, hypertension, DM 2, and others). 46,58,59 A study found that satiety levels of SR, aspartame, and saccharose were similar among each other. However, SR reduced the glucose and postprandial insulin levels. 58 Nowadays, SR glycosides are used by diverse countries to sweeten local tea, medicines, food, and diet drinks. 60
Diterpene glycosides are degraded to steviol by the intestinal flora of diverse animal species, including humans, which explains their benefits. Steviol is a molecule containing a hydrophobic ring and a negative charge in the carboxylic group. Unlike steviol, glycosides have a very limited absorption due to the monolayers of the Caco-2 cells. 28,61,62
Glycosides produce a maximum plasmatic concentration of 0.2 nM of steviol. It is completely absorbed by the large intestine and excreted by renal and biliary systems. After oral ingestion of glycosides, steviol is the main metabolite found in blood circulation and therefore, its metabolism in the liver has received special attention. 42,63 Substituting sugars with non-nutritive sweeteners, such as steviol glycosides, can lead to a loss of 380 cal/day or 1 lb of body weight in 9–10 days. 61 Table 3 summarizes some studies regarding the effects of the SR extracts on body-weight loss. Orally administered rebaudiodise A reduced the body weight, biliary acids, and serum cholesterol of rats. 64 Healthy patients achieved a maximum plasma concentration after 8 or 12 h of being administered (via the oral route) with rebaudiodise A, and most of the steviol (62% of the dose) was found as conjugated glucuronides. This indicated that, besides Phase I of metabolism, steviol also goes through Phase II, and most of the steviol is conjugated as glucuronide before being eliminated in the urine. 65 Isosteviol (compound of the metabolism of stevioside) improved the lipid profile and regulated the expression of beta-type cells by including regulating factors for insulin transcription, reducing the triglyceride content in plasma, and favoring body-weight loss in diabetic mice. 66 Extracts from SR, administrated via the oral route, showed a body-weight reduction in diabetic rats. 5
SR, Stevia rebaudiana.
SR Bertoni and DM
Diterpene glycosides in SR extracts act as an intense and a calorie-free sweetener and, if they reduce the sugar levels, they will have hypoglycemiant effects. On the other hand, if they avoid the rise of the glucose level induced by some agent (such as adrenaline, glucagon, alloxan, and glucose charge), they will have antihyperglycemic effects. 28 Some studies indicate that SR can help to reduce blood glucose levels in diverse animal models such as healthy mice, diabetic mice, alloxan or streptozotocin-induced mice, or mice supplied with aqueous or alcoholic extracts from SR in an acute or chronic way during 10–48 days (Table 4). Orally administered SR extract showed an antihyperglycemic effect, 67 a decrease of the blood glucose levels in diabetic rats under a time-dependent effect, 68,69 and a reduction of the hepatic gluconeogenesis of diabetes-induced mice. 70,71 SR also improved the glucose tolerance activity, 72 and the powder of its leaves had a hypoglycemic effect on diabetic rats. 73 The induction of the genes involved in glycolysis may be responsible for the increase in insulin secretion caused by the consumption of the stevioside and the suppression of glucagon in α-type cells of the pancreas. 63,74 Moreover, this glycoside reduces the blood glucose level as it modulates and inhibits the enzymes that metabolize glucose in the small intestine and it propitiates a better use of the glucose by periphery tissues and muscles of diabetic rats. 63,74 –76 In a study, steviosides (20 mg/kg body weight) were administered to 12 people suffering DM 2, resulting in a decrease in the plasmatic glucose concentration by decreasing the activity of the pyruvate carboxylase and the phosphoenolpyruvate carboxikinase (PEPCK). This also reduced postprandial glucose levels in the blood by about 18%. 63 Some studies indicate that the SR-based treatment on healthy volunteers increased their glucose tolerance and reduced their concentrations of plasmatic and postprandial glucoses. 40,77
GK, Goto-Kakizaki.
SR Bertoni and AHT
Diverse studies on animal models and hypertensive patients report that SR extracts and pure isolated stevioside have a relevant effect on the cardiovascular system (Table 5). In an experimental model, extracts from SR leaves were orally administered to healthy rats in a chronicle way. Results indicated a vasodilating action, diuresis, and natriuresis 60 days later. 78 The infusion of isolated steviol may affect the water transport through renal tubules, leading to a decrease in the blood that circulates in the cardiovascular system caused by increasing the amount of urine and sodium excreted by the body. 79 The increase of the stevioside-induced plasmatic renal flow reduces the vascular resistance and is associated with the vasodilatation of the vessels of afferent and efferent arterioles by means of the inhibition and influx of intracellular calcium and the release of a vasodilator prostaglandin. 79 A study indicates that a 200 mg/kg dose of isolated stevioside could effectively reduce the AP of spontaneously hypertensive (SHR) male rats without affecting their heart rate or their serum catecholamines levels. 33 Diabetic Goto-Kakizaki rats were administered with a chronic dose of 0.025 g/kg of stevioside during 6 weeks, and their AP was reduced during that period. 74 Oral and chronic treatment (2 years) with steviosides (500 mg) on hypertensive patients reduced their AP compared with placebos, and also the systolic and diastolic APs from 150 to 140 mmHg and from 95 to 89 mmHg, respectively. 80
AP, arterial pressure; SHR, spontaneously hypertensive; M, Mol.
In another study, 250 mg of steviosides was administered in hypertensive patients during 1 year. Results indicate that their systolic and diastolic APs decreased after 3 months of starting the treatment without any negative effect on the biochemical parameters. 81 The stevioside, administered via the intraperitoneal route in SHR rats, had an antihypertensive effect that caused vasodilation by inhibiting the Ca2+ flow in blood vessels. 82 Other in vitro studies concluded that the isosteviol, derived from the stevioside, inhibited Angiotensin-II and cell proliferation in the smooth muscle of rats. Isosteviol also reduced the vasopressin-induced contraction in isolated aortic rings by means of opening the KATP and SKCa channels. 83,85
SR Bertoni and dyslipidemia
Table 6 summarizes some studies regarding the antihyperlipidemic effect of SR. Alloxan-induced diabetic animals were administered, via the oral route, with aqueous and alcoholic extracts from SR under a chronic dose for 21 days, 70 and under an acute dose of 150 mg/kg. 72 Both treatments had a significant antihyperlipidemic effect. An oral and chronic treatment consisting of titanium oxide-based nanomatrices and SR extracts significantly decreased cholesterol and triglycerides. 86 Studies on humans indicate that the consumption of SR extracts increased the level of HDL and reduced the levels of cholesterol, triglycerides, and low-density lipoproteins significantly. 87
Conclusions
Studies on SR demonstrate that, besides being suitable as a sweetener, the aqueous and alcoholic extracts of this plant, as well as its steviol, are also a pharmacological alternative. In other words, these compounds have the required therapeutic potential for naturally treating endocrine diseases (such as obesity, diabetes, hypertension, and dyslipidemia) that are relevant in the current context. These diseases are associated with metabolic syndrome, which is considered a public health problem due to its current prevalence. Besides steviol glycosides, SR contains several phytochemicals, including phenols and flavonoids. More research is needed to determine their effects on the already known SR-based treatments, as well as their diverse mechanisms of action.
Footnotes
Author Disclosure Statement
No competing financial interests exist.