
Abstract
Hyaluronan (HA) has been utilized as a supplement. However, the absorption of orally administrated HA remains controversial. The degradation and absorption of HA in the intestine were investigated in this study. HA excretion into the feces, degradation in the intestinal tract, absorption through the large intestine, and translocation to the blood and skin were examined. HA administered orally was not detected in rat feces. HA was degraded by cecal content, but not by artificial gastric juice and intestinal juice. Oligosaccharide HA passed through excised large intestine sacs. Furthermore, disaccharides, tetrasaccharides, and polysaccharides HA were distributed to the skin of rats following oral administration of high molecular weight HA (300 kDa). The results of the study suggest that orally administered HA is degraded to oligosaccharides by intestinal bacteria, and oligosaccharide HA is absorbed in the large intestine and is subsequently distributed throughout the tissues, including the skin.
Introduction
H
HA is produced by hyaluronan synthases (HAS), which include three isoforms in vertebrates (HAS1, HAS2, and HAS3). 9 HAS1 and HAS2 produce high MW (>1000 kDa) HA, and HAS3 produces relatively low MW HA (∼300 kDa). 10 Some bacteria, including Streptococcus spp., also produce HA. 11
HA of animal and bacterial origin have various uses, including the production of medicines and cosmetics. HA has also been utilized as supplements for osteoarthritis pain management 12 –16 and maintaining skin moisture. 17 –21 The underlying mechanism of HA to improve osteoarthritis involves anti-inflammatory properties by the binding of HA to Toll-like receptor-4. 22 Skin moisturizing properties of HA have been proposed since increased production of HA aids in the recovery of skin barrier. 23,24
There is currently no consensus on the absorptive properties of HA, as one report claimed that HA was absorbed and distributed to the skin and joints, 25 while a second indicated that HA was not absorbed at all. 26 Because HA is naturally produced in the body, a radioisotope was used to estimate the absorption of orally ingested HA. HA was not measured directly in previous reports; therefore, there is a possibility that the absorption of HA was not reflected correctly.
To reveal the absorptive capabilities of HA, the degradation and absorption of HA in the gastrointestinal tract and the translocation of HA to tissue were examined in this study.
Materials and Methods
HA of different MWs (300 and 2 kDa; Kewpie Corporation, Tokyo, Japan) were used for the following experiments. All animal experiments were performed in accordance with the guidelines for the care and use of laboratory animals established by the Japanese Ministry of the Environment and were approved by Kewpie Corporation Ethics Committee of the Care and Use of Laboratory Animals.
HA excretion into feces
Twenty-four 5-week-old male Sprague–Dawley (SD) rats were purchased from Japan SLC (Shizuoka, Japan) and were acclimated to a temperature of 23°C ± 2°C and humidity of 50% ± 10% in a controlled room under a 12-h light/12-h dark cycle for 7 days. The rats were fed standard rodent chow (LabDiet® 5002; PMI Nutrition International, LLC, St. Louis, MO, USA) and provided water ad libitum during the acclimation period.
The animals were divided into three groups with equivalent body weights and HA groups were orally administered 1% and 5% HA (MW 300 kDa; 5 mL/kg body weight/day) for 5 days. Distilled water (DW) was orally administered to rats in the control group. Feces for last 3 days were collected, freeze-dried, and ground in a crucible for analysis. HA concentration in the ground feces was measured using the Hyaluronan Assay Kit (Seikagaku Corporation, Tokyo, Japan) with a HA binding protein (HABP). We used the Hyaluronan Assay Kit, because it excels in the quantitative capability and detection sensitivity. D-glucuronic acid concentration in feces was measured using a carbazole-sulfuric acid assay. 27 The detection limit of each assay is 12.5 ng/mL and 10 μg/mL, respectively.
Degradation of HA in the stomach and small and large intestines
Artificial gastric juices were adjusted as follows. Sodium chloride (2 g) was dissolved in 7 mL of hydrochloric acid and DW. Pepsin (activity 1:10,000; Wako Pure Chemical Industries, Ltd., Osaka, Japan) was added at a concentration of 0.1%, and DW was added to adjust the volume to 1 L (pH 1.2). One milliliter of HA solution (MW 300 kDa; 2.5%) or DW was added to 24 mL of artificial gastric juice, which was then incubated at 37°C for 2 h. Sodium hydroxide (1 M) was added to neutralize the solution.
Artificial intestinal juices were adjusted by mixing 250 mL of disodium hydrogen orthophosphate (0.2 M) with 118 mL of sodium hydroxide (0.2 M) and pancreatin (Wako Pure Chemical Industries, Ltd.) to a concentration of 0.1%, and DW was added to adjust the volume to 1 L (pH 6.8). One milliliter of HA solution (MW 300 kDa; 2.5%) or DW was added to 24 mL of artificial intestinal juices, which were then incubated at 37°C for 8 h.
Three 5-week-old male SD rats were used to examine the reaction of cecal content with HA. Briefly, the cecal content of rats was collected, weighed (average weight, 3.2 g), and mixed with an equal weight of water. One milliliter of 1.25% HA solution was added to 1.6 g of cecal content solution, and the mixture was incubated at 37°C for 24 h. One milliliter of water was added to the cecal content solution as a control. The supernatant was collected from the reaction solution by centrifugation (1500 g; 4°C; 15 min).
HA was analyzed by high-performance liquid chromatography (HPLC) using a Waters 2690 separation module (Waters Corporation, Milford, MA, USA). HA was separated on a YMC-Pack Diol-200 300 × 80 mm column (YMC, Kyoto, Japan) for the artificial gastric juice study or a YMC-Pack Diol-120 300 × 80 mm column for the artificial intestinal juice study and the cecal content study. The mobile phase was 0.003 M phosphate-buffered solution with 0.5 M sodium chloride for all analyses. HA was detected using a refractive index detector (Waters 996; Waters Corporation) at 210 nm.
Absorption of HA in the large intestine
After overnight fasting, the cecum, colon, and rectum from 6-week-old male SD rats were excised, filled with Tyrode's solution (137 mM NaCl, 3 mM KCl, 2 mM CaCl2, 2 mM MgCl2, 0.4 mM NaHCO3, 12 mM NaH2PO4, and 5 mM glucose; pH 7.4) or 5% oligosaccharide HA solution (cecum, 5 mL; colon and rectum, 0.5 mL) and closed tightly at each end. Each intestinal sac was then incubated in Tyrode's solution (cecum, 20 mL; colon and rectum, 10 mL) at 37°C with oxygenation for 2 h. Half of the medium was removed after 1 h and replaced with fresh medium. HA in the medium (after 1 and 2 h) was analyzed by HPLC (YMC-Pack Diol-120 300 × 80 mm; YMC). The detection limit of the HPLC assay was 10 μg/mL.
Translocation of HA to the blood and distribution to the skin
After overnight fasting, HA (MW 300 kDa) was orally administered to 6-week-old male SD rats (200 mg/kg body weight). Samples of cecal content, blood, and shaved ventral skin were collected from rats at 0, 2, 4, 6, and 8 h after HA administration. The cecal content was added to an equal volume of 0.003 M phosphate-buffered solution with 0.5 M sodium chloride, and the mixture was centrifuged at 1500 g for 20 min. HA in the supernatant of the mixture was analyzed by HPLC (YMC-Pack Diol-120 300 × 80 nm; YMC). Collected blood was centrifuged at 1500 g for 20 min to separate the serum. The collected skin was homogenized with DW, and the mixture was centrifuged at 1500 g for 20 min. Unsaturated HA disaccharides (u-HA2) and tetrasaccharides (u-HA4) in the serum and the supernatant of homogenized skin were analyzed by liquid chromatography–tandem mass spectrometry (LC/MS/MS) under the conditions shown in Table 1. The detection limit of LC/MS/MS is 1 ng/mL (u-HA2) and 10 ng/mL (u-HA4).
MS, mass spectrometry.
Statistical analyses
One-way analysis of variance with the Tukey post hoc test was used to determine significance. All statistical analyses were performed using the Dr. SPSS II for Windows software (SPSS, Inc., Tokyo, Japan).
Results
HA excretion into feces
HA concentrations in feces were below the detection limit (10 μg/3 days) in all groups (Table 2). Therefore, when HA was ingested orally (0.1% HA group, 2270 ± 47 μg/3 days; 0.5% HA group, 11,300 ± 19 μg/3 days), HA, which can be combined with HABP, was not excreted into feces. To analyze the excretion of low MW HA (less than decasaccharide), which cannot be combined with HABP, 28 D-glucuronic acid in feces was measured (Table 2). The amount of D-glucuronic acid in feces from the control group, the 0.1% HA group (intake amount, 1.0 ± 0.0 μg/3 days), and the 0.5% HA group (intake amount, 5.19 ± 0.09 μg/3 days) was 30.2 ± 3.0 μg/3 days, 31.0 ± 2.2 μg/3 days, and 30.6 ± 2.5 μg/3 days, respectively (corresponding intake of D-glucuronic acid = 0.4674 × HA intake).
Values are mean ± standard error, n = 8.
HA content in feces (the detection limit is 10 μg/3 days).
D-glucuronic acid content in feces (the detection limit is 1 mg/3 days).
HA, hyaluronan.
Since the amount of D-glucuronic acid in the control group was high, these results suggested that the amounts of D-glucuronic acid do not reflect the excretion of orally administered HA in feces.
Degradation of HA in the stomach and small and large intestines
HA degradation in artificial gastric juices, artificial intestinal juices, and cecal content by digestive enzymes was examined. The retention period of HA in a rat is about 2 h in the stomach, about 4 h in the small intestine, and about 24 h in the cecum. 25,29 Thus, HA was reacted with the respective enzymes for the respective retention period. The results showed that HA was not degraded by artificial gastric juices or artificial intestinal juices (Fig. 1A, B, respectively). In contrast, HA was degraded into oligosaccharides, principally disaccharides, in the cecal content (Fig. 1C).
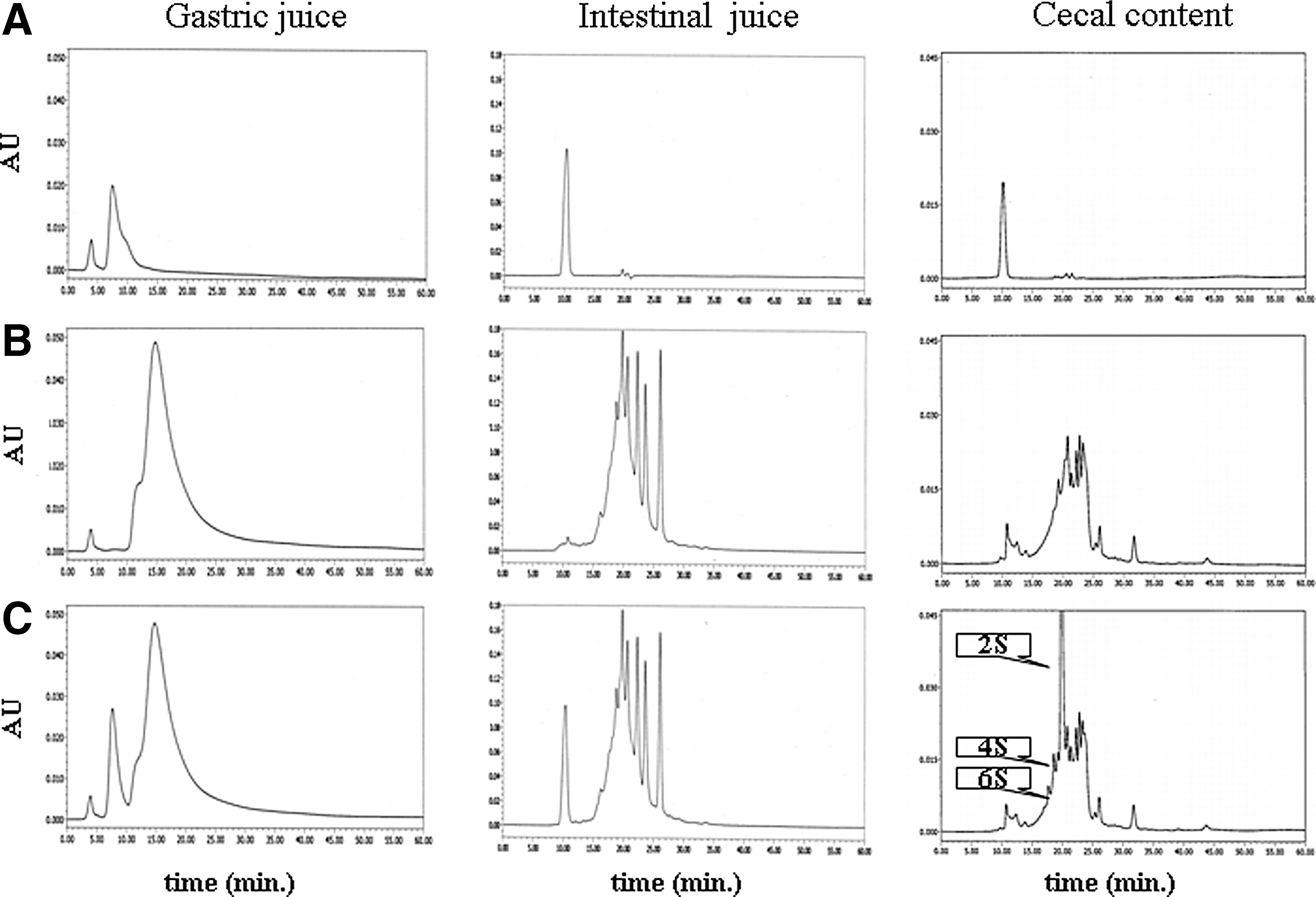
The HPLC profiles of decomposed HA by artificial gastric juices, artificial intestinal juices, or cecal content.
Absorption of HA in the large intestine
The permeability of oligosaccharide HA (MW 2 kDa) into the large intestine is shown in Figure 2. The HA with a MW lesser compared with a decasaccharide had permeated each region of the large intestine and the permeated amount increased with the passage of time. In particular, HA with a MW lesser compared with a hexasaccharide could permeate easily. Comparisons of different regions of the large intestine could not be made because of the different lengths of the organ and the enclosed solution volume. However, it was possible that HA was absorbed in every region of the large intestine.

The concentration of oligosaccharide HA in medium, in which excised large intestine, including oligosaccharide HA, was incubated for 1 and 2 h. The detection limit is 10 μg/mL. Values are mean ± standard error. n = 4.
Translocation of HA to the blood and skin
The results of cecal content analysis are shown in Figure 3. Oligosaccharide (di, tetra, hexa, octa, and decasaccharides) HA was observed in cecal content after 2 h of HA (MW 300 kDa) administration. After 4, 6, and 8 h of HA administration, similar results were obtained (data not shown).
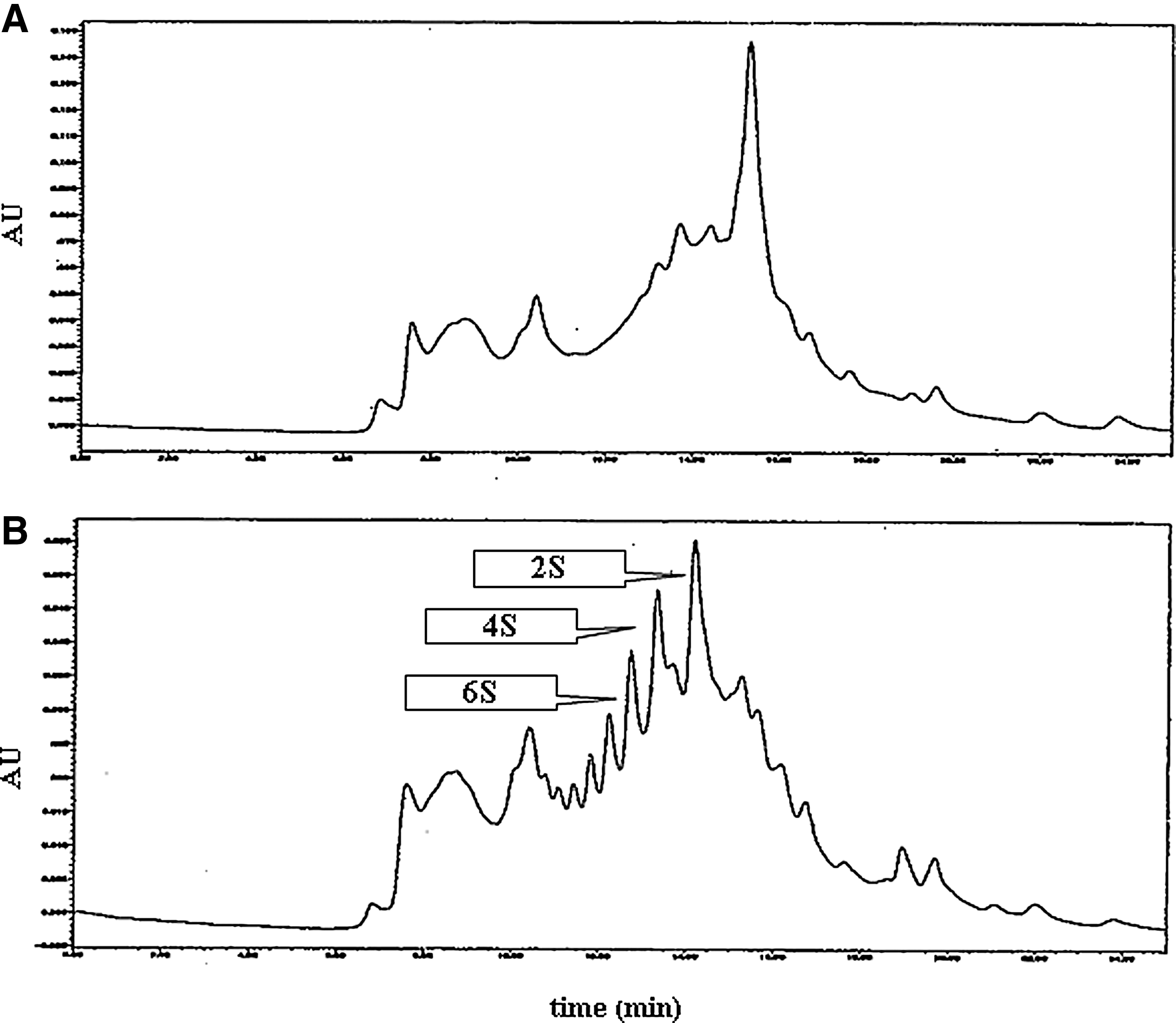
The HPLC profiles of cecal content of control rat
The results of u-HA2 and u-HA4 analysis (LC/MS/MS) are shown in Figures 4 and 5. The recovery rate of u-HA in the serum and skin was about 25% and 70%, respectively. The concentration of u-HA in the serum and skin increased with the passage of time, with the exception of u-HA4 in the serum. u-HA2 was observed in the serum 2 h after HA administration. u-HA2 concentration peaked in the serum after 6 or 8 h of HA administration (Fig. 4). u-HA4 in the serum was not observed until 8 h later (Fig. 5). u-HA2 and u-HA4 were observed in the skin 6 h after HA administration and peaked at 8 h (Figs. 4 and 5).
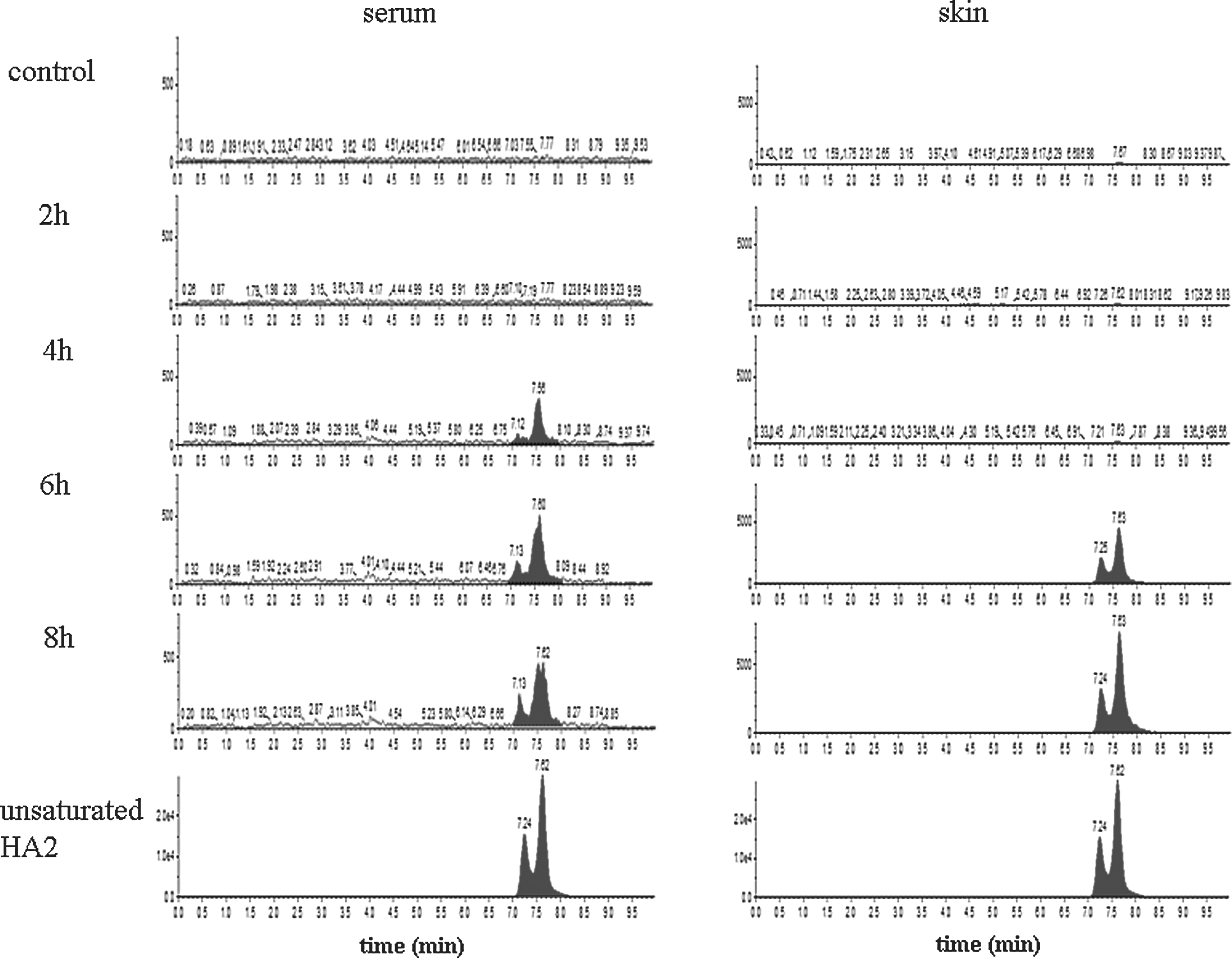
The LC-MS/MS profiles of unsaturated HA2 in serum or skin of rat, which was administered HA (MW 300 kDa). The detection limit is 1 ng/mL. LC-MS/MS, liquid chromatography–tandem mass spectrometry; MW, molecular weight.

The LC-MS/MS profiles of unsaturated HA4 in serum or skin of rat, which was administered HA (MW 300 kDa). The detection limit is 10 ng/mL.
Discussions
Chondroitin sulfate, which is also a glycosaminoglycan-like HA, was degraded into oligosaccharides by bacteria in the large intestine and eventually absorbed. 30,31 However, the absorption of HA remains controversial because it is difficult to estimate the absorption of orally administered HA as HA is distributed throughout the entire body. 3 Therefore, more recent absorption studies of HA have incorporated the use of radioisotopes. 25,26,29 The results of these studies showed that HA (1 MDa) labeled with 99technetium (99Tc), orally administered to rats and dogs, was distributed throughout the blood, skin, and joints. 25 Conversely, a second study reported that HA (1 MDa) labeled with 99Tc and 14 carbon ( 14 C) orally administered to rats was not distributed in the body at all. 26 Although the reason for these discrepancies remains unclear, the MW and the physical properties may have changed because of labeling with radioisotopes, which consequently influenced HA absorption. In a study that estimated the absorption of high MW HA (900 kDa) from chicken comb cells labeled with 14 C, over 80% of administered HA was absorbed and distributed into the skin and joints. 29
In this study, HA excretion into the feces, degradation in the intestinal tract, absorption through the large intestine, and translocation to the blood and skin were examined to determine if HA is actually absorbed.
First, HA excretion into feces was estimated. The retention period of food in a rat is about 2 h in the stomach, about 4 h in the small intestine, and about 24 h in the large intestine. 25,29 Therefore, the portion that is not absorbed should be excreted into the feces within 3 days. In this study, HA was administered orally to rats for 5 days, and the amount of HA in the feces during the final 3 days was measured. As a result, no excretion of HA into feces was detected by analysis using HABP (Table 2). Hence, HA with a MW lesser compared with decasaccharides cannot be detected in the feces, because the binding of low MW HA to HABP is weak. 28 Thus, the amount of D-glucuronic acid in feces was measured, but the results were unclear because of high background pollution (Table 2). Nonetheless, it became clear that HA with a MW greater compared with a decasaccharide was not excreted into the feces.
Second, HA degradation by digestive enzymes or intestinal bacteria was examined, which showed that HA was not degraded by artificial gastric juices or artificial intestinal juices, while HA was degraded into oligosaccharides by cecal content (Fig. 1). Similar results were obtained in the oral HA experiment (Fig. 3). It was reported that bacteria degrade glycosaminoglycan in the intestinal tract of humans. 32 Therefore, it is supposed that HA is degraded by intestinal bacteria in humans too.
In the experiment using excised large intestine, oligosaccharide HA, especially HA2, HA4, and HA6, had permeated the intestinal tract wall of the cecum, colon, and rectum (Fig. 2). Water and short-chain fatty acids are absorbed in the large intestine, and it was also reported that the carbohydrate inulin (5 kDa) is absorbed in the colon. 33 Thus, it is reasonable that the oligosaccharide HA (MW >2 kDa) is absorbed through the large intestine. Hisada et al. 34 reported that 50-kDa HA permeates through Caco-2 cell monolayers, in accordance with the results of the present study. In this report, passive diffusion through paracellular pathways was responsible for the absorption of HA with a MW of less than 5 kDa. LC/MS/MS analysis revealed that unsaturated HA2 and HA4 were detected in the skin of rats (Figs. 4 and 5). HA is degraded to unsaturated polysaccharides by hyaluronidase of intestinal bacteria, while mammalian hyaluronidase degrades HA to saturated polysaccharides. 35,36 For this reason, the detection of unsaturated HA in the blood and skin suggests that HA was absorbed in the large intestine. It became clear that u-HA2 and u-HA4 could be absorbed and were distributed to the skin. However, HA with a MW greater compared with hexasaccharides could not be analyzed by LC/MS/MS.
HA2, but not HA4, was detected in serum (Figs. 4 and 5). HA is reportedly absorbed and metabolized by the lymphatic system, 37,38 suggesting that HA with a MW greater compared with a tetrasaccharide is absorbed through the lymph.
There are two types of human hyaluronidase as follows: hyaluronidase 2, which degrades HA into 20-kDa subunits, and hyaluronidase 1 in the blood degrades HA into tetrasaccharides. 39 –43 Tetrasaccharide HA is degraded into monosaccharide by glucosidase in the liver and is utilized as an energy source and then finally expired as CO2. 29 These findings suggest the possibility that the oligosaccharide HA, which is distributed throughout the tissues, is metabolized in a similar manner.
There are many reports on the biological functions of oligosaccharide HA. 24,44 –47 For example, Kage et al. reported that HA4 improved recovery of skin function after UVA irradiation 24 and may induce epidermal differentiation through phosphorylation of CD44. 47
An in vitro study reported that low MW HA activated the immune response, including inflammation. 48 In a human study, oral intake of HA improved the knee joint pain 12,13 without promotion of inflammation. Together, these findings suggest the possibility that the reactions of HA differ in vivo and in vitro, particularly when HA is administered orally.
The results of the present study suggest that orally administered HA is degraded to oligosaccharides by bacteria in the cecum, and oligosaccharide HA migrates to the skin through the blood or lymph. It is expected that the absorbed oligosaccharide HA participates in the various effects of orally administered HA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.