
Abstract
β-glucosylceramide (GC) is a naturally occurring glycosphingolipid that was shown to improve hepatic steatosis, steatohepatitis, and insulin resistance in animal models of nonalcoholic fatty liver disease. In this study, we evaluated the safety and efficacy of oral administration of GC in subjects with nonalcoholic steatohepatitis (NASH). Twenty-three patients with biopsy proven NASH were enrolled in a double-blind, placebo-controlled trial. Patients were orally administered daily with 7.5 mg of GC. Patients were followed for safety, liver enzymes, HbA1c, insulin sensitivity, lipid profile, hepatic fat content as measured by magnetic resonance imaging (MRI), and NASH score on liver biopsy. No treatment-related adverse events were observed during treatment. In a per protocol analysis of data, oral administration of GC decreased the hepatic fat content as measured by MRI in GC-treated compared with placebo. HbA1C decreased in patients treated with GC. GC treatment was associated with a milder decrease in the high-density lipoprotein serum levels. The beneficial effects were associated with a decrease in CD4 and NKT cell subsets of lymphocytes. Due to the small number of subjects enrolled, differences did reach statistical significance. Oral administration of GC is safe and biologically active in patients with NASH and insulin resistance.
Introduction
N
Chronic inflammation underlines the mechanism of the metabolic syndrome, NASH and type-2 diabetes mellitus. 9 –12 Dysregulated inflammatory processes manifested by visceral inflammation in the liver and adipose tissue result in insulin resistance and liver damage. 13,14 Insulin resistance, oxidative stress, mitochondrial dysfunction, immune deregulation, and adipokines seem to be crucial in the pathogenesis of NAFLD. 6 In the process of inflammation, macrophages and endothelium contribute to increased serum levels of cytokines and adipokines, including C-reactive protein (CRP) IL-1β, IL-6, and TNF. 15 –17 Adipose stores play a dynamic role in the regulation of inflammation and innate immunity via modulation of the TLR/NF-kappaB regulatory pathway. 18
Recent studies suggest a change in sphingosine metabolism in patients with NASH. Using global metabolomic profiling, elevated levels of sphingosine were noted. 19 Palmitate-induced steatotic cells displayed elevated levels of diacylglycerols and monoacylglycerols. The metabolomics approach reveals biochemical changes in pathways important in the transition to hepatic steatosis, including insulin resistance, altered mitochondrial metabolism, and oxidative stress. 19 Liquid chromatography tandem mass spectrometry and gene expression analyses following steatosis associated with alcohol feeding showed increased hepatic ceramide levels associated with higher levels of the precursor molecules sphingosine and sphinganine. 20
β-glucosylceramide (GC) is a naturally occurring intermediate in the metabolic pathways of complex glycosphingolipids and has been suggested to exert an effect on the immune system. 21 –23 Previous studies have suggested that GC exerts a beneficial effect in animal models of diabetes and NASH. 24,25 A phase I clinical trial demonstrated that oral administration of GC is safe in humans. 26
The aim of the present study was to determine the safety and efficacy of orally administered GC in patients with insulin resistance and NASH.
Materials and Methods
Patient population
A randomized double-blind, placebo-controlled, one-center trial was conducted in subjects with NASH. The study was carried out in accordance with the guidelines of the Hebrew University-Hadassah Institutional Committee for Human Clinical Trials, and the approval of the Israel Ministry of Health Committee for Human Trials.
Inclusion criteria
Forty subjects (men and women ≥18 and ≤60 years of age) were evaluated for eligibility after they had signed a written informed consent form (ICF). The diagnosis of NASH was based on liver biopsy, with a NASH score of 6 or above, performed within 6 months before enrollment in the trial. All subjects completed the informed consent process culminating with written informed consent by the subject. Patients diagnosed with type 2 diabetes (nontreated or treated with up to two drugs [excluding insulin] on stable medication two months before enrolment and an HbA1C between 6.0 and 8. No evidence of other viral or immune-mediated liver disease.
Exclusion criteria
Subjects were excluded if they had active coinfection with hepatitis A, B, or C viruses, or were infected with human immunodeficiency virus infection, or diagnosed with hepatocellular carcinoma, fulminant liver failure, or severe deteriorating synthetic liver functions. Subjects with chronic inflammatory diseases such as rheumatoid arthritis or inflammatory bowel disease were excluded.
Study drug preparation and administration
Subjects who fulfilled the inclusion/exclusion criteria for participation in the study were instructed to take a daily oral dose of the study drug or placebo for a period of 40 weeks. The study drug β-d-glucosylceramide (EGS21, GC) purchased from Avanti Polar Lipids, Inc., Alabaster, Alabama, USA, or placebo, were prepared as a liquid form. Each vial consisted of 7.5 mg of GC dissolved in 5 mL phosphate-buffered saline (PBS).
Randomization
Subjects were randomized by a computer-generated randomization to receive either the study drug or the placebo. All subjects and investigators were blinded regarding treatment allocation. Confidentiality of the blinding code was maintained by an independent statistician.
Clinical and laboratory follow-up
Subjects were followed every 8 weeks. The visits included physical examination, medical history review, and laboratory tests to assess safety and record any adverse events. The laboratory tests included the following: blood counts (CBC), sedimentation rate (ESR), liver enzymes, INR, lipid profile, CRP, HbA1c, and serum insulin levels. In addition, as a means of identifying possible surrogate markers to assess the clinical effect of the study drug, FACS analysis of peripheral blood T cell populations was performed on specimens obtained every 8 weeks throughout the trial. At the end of the study, all patients underwent an additional oral glucose tolerance test (OGTT), liver biopsy, and a MRI for assessment of hepatic fat content.
Primary endpoints
An improvement of 2 points in the NASH score on liver biopsy and/or a decrease of 0.5 in HbA1c.
Secondary endpoints
Decreases in liver enzymes, a 10% decrease in hepatic fat content as measured by MRI and improvement of insulin sensitivity (Matsuda index from oral glucose tolerance assessment) improved lipid profile. Serum fasting AST, ALT, glucose, insulin, cholesterol, and triglyceride levels were measured by standard techniques.
Assessment of hepatic fat by MRI
Hepatic fat content was measured with a double-echo chemical shift gradient-echo sequence technique, which provides in-phase and out-of-phase images in a single acquisition for the assessment and quantification of fat. T1-weighted out-of-phase MRI is sensitive for detection of relatively small proportions of tissue fat as described. 24,27 Magnetic resonance images were acquired with a 1.5-T system (Sigma LX; General Electric, Milwaukee, WI, USA). Double-echo MRI was performed with a repetition time (TR) of 125 msec, double echo times (TEs) of 4 and 6.5 msec, and a flip angle of 80°. Imaging parameters included a section thickness of 3 mm, a 13-cm field of view (or larger, up to 40 cm (accordance with patient size), and a 256 × 160 matrix. Axial and coronal images were obtained. Signal intensity (SI) changes between in-phase and out-of-phase images were computed. The SI index was calculated as follows: SI index (SII) = (SIip − Siop)/SIip (SIip = in-phase SI; SIop = out-of-phase SI). Low SI index values indicate a smaller amount of tissue fat.
Histological scoring
Liver biopsies were stained with hematoxylin eosin and reviewed by an experienced pathologist in a blinded manner using the accepted NASH score. 28
Flow cytometry analysis determining changes in immune cell population
Blood samples were collected throughout the study period. Immediately following lymphocyte isolation, duplicates of 2–5 × 104 cells/500 μL PBS were deposited into Falcon 2052 tubes incubated with 4 mL of 1% bovine serum albumin (BSA) for 10 min. Cells were again suspended in 10 μL fetal bovine serum with either 1:20 FITC-antihuman CD3, CD4, CD8, or CD56 antibodies (Pharmingen, and R&D, USA) and mixed every 10 min for 30 min. After the cells were washed twice with 1% BSA, 0.5 mL of 1% paraformaldehyde was added and the cells were kept at 4°C until reading. For the control group, only 5 μL of 1% BSA was added. Cell phenotyping was performed by a FACSTAR plus, (Becton Dickinson). Live cells only were counted, and background fluorescence from nonantibody-treated lymphocytes was subtracted.
Sample size and power
Twenty-three subjects were enrolled and 20 randomized and treated according to the protocol. The study was not powered to detect rarely occurring treatment-associated adverse events. Summary statistics by time point of all clinical and laboratory variables were calculated, and statistical significance of changes from baseline was assessed by Student's t-test.
Results
Study population: intent-to-treat population and per protocol population
The intent-to-treat (ITT) included all randomized/enrolled patients who received a subject study number, signed the ICF, and received at least one dose of study medication. The ITT population included 23 subjects. Three patients were not enrolled due to screening failure (n = 2) or lack of compliance (n = 1).
Protocol population (PP) included all randomized subjects who completed the study according to the protocol. The PP population included 20 subjects (12 subjects in the GC-treated cohort and 8 subjects in the control cohort).
The study population was too small to reach statistical significance in most parameters; nevertheless, trends could be determined. Analyses were conducted on the PP population. A full data analysis is enclosed in the Supplementary Data (Supplementary Data are available online at
Oral administration of GC was safe and no adverse effects were noted in treated patients.
Effect of oral administration of GC on liver
Figure 1 shows the effect of treatment with GC on the assessment of intrahepatic fat accumulation by MRI. A decrease from 40.33 to 34.66 in the SI was noted following 40 weeks of treatment in the GC-treated group, a decrease of 14%, compared with a milder decrease from 28.76 to 26.54 in the SI, and in placebo-treated controls, a decrease of 7.7% (P = .07). The data suggest that similar to the preclinical data, oral administration of GC can prevent the slow rate of hepatic steatosis. This effect was obtained irrespective of the change in body weight and body mass index (BMI). A 1.91% decrease in BMI was noted in GC-treated group compared with 2.95% decrease in the placebo (P = non significant [NS]).

Effect of GC treatment on intrahepatic fat accumulation by MRI. Patients underwent MRI-quantification of intrahepatic steatosis at the start and end of trial. The decrease in SI score between the start (open bars) and end (black bars) of study was ameliorated in GC-treated patients compared with the placebo group (P = NS).GC, β-glucosylceramide.
No significant effect was noted between the treated and placebo groups on serum levels of ALT, AST, and GGT liver enzymes (see Supplementary Data). Ten of the patients in the drug-treated group and seven of the patients in the placebo group completed a second liver biopsy. No significant differences were noted between the groups on liver biopsy NASH score.
Effect of oral administration of GC on insulin resistance
Figure 2 shows the effect of treatment on HbA1C levels. Patients in the GC-treated group exhibited a trend for decreased HbA1C serum levels from 6.07 to 5.97 g%, while in the placebo-treated group an increase from 6.28 to 6.37 g% was noted (P = NS).
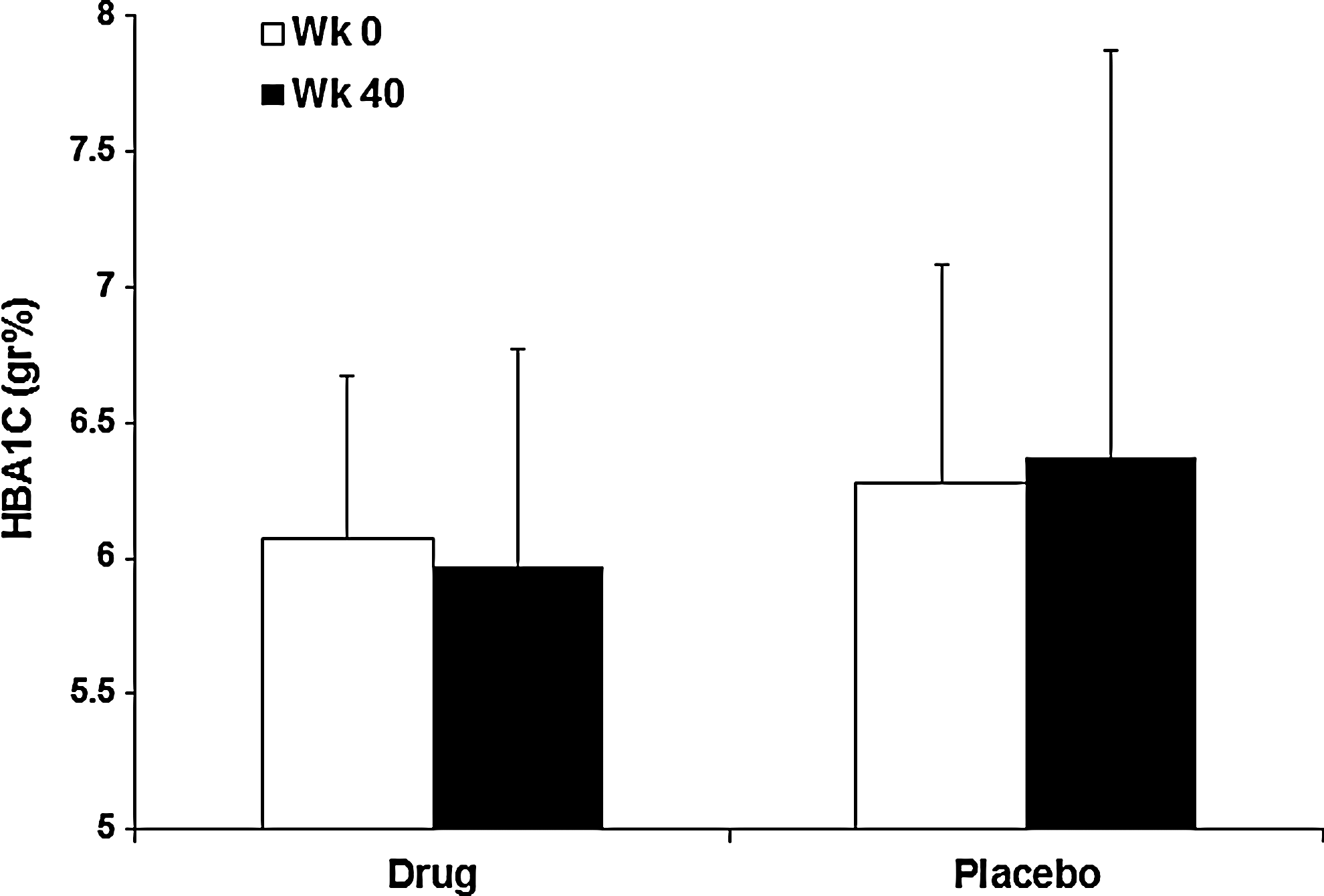
Effect of oral administration of GC on HbA1Cs serum levels. A decrease in HBA1C serum levels between the start (open bars) and end of study (black bars) was noted in GC-treated patients compared with an increase in the placebo control group (P = NS).
Figure 3 shows the effect of treatment on an intravenous glucose tolerance test. The decrease in insulin secretion calculated as the area under the curve (AUC) during OGTT was attenuated in GC-treated patients who exhibited a 3.6% decrease compared with a decrease of 9.1% in placebo-treated patients. Glucose AUC decreased by 0.01% in the GC-treated patients compared with a 3.5% increase in placebo-treated patients (P = NS). These trends may suggest a beneficial effect on GC on the glucose metabolism. No significant difference in the change in fasting blood glucose and HOMA scores was noted between the two groups.
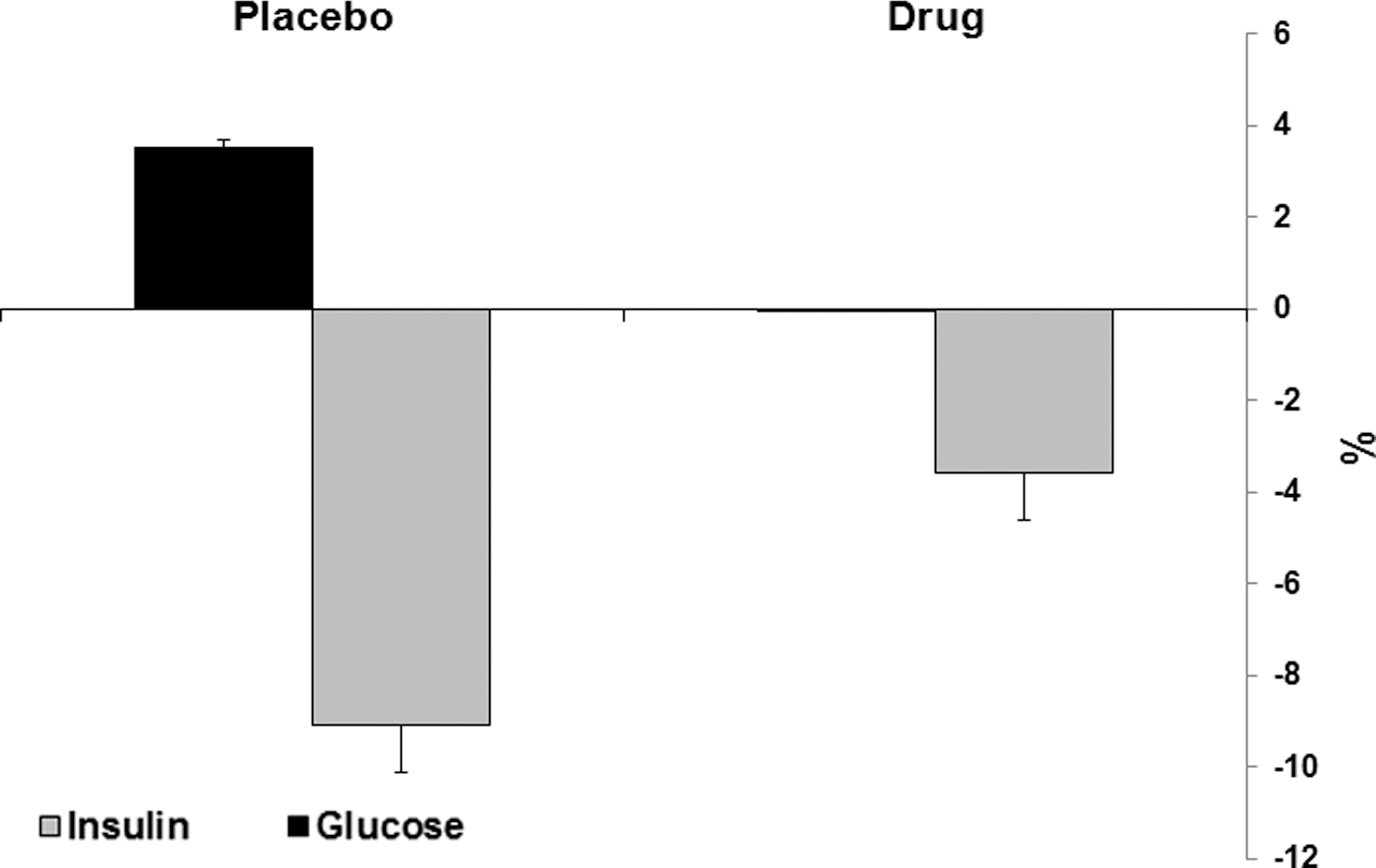
Effect of GC treatment on insulin resistance. Patients underwent an intravenous glucose tolerance test at the start and end of trial. GC treatment ameliorated the decrease in insulin (grey bars) and glucose (black bars) change. Insulin area under the curve (AUC) decreased by only 3.6% in GC-treated compared with a 9.1% decrease in placebo controls; The glucose AUC decreased by 0.01% compared with a 3.5% increase in controls (P = NS).
Effect of oral administration of GC on blood lipids and immune cells
In the placebo group a 17.2% decrease was noted in high-density lipoprotein cholesterol levels compared with only 6.99% decrease in the GC-treated group (Fig. 4, P = NS). No differences were noted between the drug and the placebo-treated groups for total cholesterol, low-density lipoprotein cholesterol, and triglycerides levels.
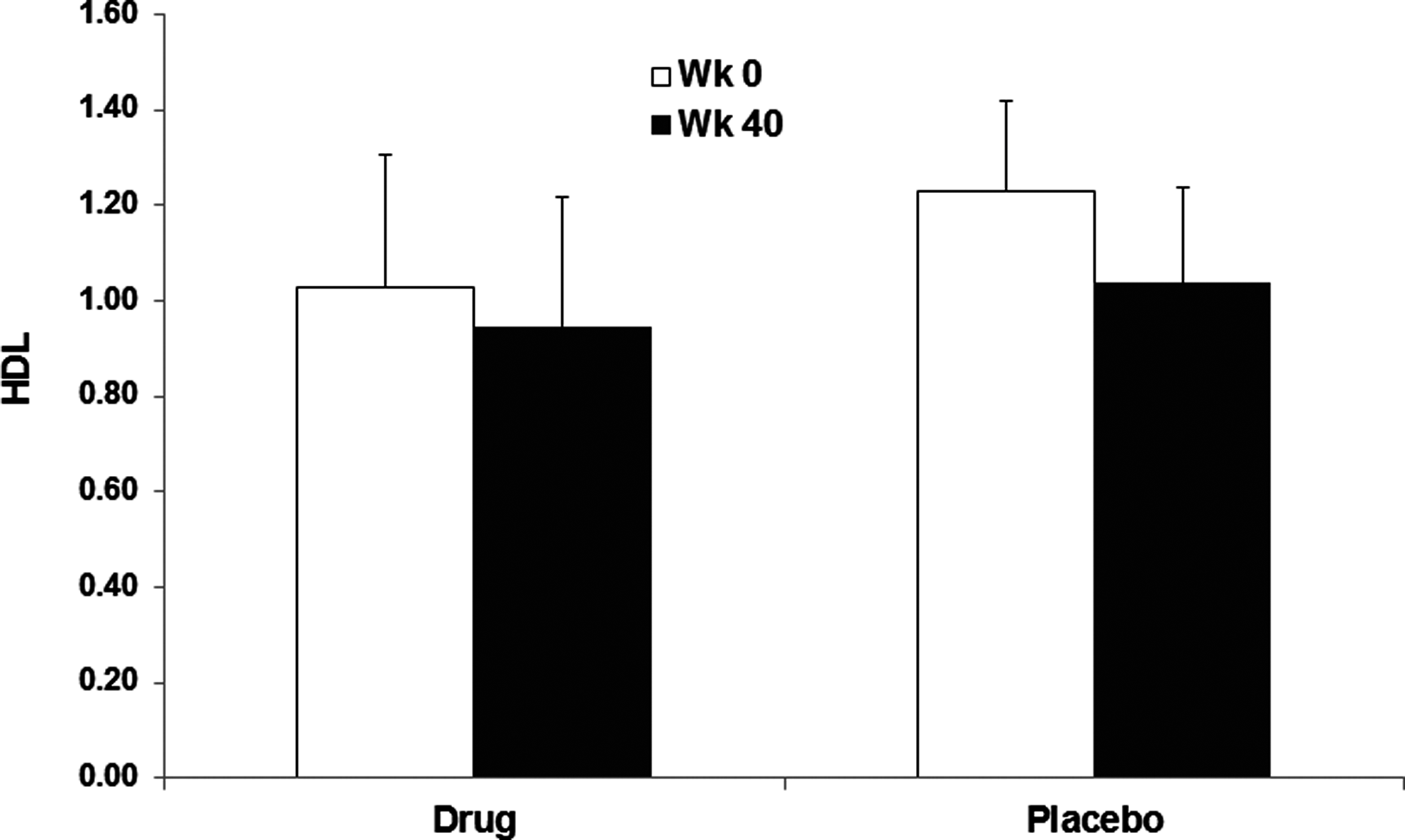
Effect of oral administration of GC on HDL cholesterol serum levels. The decrease in HDL levels between the start (open bars) and end (black bars) of study was ameliorated in GC-treated patients compared with the placebo group (P = NS). HDL, high-density lipoprotein.
Figure 5A shows the effect of treatment with GC on the CD4 lymphocyte population. GC treatment was associated with a decrease from 36.63% to 31.06% in CD4 cells, compared with an increase from 28.23% to 30.27% in controls (P = NS). Figure 5B shows that the NKT lymphocyte subset (CD3+CD56+) decreased in the GC-treated group from 1.86% to 1.5% compared with an increase from 3.41–3.71 in controls (P = NS).

Discussion
The data of the present study show that oral administration of β-glucosylceramide is safe and shows a tendency to protect or prevent deterioration in patients with insulin resistance and NASH. The study population was too small to reach statistical significance in most parameters; nevertheless, trends could be determined. We have shown that both the degree of insulin resistance, HbA1C, and steatosis were maintained and showed slight improvement in treated patients compared with the placebo controls that continued to deteriorate. These effects were associated with alterations in the CD4+ and NKT subsets of lymphocytes. The data of the present study show that GC improves insulin resistance as indicated by the decrease in the insulin AUC.
The beneficial effect of GC in these patients can be explained by its effect as an immune modulatory adjuvant in the gut-associated lymphoid system, and/or its effect on glycosphingolipid pathway. Alternatively, it can also be explained by its potential role in changing the balance of various intermediates in these pathways as suggested in previous studies. 19,20 Metabolomics profiling, liquid chromatography mass spectrometry, and gene expression analyses show alterations in the sphingosine metabolism in patients with NASH. 19,20 Ceramide and/or its glycosphingolipid metabolites were suggested to play a role in the pathogenesis of insulin resistance. 29,30
Type I Gaucher disease, a lysosomal storage disorder, is associated with high serum levels of GC. These patients suffers from metabolic abnormalities such as high resting energy expenditure, low circulating adiponectin, and peripheral insulin resistance. 31
Several studies suggested that by reducing GC serum levels, one could alleviate insulin resistance. Treatment of ob/ob mice with the iminosugar derivative N-(5′-adamantane-1′-yl-methoxy)-pentyl-1-deoxynojirimycin (AMP-DNM), an inhibitor of glucosylceramide synthase, an enzyme that catalyzes a necessary step in the conversion of ceramide to glycosphingolipids, normalized their elevated tissue glucosylceramide levels, lowered circulating glucose levels, improved oral glucose tolerance, reduced HbA1C, and improved insulin sensitivity in muscle and liver. 29,32
In the Zucker diabetic fatty rats, a reduction in blood glucose levels and improved glucose tolerance were achieved by lowering glycosphingolipid levels, using a glucosylceramide synthase inhibitor (1R, 2R)-nonanoic acid[2-(2′,3′-dihydro-benzo [1, 4] dioxin-6′-yl)-2-hydroxy-1-pyrrolidin-1-ylmethyl-ethyl]- amide-l-tartaric acid salt (Genz-123346). 29,33 Treatment prevented the loss of pancreatic beta-cell function.
Glycosphingolipids were suggested to negatively modulate the activity of the insulin receptor, 34 the use of Genz-123346, an inhibitor of glycosphingolipid synthesis, was hypothesized to improve insulin sensitivity and glucose control. However, Genz-123346 did not alter insulin secretion, suggesting that its effect is mainly due to increase in peripheral insulin sensitivity. 33 This may underline the different effect noted in the hyperglycemic Cohen diabetic rats, which do not exhibit peripheral insulin resistance, and diabetes development is solely attributed to of β-cell dysfunction. 25
The conflicting results about the potential association of GC and diabetes may be related to a lack of ability to measure an effect of these inhibitors on different types of glycosphingolipids, thereby isolating the levels of serum GC from those of other metabolites that might be changed by their administration and the characteristic of the animal model studied.
Moreover, in untreated Gaucher patients the prevalence of obesity is lower than in the general population. 35 Long-term treatment with enzyme therapy, reducing the GC serum levels, induces a larger than average weight gain leading to a similar prevalence of obesity in enzyme therapy-treated patients and the general population. 36 Furthermore, most patients with Gaucher disease do not have overt diabetes, making it unlikely that GC serum levels explain the beneficial effect of GC-lowering agents in insulin resistance. Furthermore, the prevalence of type 2 diabetes increases significantly during treatment with enzyme therapy. 36 Elevated GC levels were recently suggested as a potential evolutionary benefit for patients with Gaucher disease. 30,35
Glycosphingolipids are important components of cell membranes. A potential interaction between altered glycosphingolipid levels and the insulin receptor on cell membranes was suggested important in the pathogenesis of insulin resistance. 37,38 In the diet-induced obese mouse, treatment with Genz-123346 normalized HbA1C levels and improved glucose tolerance and was associated with alteration of the phosphorylation state of the insulin receptor and downstream effectors showed increased insulin signaling in the muscles of the treated Zucker diabetic fatty rats and diet-induced obese mice. 33 The improvement noted with the GC in immune-mediated disorders was also suggested to be associated with an effect on lipid rafts and intracellular signaling pathways. 39,40
Modulation of the immune system can improve glucose metabolism in both human patients and animal models of diabetes. 33,41 GC was shown to exert an immune modulatory effects in various models, including animal models of NASH, and also in humans. 42 Potential mechanisms that may explain the noted effect are associated with a primary immune modulatory effects on regulatory T cells (Tregs), and/or NKT cells, or any other immune cell involved in the pathogenesis of insulin resistance and chronic inflammation in NASH. 17,43,44
NKT cells are a subset of innate immune cells that express a highly restricted repertoire of T-cell receptors that recognize glycosphingolipid antigens bound with the antigen-presenting molecule CD1d. 45 This subset of cells produces immunomodulatory cytokines upon antigenic stimulation, which endows these cells with potent immunoregulatory properties. 45 NKT cells have increased presence in the liver and participate in the inflammatory processes during hepatic diseases. 46 In patients and mice with a variety of autoimmune diseases, numbers and functions of NKT cells are disturbed. 45 In some mouse models of autoimmunity, NKT cell deficiency exacerbates disease, suggesting that NKT cells play a role in suppressing autoimmunity. Activation of NKT cells with glycosphingolipid antigens protects mice against the development of autoimmunity. Activation of these cells protects non obese diabetic (NOD) mice from T1DM development. 47,48 Most studies have used the potent sponge-derived NKT cell antigen alpha-galactosylceramide (alpha-GalCer). 45 β-glycosphingolipids have emerged as a family of potential ligands for NKT cells 49 and alter immune responses in the opposing settings of autoimmune diseases or cancer. 20,21,23,42,50 NKT cells were described to have a role in the pathogenesis of NASH in animal models. 27,51 –55 By exerting an immunomodulatory effect, β-glycosphingolipids improve the β-cell function and glucose intolerance. 24,25 In some models, the beneficial effect was associated with alteration of NKT cell distribution manifested by increased intrahepatic NKT lymphocytes.
The small number of patients enrolled in the trial did not enable reaching statistical significance for the tested parameters. The relatively short follow-up period may explain the lack of a profound effect on liver fibrogenesis, which may require longer periods of treatment. An additional hurdle may be the use of a relatively small dose of GC, while studies in animal models suggested that higher dosage may exert a more profound effect.
In summary, oral administration of GC to patients with NASH and insulin resistance is safe and retains its biological activity. We demonstrated a trend for beneficial effects on liver and diabetes parameters. We propose to design a study with a larger cohorts combined with long-term administration of higher doses of GC that may have a more significant effect on preventing the progression of the disease.
Footnotes
Acknowledgments
This work was supported, in part, by ENZO Biochem, NYC, NY, and by The Roman-Epstein Liver Research Foundation (to Y.I.) and by the US-Israel BIRD Foundation.
Author Disclosure Statement
Y.I. is a Consultant for ENZO Biochem, NYC, NY, and a medical director for Natural Shield. For all other authors, no competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.