
Abstract
Anthocyanin-rich black soybeans have been used in traditional East Asian medicine to cure diseases related to oxidative stress and carcinogens, but not obesity. Our objective was to investigate the effects of anthocyanin-rich black soybean testa extracts (BBT), Glycine max (Chongja No. 3), on obesity. In total, 63 participants defined as overweight or obese by their body mass index (BMI >23) or waist circumference (WC >90 cm for males, >85 cm for females) were sorted into two groups: 32 receiving the trial medication (BBT, 2.5 g/d) and 31 receiving the placebo (starch, 2.5 g/d). Participants completed an 8-week, randomized, double-blinded, and placebo-controlled clinical trial. There were no significant differences between the two groups at the beginning of the trial, and both required the same safety assessments. Significant decreases in abdominal fat, described according to WC and hip circumference, and lipid profiles such as triacylglycerols (TG), low density lipoprotein cholesterol (LDLc), and non-high density lipoprotein cholesterol (non-HDLc) were observed in the BBT group at the conclusion of the clinical trial. The indicators for arteriosclerosis such as total cholesterol (TC)/HDLc and LDLc/HDLc were significantly decreased in the BBT group, but had not changed in the placebo group. With no difference between the two groups in energy-adjusted dietary intakes and physical activity, BBT was shown to strongly improve plasma lipid profiles, related to the reduction of WC (an indicator of abdominal fat) as long as high dietary fiber and low cholesterol diets were maintained. In conclusion, BBT can potentially be developed as a functional food for preventing abdominal obesity with high fiber and low cholesterol diets.
Introduction
O
Black soybeans are native to Northeast Asia and are a member of the Leguminosae family of herbaceous annuals. Because their functional components include isoflavones, saponins, lecithin, and oligosaccharides, black soybeans have been used in traditional East Asian medicine to treat skin troubles, pulmonary symptoms, asthma, gastric ulcers, renal diseases, and beriberi. 9,10 Recent studies have examined the safety and antioxidative and anticarcinogenic effects of black soybean pigment, but the antiobesity effects of anthocyanins in black soybean have not yet been shown. 11 –14 We observed antiobesity and lipid-lowering effects in anthocyanin-rich black soybeans that were consistent with those of previously published studies. 15 We conducted an in vitro study before performing a randomized clinical trial and found that black soybean testa extracts (BBT) inhibited fat accumulation and related factors such as peroxisome proliferator-activated receptor gamma (PPARγ) and CCAAT enhancer binding protein alpha (C/EBPα) in adipocytes induced from preadipocytes. When BBT was administered to a high-fat diet-induced obesity (DIO) model, the BBT group exhibited a decrease in the expression of insulin, leptin, PPARγ, C/EBPα, cytokines, tumor necrosis factors-α (TNF-α), body weight, abdominal fat, and the infiltration of macrophages, and an increase in adiponectin levels compared to the DIO only. 16 Based on previous research, we scientifically examined the preventive and therapeutic effects of BBT treatment on obesity. This article demonstrates new possibilities for black soybeans to contribute to the improvement of national healthcare.
Materials and Methods
Research design
Our study was conducted as an 8-week planned, randomized double-blind placebo-controlled clinical trial (RCT). The 80 final enrolled participants were allocated, according to a computer-generated randomization schedule into either the BBT (n = 40) or placebo (n = 40) group; the groups were maintained equal in size to ensure maximum statistical power. Neither the investigators nor the participants knew the randomization code or the results. During their first and second visits, participants were given a 4-week supply of the test products after their physical measurements were recorded. During the 8-week RCT, the staff monitored participants for the occurrence of any adverse effects, and at the close of the RCT, participants were asked to return for tests of lipid biomarkers and anthropometrics (Fig. 1). The Institutional Review Board of Hanyang University Hospital (HY-14-04-09) approved and conducted this study. It was performed in accordance with the Declaration of Helsinki, and written informed consent was obtained from all participants. This trial was registered at

Flow diagram of four phases (enrollment, random allocation, follow-up, and data analysis) for 8-week randomized controlled trial of the two groups. Color images available online at
Study products and compliance
The extracts of black soybean testa [Chongja No. 3, Glycine max (L.) Merr.] used in the previous in vitro and in vivo studies were the same substance used for this human study. 16 Anthocyanins in BBT extracted in 60% ethanol and concentrated were analyzed by HPLC (Dionex Ultimate 300 series; Dionex softron GmbH, Germering, Germany). BBT was low in calories (3.3 kcal/g extracts) and rich in anthocyanins (12.58 mg/g extract) with three majors such as cyanidin-3-glucoside (C3G), delphinidin-3-glucoside (D3G), and petunidin-3-glucoside (P3G) distributed by 68.3%, 25.5%, and 6.5% of total anthocyanins. The others, such as cyanidin-3-galactoside, pelargonidin-3-glucoside, peonidin-3-glucoside, and cyanidin, including undetectable anthocyanins, were <5% in BBT. Both the BBT and the placebo were manufactured by In-Sung Pharmaceuticals. The BBT was composed of 100% BBT, whereas the placebo was composed of 97% starch and 3% natural dark purple pigment. The BBT group was directed to consume two capsules orally before each of the three daily meals for a total of 2.5 g/d. The placebo group was given identical instructions. At each visit, we collected the remaining capsules from the participants and investigated their rate of compliance; participants with a rate of under 70% were eliminated from the final study analysis. The percentages of compliance were calculated by dividing the actual intake (total supplied capsules−returned capsules) by the planned intake (168 capsules over 4 weeks).
Medical history and physical measurements
On signing the agreement, a 3-year medical history was taken for each participant. Any symptoms that worsened during the trial were recorded as abnormalities, and prescription histories were precisely recorded. Blood pressure, the pulse rate, and vital signs were measured before the collection of blood. BMI (kg/m2) was calculated by dividing the body weight (kg) by the height squared (m2). WC and hip circumference (HC) were measured, and the waist–hip ratio (WHR) was calculated by dividing WC by HC. Body fat mass (BFM), body fat percentage, and fat-free mass (FFM) were measured using dual energy X-ray absorptiometry (DEXA).
Blood and urinary biochemistry
Blood and urine were collected from each participant after 12 h of fasting. Hematology laboratory tests, blood chemistry assays, and urinalysis were performed with a Coulter STKS hemocytometer (Beckman Coulter, Inc., Fullerton, CA, USA), a Hitachi 7150 automated analyzer (Hitachi Ltd., Tokyo, Japan), and a Clinitek Atlas automated urine chemistry analyzer (Siemens Healthcare Diagnostics, NY, USA), respectively. All analyses were performed at the Korea Biomedical Laboratory by using the Bio-Plex cytokine assay kit (Bio-Rad Laboratories, Inc., Hercules, CA, USA) according to the manufacturer protocols, except non-high density lipoprotein cholesterol (HDLc). Non-HDLc was calculated from very low density lipoprotein cholesterol (VLDLc) plus low density lipoprotein cholesterol (LDLc). Data analysis was performed with Bio-Plex Manager 6.1 software (Bio-Rad Laboratories, Inc.).
Diet survey and physical activity questionnaire
Participants were asked not to make any changes to their usual lifestyle and diet during the study. Three-day dietary records, including 2 weekdays and 1 weekend day, were collected to monitor dietary changes at weeks 0, 4, and 8. These records were analyzed with CAN pro 4.0 (Computer Aided Analysis Program 4.0 for professionals, Korean Society of Nutrition, Seoul, Korea). A trained coordinator asked participants to fill out a global physical activity questionnaire to monitor changes in physical activity at weeks 0, 4, and 8.
Statistics
The sample size was calculated as follows. One of the primary measures of outcome was the amount of BFM decrease, assuming 0.77 kg in the BBT group and 0.16 kg in the placebo group, with a standard deviation of 0.98 kg, α set at 5%, and power at 80%. This resulted in 32 participants qualifying from each group, with a dropout rate of 20%. In this study, the data from the participants were analyzed in three ways: a safety group; intention-to-treat (ITT) group; and per protocol (PP) group. The safety group included all participants who had taken the capsules at least once during the trial, the ITT group refers to the participants whose measurements for the main indicators were taken at least once after taking the capsules, and the PP group refers to the participants in the ITT group who fulfilled our requirements. The validity test was analyzed based on the PP group, and the safety group was the basis for the safety assessment.
The descriptive differences between groups in the participant population were analyzed using an independent t-test for mean comparison and the chi-square test for ratio comparison. Fisher's exact test was used for smoking because it was a nonparametric term. A paired t-test was used to analyze changes in major indicators before and after treatment. Repeated measures analysis of variance (RM ANOVA) was used to analyze the comparison between the safety and PP groups and for repeated measures within the groups. A linear mixed model was used to analyze dietary intake and physical activity. Reported abnormalities during the trial were recorded, and the incidence was calculated in proportion to the total participant population. The analysis was performed using Fisher's exact test. A paired t-test was used for the mean comparison of clinical pathology tests and vital signs before and after treatment, and a linear mixed model was used for vital signs because the term possesses three comparative periods. The comparison between the two groups was performed by a linear mixed model.
Results
Compliance and general characteristics
During the progress of the trial, six participants (two from BBT, four from placebo) dropped out: four by consent withdrawal, one for protocol violation (doping), and one because of an abnormality. In addition, 11 participants (six from the BBT group, five from the placebo group) were measured at under 70% compliance and ruled out in the analysis as a result. Compliance was 90.08% in the BBT group and 89.18% in the placebo group, showing no statistical significance. In total, 63 participants (32 from the BBT group, 31 from the placebo group; 78.8% in total) completed the 8-week research plan (Table 1). Because of the lack of a significant difference between the anthropometrics of the two groups, such as their BMI, WC, WHR, and BP, and lifestyle habits, such as alcohol consumption and smoking, the participants were randomly allocated at the baseline.
Values are presented as mean ± SD.
Analyzed by Independent t-test.
Analyzed by chi-square test.
Analyzed by Fisher's exact test.
Compliance was calculated by total intakes by prescriptions.
Analyzed by Student's t-test.
BMI, body mass index; DBP, diastolic blood pressure; HC, hip circumference; N.S., statistically nonsignificant; SBP, systolic blood pressure; WC, waist circumference; WHR, waist–hip ratio.
Changes in anthropometrics and blood chemistry resulting from BBT treatment
Significance assessment was assigned, based on PP, to the 63 participants who fulfilled our criteria for analysis until the end of the trial. BFM and FFM did not differ between the BBT and control groups (Table 2). However, WC, the indicator of abdominal fat, was significantly decreased in the BBT group despite an increase in BFM (Fig. 2). Moreover, there were strong positive correlations between BFM and BMI (r = 0.484, p < .0001), WC and BMI (r = 0.413, p = .001), and WC and WHR (r = 0.686, p < .0001) before and after treatment. All blood biomarkers for lipid metabolism were decreased in the BBT group, and total cholesterol (TC), LDLc, HDLc, and VLDLc were decreased in the placebo group (Table 2). There were differences in the plasma LDLc, non-HDLc, and LDL/HDL ratios between the two groups, both before and after the 8-week trial. Hematologic indicators for arteriosclerosis, such as TC/HDLc and LDLc/HDLc, were significantly decreased in the BBT group, but showed no difference in the placebo group (Fig. 2). The inflammatory cytokines TNF-α and MCP-1 were significantly decreased in both groups with no statistical difference between them.
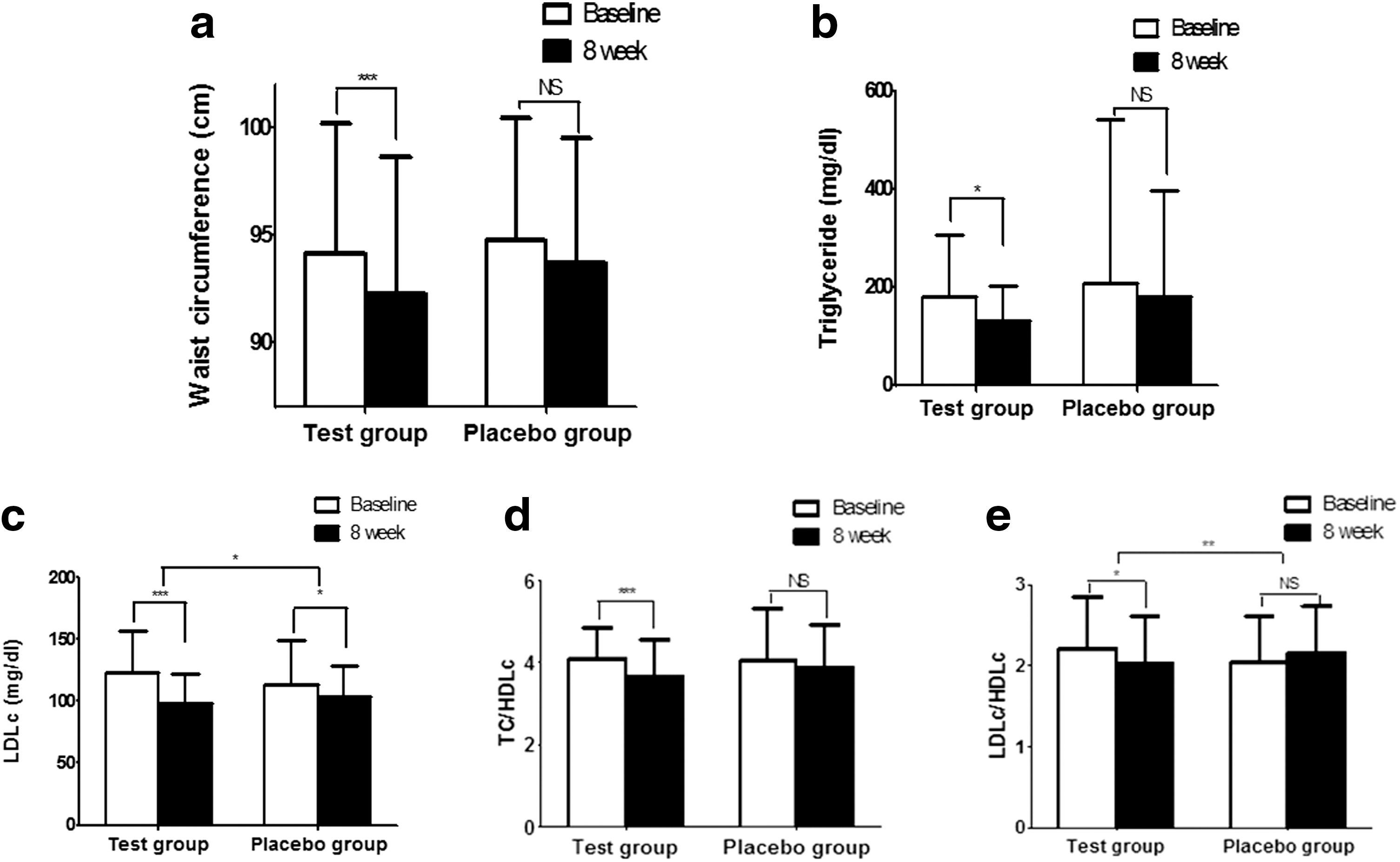
Changes in WC
Values are presented as mean ± SD.
Analyzed by paired t-test.
Analyzed by RM ANOVA.
BFM, body fat mass; DEXA, dual energy X-ray absorptiometry; FFM, fat-free mass; HDLc, high density lipoprotein cholesterol; IL-6/-10, Interleukin-6/-10; LDLc, low density lipoprotein cholesterol; MCP-1, monocyte chemoattractant protein-1; RM ANOVA, repeated measures analysis of variance; TC, total cholesterol; TG, triacylglycerols; TNF-α, tumor necrosis factor-α; VLDLc, very low density lipoprotein cholesterol.
Dietary survey and physical activity
The dietary intakes and physical activities of the participants were measured at every visit (Table 3). Analyzing the dietary intake data adjusted by caloric intake, we found that only plant fat was decreased in the BBT group, with no other statistical differences between the two groups, both with and without the adjustment. According to linear regression analysis, a strong negative correlation (R 2 = 0.18, p = .016) between changes in BFM and changes in dietary fiber intake was found in the BBT group; this phenomenon was not significant in the placebo group. BBT group also showed a strongly positive correlation between changes in WC and changes in cholesterol intakes (R 2 = 0.23, p = .043), but not in the placebo group (Fig. 3). Even though the changes in dietary fiber and cholesterol intakes during the experimental period were not different in either the test or placebo group, these results supported that the visceral fat accumulation may be decreased by consuming diets high in anthocyanins and dietary fiber and low in cholesterol. Physical activity, described by metabolic equivalent of task (MET)-min/week, did not change before or after treatment in either group.
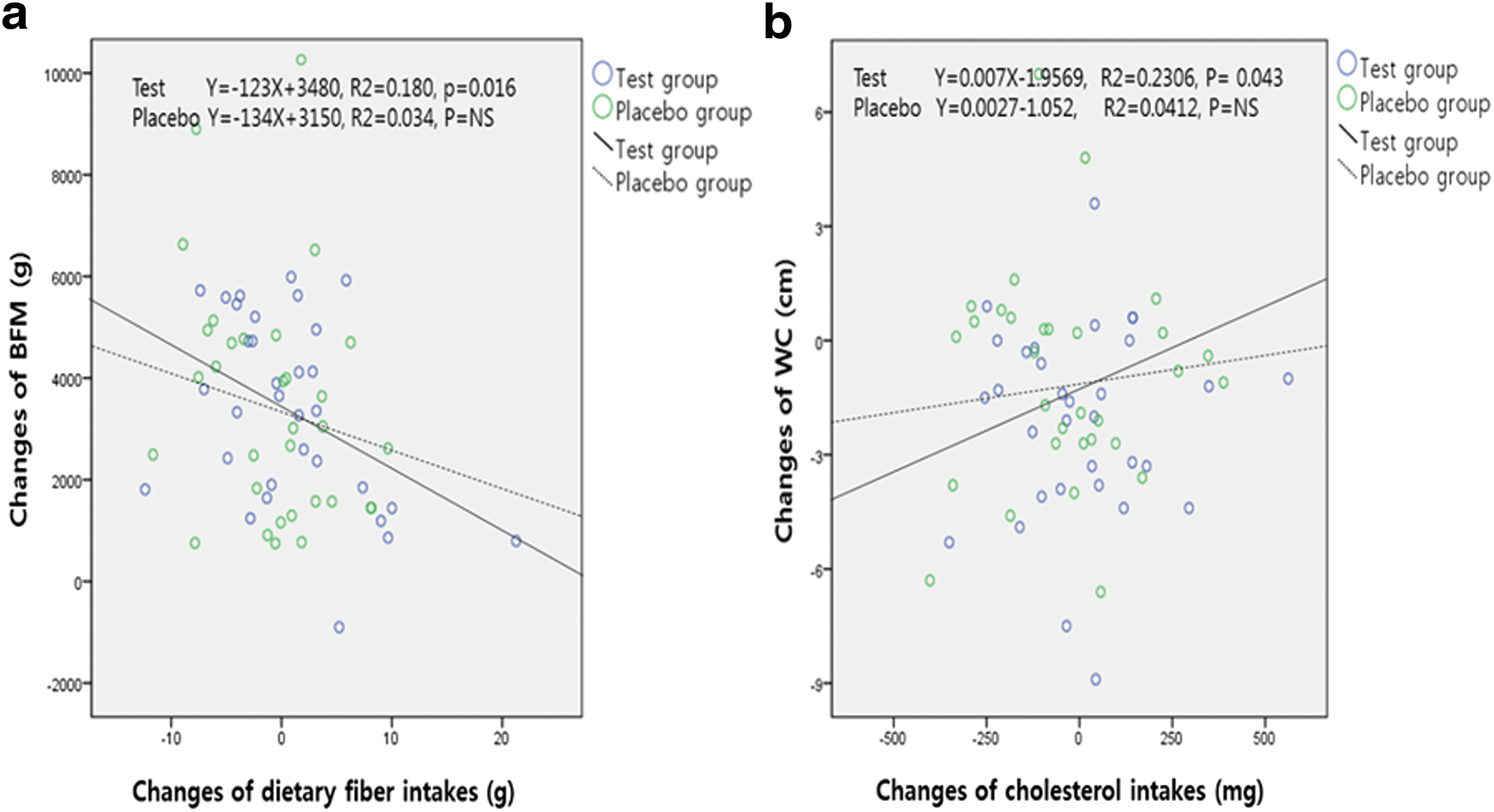
Regression between changes of body fat mass and changes of dietary fiber intakes
Values are presented as mean ± SD.
Analyzed by paired t-test.
Analyzed by linear mixed model for repeated measures data adjusted by energy intakes (kcal).
Analyzed by linear mixed model for repeated measures data.
MET, metabolic equivalent of task (min/week).
Safety assessment
Of the 80 participants, 19 cases of mild or moderate abnormalities were reported among 17 participants (21.25%): 8 cases from 7 participants (17.5%) in the BBT and 11 cases from 10 participants (10%) in the placebo. Reported abnormalities were two cases of colds, two cases of headaches, one case of bruising, one case of menstrual pain, one case of enteritis, and one case of ulitis from the BBT and two cases of colds, one case of diarrhea, one case of muscular pain, one case of otitis, one case of laryngitis, one case of fatigue, one case of xerophthalmia, one case of rash, one case of conjunctivitis, and one case of possible hepatosis from the placebo group. There was no difference between the two groups in the incidence rate of abnormalities, indicating that there was no causal relationship between these abnormalities and BBT. A clinical pathology test (complete blood count, biochemical test, and urine test) was administered at the third visit (Table 4). The results did not demonstrate a statistically significant difference between the two groups. Vital signs (systolic pressure, diastolic pressure, and pulse) were measured at every visit without any statistically significant difference observed between the two groups; the values were of no clinical significance (Table 3).
Values are presented as mean ± SD. Normal Ranges for clinical markers; WBC (4–10 × 103/μL), RBC (3.9–6.4 × 1003/μL), Hemoglobin (12.0–18.0 g/dL), Hematocrit (36–52%), Platelet (150–400 × 103/μL), Total bilirubin (0.1–1.0 mg/dL), ALP (60–300 IU/L), gamma-GTP (5–50 IU/L), ALT (5–40 IU/L), AST (5–37 IU/L), Glucose (70–120 mg/dL), Total protein (6.4–8.3 g/dL), Albumin (3.8–5.3 g/dL), BUN (8–20 mg/dL), Creatinine (0.6–1.4 mg/dL), Creatinine Kinase (30–190 IU/L), LDH (200–400 IU/L), SG (1.005–1.030), and Ph (5.0 ∼ 8.0).
Analyzed by paired t-test.
Analyzed by linear mixed model for repeated measures data.
ALP, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BUN, blood urea nitrogen; LDH, lactate dehydrogenase; RBC, red blood cells; r-GTP, gamma-glutamyl transpeptidase; SG, specific gravity; WBC, white blood cells.
Discussion
In our previous in vitro study, we found that the extracts of BBT inhibited fat accumulation and related factors such as peroxisome proliferator-activated receptor gamma (PPARγ) and CCAAT enhancer binding protein alpha (C/EBPα) in adipocytes induced from preadipocytes. 15 According to previous DIO studies, BBT markedly reduced body fat and the final sizes of adipocytes while also reducing triacylglycerols (TG) levels in plasma and the liver. The depression of lipogenic factors such as PPARγ, ACC, and C/EBPa and expression of lipolysis proteins such as LPL, HSL, and AMPK supported the antiobesity effect of BBT, which was stronger than Orlistat, a drug that reduces TG levels to prevent obesity. 16 Considering the high decrease in body weight following the Orlistat treatment, the relative effects of BBT on lipogenesis and lipolysis that we observed were considerably higher than those exerted by Orlistat.
Compared to the in vivo animal study showing that BFM was reduced by dose-dependent BBT treatment (from 250 mg/kg to 1 g/kg) without hepatic toxicity, BBT (2.5 g/d, equal to 500 mg/kg in the mice study) was not sufficient to reduce total BFM in the human study. The ability of BBT to decrease levels of proinflammatory cytokines TNF-α and IL-6 more effectively and increase the production of anti-inflammatory cytokine IL-10 compared with Orlistat can otherwise explain the antiadipogenesis effects of BBT, but this particular significance was not demonstrated in the human study. Because of the limited dosage (<3 g/day) of the clinical study, total anthocyanin amounts (32 mg/day) in 2.5 g BBT were not sufficient to change the levels of proinflammatory cytokines in the blood of participants.
Despite the lack of difference in BFM and FFM as measured by DEXA between the BBT and control, BBT was observed to reduce WC and improve plasma lipid profiles in the subjects. The main reason why the first endpoints, reduction of BFM or weights, were not different between the BBT and control groups may be that our participants were obese instead of persons with normal BMI. Visceral fat, measured indirectly by WC or WHR, is metabolically and hormonally distinct from subcutaneous fat and is directly implicated in metabolic cardiovascular development with plasma lipids. 17,18 Visceral fat produces cytokines, TNF-α and IL-6, which stimulate forms of inflammation such as the hepatic production of C-reactive protein. 19 The reductions in the central fat accumulation caused by BBT, accompanied by lower TG, LDLc, and LDLc/HDLc ratios, were similar to those of other studies that showed a strong association between WC and TG or the TC/HDLc ratio. 20 A previous report suggests that some Asian populations, such as Filipino-American women, may be more likely to deposit central fat independently of BMI, thus placing them at higher risk of metabolic diseases. 21 Even though less is known about which is the stronger indicator of the risk factor for accumulation of abdominal fat, longitudinal changes in WC or current WC, we have supporting data for positive correlations between changes in WC and cholesterol intakes, and negative correlation between changes in BFM and fiber intakes. We suggested BBT may help decrease visceral fat and lower plasma lipids as long as high fiber and low cholesterol diets are sustained.
It has been reported that a diet containing C3G significantly reduces body fat accumulation in a 60% fat-DIO by activating the AMPK pathway in the white adipose tissue, skeletal muscle, and liver, and by decreasing the levels of TNF-α and ACC in epididymal fat. 15,16,22,23 Administration of 11 purified anthocyanins (320 mg/day) from bilberry and blackcurrant for 12 weeks improves endothelium-dependent vasodilation and lipid profiles in hypercholesterolemic participants with activation of the NO/cGMP signaling pathway. 24
Although less is known about the role of D3G in the reduction of body fat compared with that of C3G, we found that D3G concentration was higher than C3G in our anthocyanin-rich BBT, and D3G was more effective for reducing plasma lipids than C3G based on evidence from the 3T3L-1 in vitro study. Therefore, the ability of BBT to reduce plasma lipid profiles in humans may stem from D3G rather than C3G. As in our in vitro study, C3G improved insulin resistance, accompanied by GLUT4 translocation, adiponectin upregulation, and PPARγ activation, and suppression of LDL oxidation. 25
Our study had two main limitations. First, 8-week treatments were not a sufficient length of time to determine the effects of the supplement total body fat, despite the observation that short-term BBT supplementation significantly reduced abdominal fat. Second, measuring computed tomography would have been more accurate for testing WC than the DEXA method, which shows entire body fat distribution. However, taking a CT of every participant would not only be burdensome to them but would also render the trial research more difficult to generalize for larger populations in the future. Following the approved DEXA method is recommended for yielding optimal outcomes over a longer trial period.
In conclusion, we found that BBT had various causal effects on abdominal fat accumulation, lipolysis, and adipogenesis. With no difference between the two groups in energy-adjusted dietary intakes and physical activity, 8-week treatments of BBT (2.5 g/d) with high concentrations of anthocyanins (12.58 mg/g) were shown to strongly improve plasma lipid profiles, which were related to decreased abdominal fat as long as high dietary fiber and low cholesterol diets were maintained. In conclusion, BBT can potentially be developed as a functional food for preventing abdominal obesity with high fiber and low cholesterol diets. Although underlying mechanisms and related pathways remain unclear, BBT can be consumed as a nutrient-rich food and developed for preventing obesity in this age of cultural and industrial globalization.
Footnotes
Acknowledgments
This work was supported by the Cooperative Research Program for Agriculture, Science, and Technology Development (PJ907089), Republic of Korea. The authors thank the CRO, Healthcare, and Management, which assigned different staff in each investigation, handled all the data individually, and prevented any intervention from crossing over.
Author Disclosure Statement
No competing financial interests exist.