
Abstract
A double-blind crossover pilot trial tested the hypothesis that botanically derived calcium could demonstrate greater influence over calcium metabolism markers compared with a nonplant-derived calcium carbonate supplement or placebo. Twelve fasting female subjects received a single oral dose of Aquamin F™ (derived from the marine algal Lithothamnion sp.), or calcium carbonate, or placebo. Blood and urine samples were collected at baseline and over 12 h to evaluate ionized and total calcium and parathyroid hormone (PTH). Subjects treated with Aquamin F demonstrated significantly greater urinary clearance of calcium after 12 h compared with placebo (P = .004). Following a meal at 90 min, subjects treated with Aquamin F demonstrated a more prolonged suppression of serum PTH concentration (significantly lower than placebo at 90, 120, and 240 min). Calcium carbonate provided an intermediate response; urinary clearance was not significantly different from placebo treatment and PTH was only significantly lower than placebo at 90 min. Aquamin F may demonstrate greater influence over these markers of calcium metabolism than calcium carbonate or placebo, as suggested by a greater calciuric response and a more prolonged suppression of serum PTH concentrations following a meal in premenopausal women.
Introduction
O
Clinically useful calcium supplements must contain readily bioavailable calcium; however, bioavailability of different calcium supplements varies widely. 12,13 In addition, the percentage of calcium absorbed from a calcium preparation (i.e., the bioavailability) depends on the variable calcium absorptive capacity of the human subjects tested, 14,15 as well as the amount of calcium available for absorption in the calcium supplement. 9,16,17
Although natural plant sources of calcium are rare, the mineralized remains of the marine red algae, Lithothamnion sp., is known to contain large amounts of a highly porous and readily bioavailable calcium. The product from this seaweed species consists of mineral substances, particularly calcium carbonate (∼32% calcium by weight). The calcium carbonate found in Lithothamnion sp. is currently marketed and sold globally as a calcium supplement (Aquamin F™; Marigot Group Ltd., Cork, Ireland). Animal studies demonstrated the efficacy of Aquamin in positively influencing bone health in mice fed a high-fat western diet. 18 Furthermore, trials in human subjects have demonstrated Aquamin F supplementation in postmenopausal women may aid in maintaining bone density among osteopenic subjects when coadministered with a short-chain fructooligosaccharide 19 and can affect markers of calcium metabolism (including parathyroid hormone [PTH]) during exercise in both young males and in postmenopausal women. 20,21
Measuring the systemic absorption of an oral calcium supplement is made difficult because calcium is a normal and dynamic constituent of the extracellular milieu. Increased calcium absorption is expected to result in a measurable increase in urinary calcium secretion and additional markers, such as serum parathyroid (PTH) concentration, may help to verify increased calcium absorption. PTH levels decrease when subjects are supplemented with calcium. 20 –23 Elevated PTH concentrations have been reported in postmenopausal women; however, treatment with calcium reduced the PTH concentration to levels seen in premenopausal women. 24,25 In addition, consumption of a meal may impact serum PTH levels, but the magnitude and direction of this effect varies. 26,27
This study evaluated if botanically derived calcium had a greater influence over calcium metabolism markers compared with a nonplant-derived calcium carbonate supplement or placebo in premenopausal women.
Materials and Methods
Study treatments
The protocol was approved by the Quorum Review IRB (Seattle, WA, USA). The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Declaration of Helsinki 1975. Each subject was exposed to three treatments (placebo, calcium carbonate, or Aquamin F) separated by a 7-day wash-out period before the next treatment. Each subject was randomized to one of six possible treatment orders in double-blinded manner. To avoid any seasonal effects on calcium metabolism, all subjects completed the study within 4 weeks. For 1 week before each treatment period, subjects were maintained on calcium (400 mg/day) and sodium (100 mEq/day) restricted diets. On the day before the test, each subject fasted for 12 h and drank 600 mL of distilled water at 20:00 h and a further 300 mL and 23:00 h. On the morning of the test, subjects drank 600 mL of distilled water at 06:00 h and then 300 mL every 2 h during the remainder of the 12-h test period. Each subject received a standard calcium- and sodium-restricted meal at 90, 360, and 720 min after administration of the treatment dose. Each treatment dose included three, 2-piece gelatin capsules delivering 720 mg of elemental calcium (240 mg/capsule) from Aquamin F or calcium carbonate or placebo (all capsules provided by Marigot Group Ltd., Cork, Ireland).
Measurements
Blood samples were collected at 0 (before) and 0.25, 0.5, 1, 1.5, 2, 3, 4, 5, 6, 8, 10, and 12 h after administration of the treatment and were analyzed for ionized calcium, total calcium, and PTH levels. Urine was collected immediately before time 0 and during the entire 12-h test period. Total urine volumes produced during the test period were recorded and urinary calcium was measured. Measurements were performed in a single laboratory (Quest Diagnostics Laboratory, Minneapolis, MN, USA). Total urinary calcium excretion was calculated by multiplying the urinary calcium concentration (mg/dL) by the volume of urine collected. Urinary calcium excretion ratios were calculated for Aquamin F over placebo, calcium carbonate over placebo, and Aquamin F over calcium carbonate.
Statistical analysis
Baseline characteristics and primary outcome variables were compared using paired t-tests and repeated measures analysis of variance with Greenhouse–Geisser correction to analyze the three treatment conditions on any outcome variable. PTH reduction (relative to baseline) was compared between groups across all timepoints from 60 to 600 min using mixed-model regression. Statistical significance was established at P < .05. Classic pharmacokinetic techniques 28 were used to assess bioavailability. The pharmacokinetic parameters, time to maximum concentration (Tmax), elimination half-life (T½), maximal concentration (Cmax), and area over the curve were calculated using the linear trapezoidal rule.
Results
Study population and baseline measurements
Twelve healthy female volunteers gave their voluntary, written informed consent before participation in any trial activities and were enrolled in the study. The subjects were not using any mineral supplement or medication known to affect the metabolism of calcium. All 12 randomized subjects completed the trial with no missing data. The mean age was 28.8 years, mean body weight was 66.7 kg, and mean BMI was 25.5 kg/m2. No serious adverse events were reported in this trial.
Serum ionized and total calcium
Serum ionized and total calcium concentrations were relatively unchanged over the duration of the12-h study period. The ionized calcium concentrations were ∼5 mg/dL and the total calcium concentrations were ∼9 mg/dL during each of the three treatment periods. Estimates of Tmax and T½ were not possible because of the flat pharmacokinetic profiles and no estimates of AUC to infinity could be calculated. No significant differences were found between any of the treatment groups for ionized or total serum calcium concentrations.
Urinary calcium excretion
In contrast to the relatively unchanged serum calcium values, treatment with Aquamin F resulted in a significantly greater urinary calcium concentration and total amount of calcium excreted than placebo (P = .004, and P = .006, respectively) (Table 1). In contrast, the urinary calcium concentration and total calcium excretion amounts during the calcium carbonate treatment were not significantly different than placebo (P = .36 and P = .95, respectively) (Table 1).
Serum PTH
A main effect of treatment across all timepoints from 60 to 600 min was significant (P = .04) and treatment by time interaction approached statistical significance (P = .055). Post hoc matched-pair comparisons at each timepoint revealed significant group differences at 90, 120, and 240 min between Aquamin treatment and placebo and at 90 min between calcium treatment and placebo. Table 2 shows the effect of treatment on serum PTH concentration and Figure 1 shows the percent change in PTH level relative to baseline (time 0) to observe the relative changes in concentration. Relative to time 0, the serum PTH concentrations for all treatments decreased during the first 60 min after dosing. At 90 min, immediately before consumption of the meal, the serum PTH concentration for the placebo treatment increased back to baseline levels and then decreased with further sampling before returning to baseline levels again at 360 min. In contrast to the changes in serum PTH seen with placebo, the serum PTH concentration after the Aquamin F treatment continued to decrease after 60 min and remained significantly lower than the PTH concentration for placebo at 90, 120, and 240 min (P = .003, .017, and .030, respectively). The serum PTH concentration after the calcium carbonate treatment was intermediate between the Aquamin F and the placebo treatment responses, being significantly decreased at 90 min only compared with placebo (P = .026). All treatments resulted in similar PTH responses after 300 min and returned to baseline levels at 360 min after dosing, immediately before the next meal (Fig. 1).
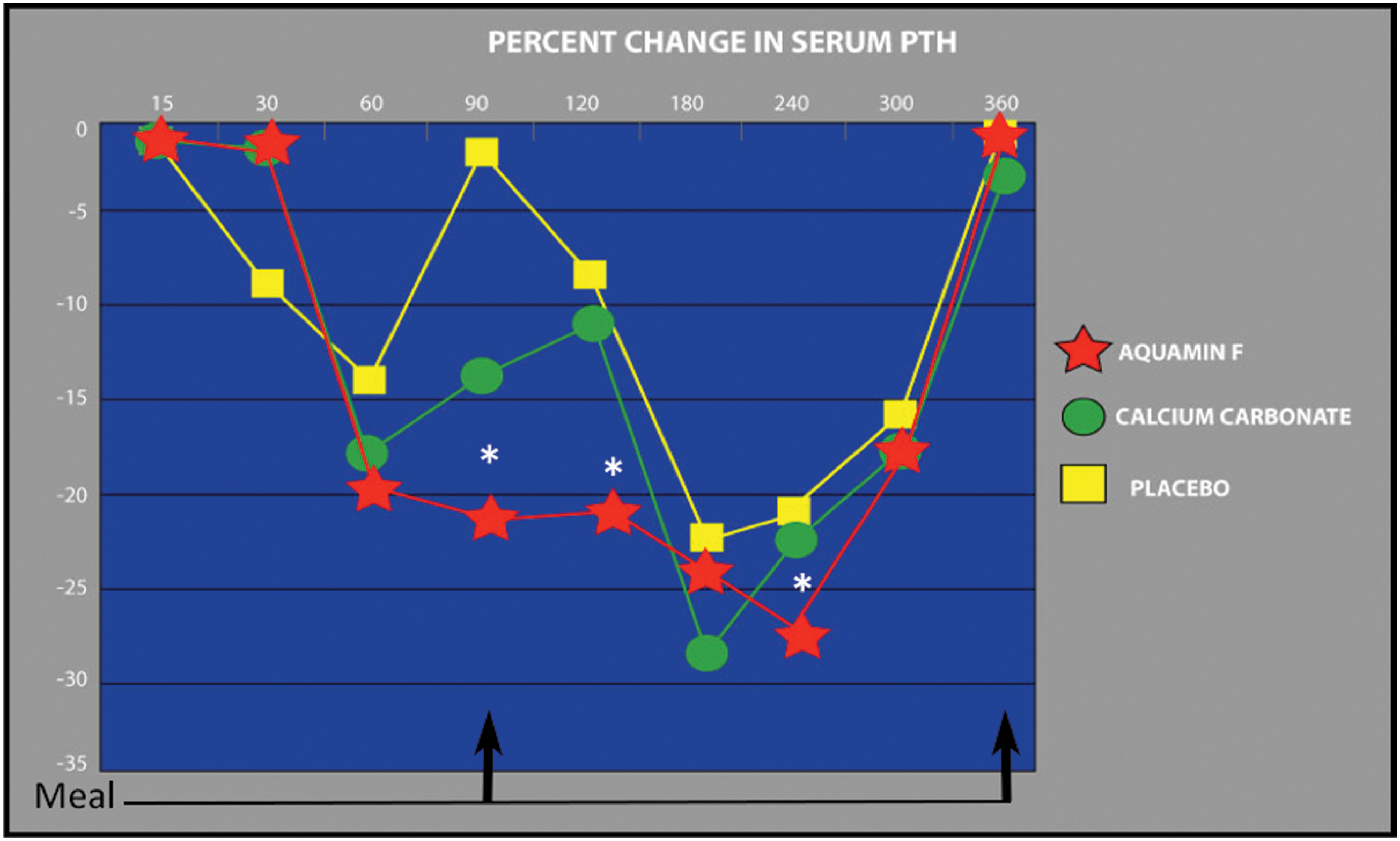
Percent change in serum PTH levels over time. *Compared with placebo, the decrease in PTH concentration following Aquamin F™ treatment was significant at 90, 120, and 240 min (P = .003, P = .017, and P = .030, respectively) while calcium carbonate treatment was significantly different from placebo treatment only at 90 min (P = .026). Arrows indicate the timing of meals. PTH, parathyroid hormone. Color images available online at
Discussion
The number of osteoporosis-related primary care physician and specialty physician visits has increased more than fourfold from 1.3 million in 1994 to 6.3 million visits in 2003. 29 In addition, a cross-sectional analysis of 9 million osteoporosis patient visits showed a similar fourfold increase in osteoporosis-related visits from 5% in 2002 to 20% in 2008, 30 while undertreatment was noted, particularly among elderly patients residing in institutional settings. 29 –32 Increased calcium intake has been associated with a reduction in the risk of bone fracture 33,34 and osteoporosis prevention begins with the development of optimal levels of peak bone mass as early as 6–10 years of age and certainly during the second decade of life. 5 Regular exercise and a healthy diet with enough calcium helps young adults maintain good bone health and may reduce their risk of osteoporosis later in life.
This study enrolled young, premenopausal women to study a period of relative bone stability compared with adolescent or postmenopausal women. The pharmacokinetic and pharmacodynamics responses to a form of calcium derived from a mineralized seaweed (Lithothamnion sp.; Aquamin F) compared with calcium carbonate or placebo.
The amount of calcium excreted in the urine during active calcium treatments (Aquamin F and calcium carbonate) was 50–60% higher than during placebo treatment. The calcium excreted in the urine during the Aquamin F treatment was 6% higher than the calciuric response during the calcium carbonate treatment. The crossover nature of the trial design allowed determination of each individual's response to each treatment and revealed a significant increase in calcium excretion from the Aquamin F treatment compared with placebo (P = .004 and P = .006 respectively) (Table 1). This was not observed with the calcium carbonate treatment.
Previous research demonstrated a decline in serum PTH levels in response to an increase in serum calcium from oral calcium supplements. 24 In this study, Aquamin F treatment significantly decreased PTH concentrations compared with placebo at 90, 120, and 240 min (P = .003, P = .017, and P = .030, respectively) while calcium carbonate treatment significantly decreased PTH concentration compared with placebo only at 90 min (.026). PTH concentrations are highly sensitive to the consumption of a meal. 26,27 A prior study showed ingestion of a gastric acid-stimulating test meal resulted in increased serum PTH in normal subjects, and ingestion of antacid with the test meal prevented an increase in serum PTH concentration. 26 The greater effectiveness in suppressing PTH concentration shown by Aquamin F compared with calcium carbonate may be a feature of its antacid qualities, or its calcium load, or a combination of both. Another study showed an increase in calcium excretion following the consumption of a high protein meal, without changes in serum PTH concentration. 35 This may be a consequence of the experimental design as the time of sampling started with consumption of the meal. Changes in PTH may occur in anticipation of a meal as well as being a consequence of its consumption. 26
This study examined the absorption, PTH response, and renal excretion of calcium in premenopausal women treated with Aquamin F, calcium carbonate, and placebo. Calcium from Lithothamnion sp. has a highly porous structure, resulting in substantially greater surface area per particle compared with calcium carbonate from other sources (Marigot Ltd., unpublished data). The results of this pilot study suggest Aquamin F is more biofunctional for impacting bone metabolism than a traditional calcium supplement, even though both contain calcium carbonate. Oral administration of Aquamin F in premenopausal women had a greater calciuric response and a more profound pharmacodynamic response resulting in a prolonged suppression of serum PTH concentrations following a meal when compared with similar treatments with calcium carbonate or placebo.
This study indicates that the response is not linear across all timepoints and is highly variable. For these reasons, we chose a time 60 min just before meal consumption at 90 min to measure the response in a repeated measures analysis. Subsequent studies are needed to evaluate the implications of this research, the impact of vitamin D on the absorption of Aquamin F, and to further evaluate the effects of Aquamin F on markers of bone metabolism in older, postmenopausal women as have been recently described. 19 Although additional studies are needed, this study suggests Aquamin F, a calcium supplement derived from the marine red algae Lithothamnion sp., may represent an effective means of providing calcium supplementation to individuals at risk of bone loss due to osteoporosis.
Footnotes
Acknowledgment
The authors thank Dr. Ronald Sawchuk for the pharmacokinetic and pharmacodynamics analyses.
Author Disclosure Statement
No competing financial interests exist.