
Abstract
The effect of GINST15, an enzyme fermented ginseng supplement, on hormonal and inflammatory responses to physical stress in humans is unknown. The purpose of this investigation was to examine the constitutive and stress-induced effects of GINST15 supplement on hypo-pituitary-adrenal (HPA) and antioxidant activity in addition to muscle damage. Ten women (age: 38.7 ± 7.8 years; height: 163.81 ± 4.4 cm; body mass 76.0 ± 11.6 kg) and nine men (age: 41.2. ± 9.7 years; height: 177.4 ± 5.3 cm; body mass: 88.5 ± 5.0 kg) participated in a double-blinded, placebo-controlled, counterbalanced within-group study. Participants completed three 14-day treatment cycles with different doses (high: 960 mg; low: 160 mg; placebo: 0 mg) separated by a 1-week washout period. At the end of treatment, physical stress was imposed with intense resistance exercise work stress. Participants provided blood at rest and various time points after exercise (immediately [IP], 30 min [30], 60 min [60], 24 h [+24HR]). Cortisol (CORT), superoxide dismutase (SOD), total glutathione, nonspecific antioxidant activity, total antioxidant power (TAP), and creatine kinase were measured. GINST15 supplementation produced stress-inducible dose-dependent reductions in circulating cortisol and increased enzymatic and nonspecific antioxidant activity. Twenty-four hours after intense exercise, a high dose GINST15, a bioactive ginsenoside metabolite, significantly reduces muscle damage and HPA responses to physical stress in humans; these effects may result from increased antioxidant expression.
Introduction
G
Ginseng is composed of many substances (see Refs. 2,21 ), but the primary bioactive constituents are saponins (ginsenosides), which number in the hundreds. 22 These triterpene glycosides share the following properties: (1) a steroid-like four-ring structure; (2) mono-, di-, or trimeric sugar molecules; and (3) two or more free or sugar-bound hydroxyl groups. 23 In addition to the presence of stereoisomers, these variable properties likely explain the wide range of effects observed in cell lines and animal models. 3,4,7,15,23 –26
Ginsenosides display low bioavailability in their unmodified form. Rather than being directly absorbed, major ginsenosides are hydrolyzed by intestinal bacteria into bioactive metabolites. 27 –31 However, a large proportion of the population may lack the requisite microbial profile. 24,32 Modern industrial processes have overcome this limitation by mimicking the actions of gut bacteria with recombinant enzymes. 24,31,33,34
A prominent example is GINST15 (20-O-β-D-glucopyranosyl-20(S)-protopanaxadiol; or Compound K), the major metabolite of ginsenosides Rb1, Rb2, and Rc. 22,24,29 –31 Because of its relative nonpolarity, GINST15 is readily absorbed into circulation (bioavailability ≅35% at 20 mg/kg). 34,35 Correspondingly, GINST15 has generated intense interest as a therapeutic modality, with demonstrated efficacy in various animal models of neurological 1,2,11,12,15,36,37 and metabolic disease, 4 in addition to cancer. 5,6
Despite varying etiologies, the conditions ginsenosides are used to treat share the common properties of pathological oxidative stress, inflammation, and aberrant neuroimmune function. 2,25 As a physical stressor, exercise transiently induces neuroimmune activity, oxidation, inflammation, and muscle damage (for a review, see Ref. 38 ). Accordingly, exercise has been used to study the effects of ginsenosides on immune, 20,21,39,40 skeletal muscle, 18 –20,41,42 hepatic, 41,43,44 and psychological function. 8,13
These investigations consistently report reductions in exercise-induced oxidative damage and inflammation in conjunction with increased enzymatic antioxidant activity. Nevertheless, use of high doses in animal and cell-based models may constrain translational impact in humans. It is also important to consider potential differences in stress responses of voluntarily exercising humans compared to those of animals under forced exercise.
Our understanding of the effects of GINST15 on its purported targets in humans is in its infancy, with a paucity of research using exercise. Nonprocessed ginseng extracts have largely failed to produce significant treatment effects, 9,45 –49 likely reflecting a combination of low doses, low bioavailability, and insufficient treatment period durations. Higher doses (6 g/day) reduce oxidative damage and increase antioxidant content, but treatment-related differences in time to exhaustion (exercise workloads) limit the interpretability of these findings. 50 Reductions in muscle damage have been observed without differences in time to exhaustion, but antioxidant activity was not examined. 51
Given its demonstrated efficacy in exercising animals, 16 –18,44,52 GINST15 may confer protection against exercise-induced stress in humans, as reflected in circulating measurements of antioxidants, neuroendocrine activity, and muscle damage. The purpose of this investigation was to examine the constitutive and stress-induced effects of GINST15 supplement on neuroendocrine hypo-pituitary-adrenal (HPA) and antioxidant activity in addition to muscle damage.
Materials and Methods
Experimental approach
A double-blinded, placebo-controlled, counter-balanced within-group study design was used. To examine the dose-dependent effects of GINST15 on oxidative and HPA activity in humans, we measured various circulating biomarkers after 14 days of treatment with a high dose (HIGH: 960 mg), low dose (LOW: 160 mg), or placebo (CON: 0 mg). Blood was collected at rest before the exercise resistance stress (RE), immediately after exercise (IP), at 30 and 60 min postexercise, and again 24 h after the exercise test. Each treatment cycle was separated by a 1-week washout period. Participants were familiarized with the experimental procedures during an initial baseline testing visit.
Participants
Ten healthy women (age: 38.7 ± 7.8 years; height: 163.81 ± 4.4 cm; body mass: 76.0 ± 11.6 kg) and nine men (age: 41.2. ± 9.7 years; height: 177.4 ± 5.3 cm; body mass: 88.5 ± 5.0 kg) volunteered to participate in the study. The exclusion criteria were as follows: failure to confirm medical clearance for participation in intense exercise; ongoing consumption of any ginseng-containing product; food or supplement allergies; hypersensitivity to caffeine; musculoskeletal injuries or physical limitations affecting the ability to exercise; current use of any hormonal substance, including testosterone, anabolic steroids, or growth hormones; ongoing use of any anti-inflammatory medications; diagnosis of diabetes, hypertension, or cardiovascular disease; use of cholesterol or blood pressure–lowering medications; the use of tobacco products; and alcohol consumption in excess of three drinks per day or 18 per week. Each participant was healthy and active with recreational activities (e.g., walking and so on), but not participating in any structured or organized training programs week to week. All subjects provided written informed consent for inclusion before they participated in the study. The study was approved by the Ohio State University Biomedical Sciences Institutional Review Board (2014H0404).
GINST15 treatment
During each 14-day treatment cycle, participants consumed 960 mg (high dose), 160 mg (low dose), or placebo (CON) using identical liquid capsule preparations (GINST15®; ILHWA Co. LTD., South Korea) (Table 1). Treatment allocation was counterbalanced and double blinded. Each daily dose of six capsules was split into the AM and PM compartments of a 7-day pill box. Participants were instructed to consume three capsules in the morning and evening. For Low dose, an active (160 mg) capsule was placed into the AM compartment; the remaining five capsules were placebo. Participants were reminded of their supplement schedule and each participant kept a supplement log and returned that document along with the empty pill box. Participants followed the same schedule on the day of RE stress test visit and also for the 24 h recovery visit, with the exception that the first three capsules were ingested immediately after the resting blood draw during each RE visit.
During each 2-week treatment period, participants consumed 960 mg (high dose GINST15), 160 mg (low dose GINST15), or no hydrolyzed ginseng extract using identical liquid capsule preparations (CON, placebo condition).
Resistance exercise work stress and recovery visits
After 14 days of supplementation, participants reported to the laboratory to provide blood samples and complete an intense resistance exercise work stress (RE). The tests were performed in a fasted state at a standardized time in the morning. Women were tested during days 1–8 of the follicular phase. The intense exercise work stress consisted of using a leg press (Plyo Press; Athletic Republic, Park City, UT, USA), for 5 sets of 12 repetitions at 70% of 1 repetition maximum (RM) (obtained during baseline visit), with 2 min rest between sets. The 1 RM test was performed using similar methods common in our laboratory. 53,54 In brief, dynamic stretches were performed and then warm-up sets of about 5–10 repetitions were done at 50% and 70% of estimated 1 RM followed by 1 RM attempt with no more than 5 attempts to lift the heaviest weight possible. About a minute of rest was used between single attempts if the subject was ready. To facilitate comparison of resistance exercise stress test responses, the total work performed in the resistance exercise stress test protocol was kept the same for each of the three testing cycles based on the percent of the 1 RM calculation. Twenty-four hours after the RE stress test visit, participants provided a resting blood sample. Baseline testing for scale ratings of mood disturbances, sleep quality, and perceived muscle soreness was obtained before starting a study supplement protocol sequence and again after the resistance exercise stress test, as well as at the 24 h recovery time point. At the conclusion of 24 h recovery testing visit, participants began a 1-week washout period, followed by the initiation of the next 14-day treatment cycle.
Blood collection and analysis
At the beginning of RE and 24 h recovery test visits, a resting blood sample was collected using an indwelling Teflon cannula inserted into a superficial antecubital vein and kept patent with an isotonic saline solution. After cannula insertion, participants sat for 15 min before the first blood draw (REST) to allow for equilibration. To avoid dilution of the sample, 3 mL of waste was drawn from the cannula and discarded before each blood draw. A 4 mL sample was obtained using a Vacutainer apparatus and collection tubes containing buffered sodium citrate or sodium heparin.
Serum blood samples were left at room temperature for 30 min to coagulate. Tubes were centrifuged at 3000 g for 12 min at 4°C. Citrate and Heparin samples were kept on ice until processing. Citrate samples were centrifuged at 3000 g for 12 min at 4°C. For the analysis of total glutathione (tGSH), 500 μL plasma was removed from the heparin tube and split into two 250 μL samples. Thousand microliters ice-cold 5% metaphosphoric acid was added to each 250 μL sample, which was then vortexed and centrifuged at 13,000 g for 2 min at 4°C. The resulting deproteinated heparin supernatant, citrate plasma, and serum samples were stored at −80°C until biochemical analysis.
For biochemical analysis, samples were thawed once and analyzed in duplicate at the recommended absorbances (Synergy H1 plate reader; BioTek, Inc., Winooski, VT, USA). Each analyte was assayed as per manufacturer recommendations. Serum cortisol (CORT) was measured by enzyme-linked immunosorbent assay (ELISA) using an end-point assay at 450 nm (#CO103S; Calbiotech, Spring Valley, CA, USA). Inter-and intra-assay variances were ≤6%. Serum creatine kinase (CK) was measured at a 1:35 sample to reagent ratio with a kinetic assay at 340 nm (#326-10; Sekisui Diagnostics, Lexington, MA, USA). Inter- and intra-assay variances were ≤8%.
Plasma superoxide dismutase (SOD) enzyme activity was measured using the cytochrome c reduction method, implemented with a hematoxylin autoxidation rate assay (#NWK-SOD02; Northwest Life Science Specialties, Vancouver, WA, USA). Inter- and intra-assay variances were ≤11%. The test involved a 10-min kinetic absorbance reading at 560 nm; samples were undiluted. After 1:40 dilution, plasma total antioxidant power (TAP) was measured using a copper reduction assay (TA02; Oxford Biomedical, Oxford, MI, USA). End-point mode detection was accomplished at 450 nm. For tGSH, deproteinated citrate samples were diluted 1:20 with assay buffer and analyzed using a kinetic enzymatic recycling assay (#GT20; Oxford Biomedical). The colorimetric reaction was monitored in 1 min intervals over a 10-min period at 405 nm. Inter- and intra-assay variances were ≤10%.
Experimental controls
At the beginning of each RE stress test and +24HR visit, participants completed surveys for sleep quality, 55 mood state, 56 muscle pain and soreness, 57 and life stress. 58 Euhydration was confirmed using urine refractometry (USG ≤1.025). When necessary, participants were given water and retested until the cutoff was met. To eliminate diurnal and dietary effects on target biomarkers, participants were tested in a fasted state (≥8 h) at a standardized time of the day (±2 h). Participants were also asked to log their diets during the initial 14-day treatment period (in addition to RE stress test and 24 h recovery visit days), with replication during each of the two remaining treatment cycles.
To ensure the accuracy and completeness of diet records, participants were counseled and given specific instructions for recording their diets. Participants were asked to refrain from ingesting any additional ginseng-containing products during the study. In addition, participants were asked to refrain from any physical exercise 72 h before RE stress test until the completion of the subsequent +24HR visit. After the RE stress test, participants were asked to refrain from the use of any external or supplemental recovery drug, supplement, device, or any other recovery modalities.
Statistical analysis
Data are presented as mean and standard deviation. nQuery Advisor® software (Statistical Solutions, Saugus, MA, USA) was used to determine that a group size of n = 20 (10 men and 10 women) would be adequate to defend the 0.05 alpha level of significance with a Cohen probability level of at least 0.80. Data analysis was performed using SPSS (Version 24; IBM, Inc., Armonk, NY, USA). Assumptions for linear statistics were generally met, and when kurtosis or skewness was significantly greater than zero, data were reanalyzed after log10 transformation. If a similar outcome was found, the analysis on transformed data was disregarded. When Levene's test for equality of variance did not allow for the assumption of equal variance, analyses were conducted on adjusted data (using Levene's adjustment procedure).
Independent T-tests were used to compare men and women subject characteristics. For each of the other dependent variable, we used two-way analysis of variance with repeated measures, (2 sex × 2 treatment × 2 or 5 time points) When significant main effects or interactions were demonstrated post hoc analyses for pairwise comparisons utilized subsequent Fisher LSD post hoc analyses. Significance in this investigation was set at P ≤ .05.
Results
For cortisol there was a main effect for treatment, time, and sex with interaction effects being significant for time and sex. In the both GINST15 supplementation treatment groups, neither dose had any effect on resting serum cortisol (Fig. 1A, C). Pairwise post hoc comparisons showed that in men, resistance exercise resulted in significant HPA activation in the CON treatment condition, reflected by significantly elevated circulating cortisol up to 1 h after the exercise stress. Again, pairwise comparisons showed that high dose GINST15 treatment resulted in significant suppression of the stress response compared to CON and low dose GINST15 treatment. Again, similar to the men, in women, resistance exercise stress in the CON condition increased cortisol concentrations up to 30 min postexercise. Interestingly, in general the low and the high dose supplementation resulted in significant cortisol attenuation compared to CON for up to 60 min into recovery. Twenty-four hours after exercise, cortisol values had returned to pre-exercise levels and did not differ by sex. The main effect for treatment-time-sex interactions showed with pairwise comparisons that women had higher resting cortisol concentrations compared to men but were lower during postexercise at each time point for the CON conditions. Women also had lower values for the low dose than men. Similar values were seen for the high dose GINST15 for both men and women.
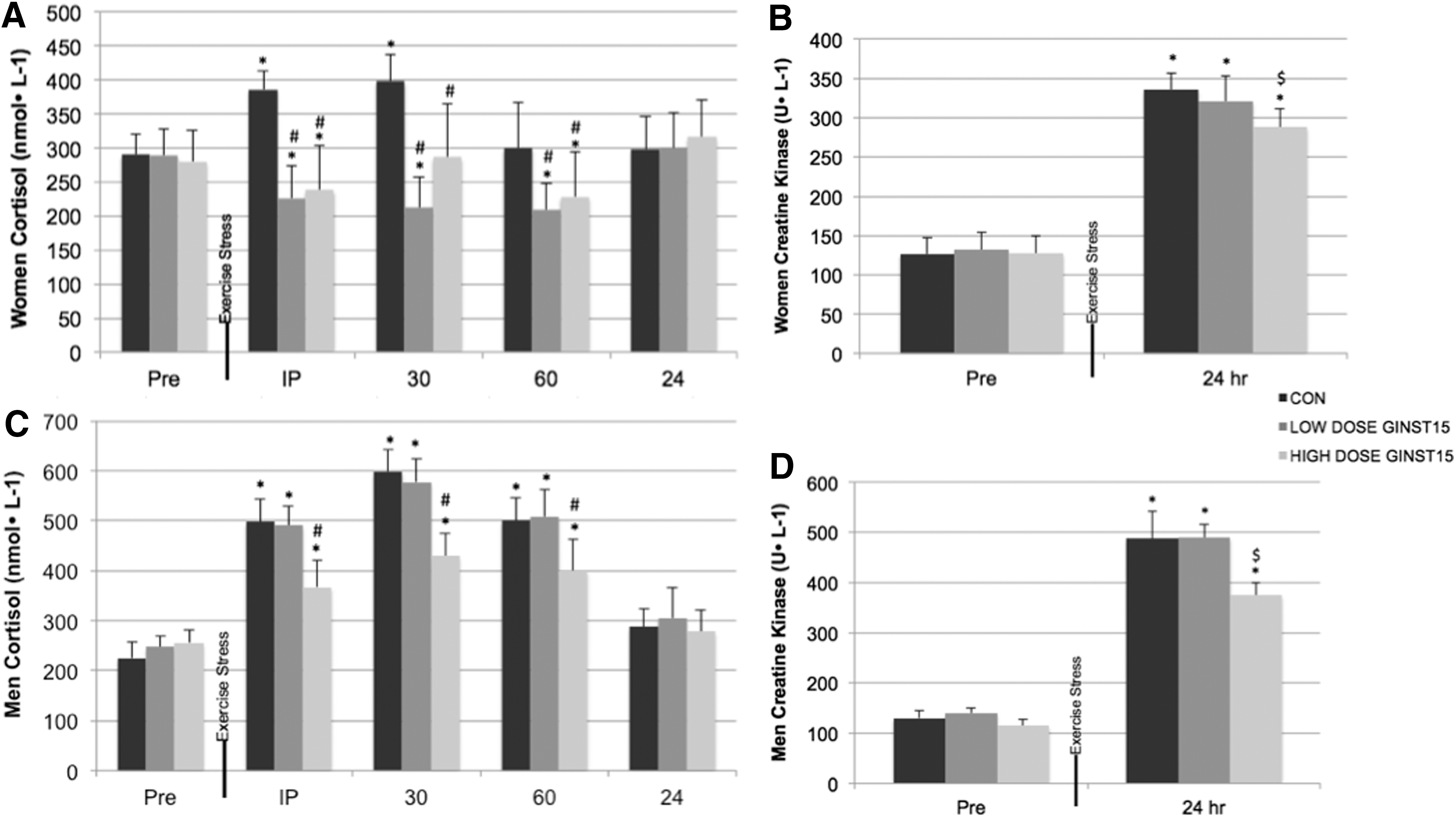
Serum cortisol and CK by time point, sex, and treatment condition.
For CK, an indirect measure of muscle damage, significant main effects for treatment, time, and sex were observed. Expected increases in response to exercise under all treatment conditions were observed for both men and women (Fig. 1B, D). Pairwise post hoc comparisons showed that the high dose GINST15 had significantly lower response to the exercise stress compared to the CON condition or low dose GINST15. The interaction effects for sex showed with pairwise comparisons that men had significantly higher values in recovery than women at all of the time points and this was expected due to the greater muscle mass to perform in the resistance exercise stress test.
In Table 2 a main effect for treatment and time was observed with interactions for supplement and time. Post hoc analyses showed that the values for tGSH were significantly increased only in the high dose GINST15 treatment above rest immediately after exercise and at both 30 and 60 min postexercise stress. In addition the high dose GINST15 values were also significantly higher than the corresponding values at these same time points.
P ≤ .05 from corresponding rest time point.
P ≤ .05 from corresponding CON and low dose treatments.
In Table 3, SOD showed main and interaction effects for treatment and time. As shown in Table 3, all of the treatments demonstrated significant increases from resting values with the high dose GINST15 demonstrating significantly higher values than that other two groups at immediate and 30 min postexercise stress. No differences between men and women were observed.
P ≤ .05 from corresponding rest time point.
P ≤ .05 from corresponding CON and low dose GINST15 treatments.
In Table 4 the TAP values demonstrated main effects for treatment and time with interactions between treatment and time. Significant increases were observed for both men and women immediately postexercise stress and remained elevated at 30 and 60 min into recovery for the high dose GINST15 treatment. Post hoc analyses showed that the high dose GINST15 treatment was significantly higher than the other two treatment conditions. Again, no sex-linked differences were observed.
P < .05 from corresponding rest time point.
P < .05 from corresponding CON and low dose GINST15 treatments.
In Table 5 mood state changes are presented with no statistical main effects or interactions observed. No significant differences between sexes or with any of the treatment conditions were observed for mood disturbances before and following the resistance exercise stress test. Similarly in Table 6 no statistical main or interaction effects were observed for sleep disturbances and muscle soreness perceptual ratings; again no differences were observed for men or women or for any treatment condition (Table 6).
The higher the number the more mood disturbance is reflected. The values (mean ± SD) for the baseline, performance, and recovery of the women (n = 10; A) and men (n = 9; B) for each supplement. Baseline for women was −2.8 ± 8.1 and for men was −1.9 ± 3.6.
Women, n = 10; men, n = 9.
R, recovery time point after 24 h of recovery after resistance exercise stress test; stress, resistance exercise stress test.
Discussion
In this study we were very interested in whether or not such a bioactive ginsenoside metabolite could exert dose-dependent effects on HPA activity, antioxidant activity, and inflammation at rest and in response to physical work stress in humans. We used an intense resistance exercise stressor to induce HPA activation while causing muscle tissue damage. The primary findings of this investigation are that GINST15 produces a dose-dependent inhibitory effect on HPA activity and muscle damage after exercise, which appears to reflect increased antioxidant activity. Resting biomarker concentrations were not altered by the supplement, and values returned to pre-exercise stress values within 24 h after exercise. This suggests that the supplement, most notably the high dose GINST15, primarily affects the stress response.
Animal models have revealed the ability of ginsenosides to reduce circulating corticosterone in response to weight-loaded swimming, 13 acute stress, 59 and chronic mild stress. 10 Paradoxically, ginsenosides also activate the HPA axis, with the caveat that this is observed in an unstressed state at the initial stages of treatment. 60 Reductions in circulating HPA markers of stress such as cortisol may reflect the increased neuronal nitric oxide (NO) signaling through increased nitric oxide synthase (NOS) activity. 59 Interestingly, ginsenosides may act as partial agonists for glucocorticoid receptors, 61 raising the possibility that ginsenosides reduce glucocorticoid synthesis through endogenous HPA axis feedback loops.
In rats and mice, ginsenoside supplementation reduced exercise-induced muscle damage (CK) and lipid/protein oxidation (thiobarbituric acid reactive substances, malondialdehyde [MDA], protein carbonyls), while increasing citrate synthase, GPX, and SOD. 18,41,43 The effects were dose dependent. Others have demonstrated reduced oxidative activity and muscle damage with variable changes in antioxidant activity in response to exercise. 19,42,44 Accordingly, reductions in oxidative muscle damage could reflect the inhibition of iNOS. 62
Alternatively, ginsenosides may interact directly with hydroxyl radicals while activating genetic binding sites for transcription factors (e.g., specific-1 [Sp1], activator protein 2 [AP-2], and early growth response 1 [Egr-1]) on the gene as promoters of SOD. 63 Nevertheless, the dose-dependent relationship observed in this study supports our contention that intense exercise caused oxidative damage to muscle and that treatment-related reductions in muscle damage were the result of increased antioxidant activity. However, the changes in muscle damage were not consciously perceived to be different across treatment conditions.
In a prior study in men, 4 weeks of supplementation at 1600 mg/day of American ginseng (i.e., AG, Panax quinquefolium) led to reduced CK and lactate in response to an exhaustive running protocol (80% VO2 max). 51 Time to exhaustion in this study did not differ, suggesting that (1) the benefits of ginsenosides are adaptogenic, not ergogenic and (2) increased antioxidant expression is not a simple reflection of greater oxidative stress because of higher absolute workloads. Our observations in the current study are also in agreement with another prior report in men, where 6 g/day supplementation of P. ginseng extract resulted in reduced oxidative damage (using MDA) and increased enzymatic antioxidant activity (using catalase and SOD). 50
Our findings of reduced muscle tissue damage may reflect a number of different mechanisms that may be integrated in their involvement and be a topic of further research. We know that ginsenosides can increase the expression of pro-inflammatory cytokines through effects on toll-like receptor (TLR4) expression in macrophages. 39 Ginsenoside treatment increased NF-κβ, IL-6, e/iNOS, TNFα, and GPX in muscle without any sign of increased oxidative damage, necrosis, or M1 macrophage infiltration at rest. After exercise, reduced muscle necrosis, M1 infiltration, e/iNOS synthesis, and cytokine release were observed; IL-10, SOD, and M2 macrophage content increased. 17,20,64 Reductions in COX-2 and iNOS mRNA or TNFα may explain decreases in NF-κβ activation. 15,16,37
Further examination revealed that GINST15 does not act directly on TLR4, but stabilized interleukin-1 receptor-associated kinase-1, a downstream kinase, prevented its phosphorylation and the subsequent activation of NF-κβ. 16 These observations support the theory that ginsenosides induce protective inflammation (i.e., euflammation), 65,66 with initial low-level inflammation promoting moderate responses to subsequent stressors. The inflammatory response to exercise and the role of GINST15 remain a fertile area for future study as the basis for it has been set up in this study. Euflammation is also consistent with the expression of antioxidants. 1
If GINST15 promotes the generation of NO at the early stages of treatment, this would increase endogenous antioxidant expression through Nrf2 activation of antioxidant response elements. 1,7,67 The antioxidant changes in this study reflect this more basic set of mechanisms to be potentially operational. Mechanistically, euflammation could be promoted by any combination of the following: (1) increased NOS synthesis; (2) inflammatory cytokine secretion; (3) partial agonist effects on glucocorticoid receptors; (4) reduced TLR4 sensitivity to endogenous ligands; (5) and immunophenotypic shifts to an M2 state. 39,59 –61
As steroid glycosides, it is important to consider the possibility of harmful off-target effects, especially at high doses. This includes potential agonistic effects on various steroid receptors and saponin-induced modulation of cell membrane structure and permeability. In rats, the safe upper dose limit of ginsenosides is as high as 2000 mg/(kgċday) of Korean red ginseng extract, 68 corresponding to over 150,000 mg/day in our subject population (dosing ranging from ∼9 to 15 mg/kg). This also compares favorability to doses used in the aforementioned animal models, which averaged ∼20–120 mg/kg. Thus, the importance of bioavailability as an experimental consideration may be warranted.
In summary, this study was one of the first to provide insights into the influence of a ginseng supplement on work stress-induced responses in middle-aged men and women. The HPA activity with GINST15 supplementation is reduced and potentially helps to mediate, in part, less catabolic activity in muscle. The antioxidant activity with GINST15 supplementation at the high dose GINST15 is reflected during the acute recovery phase over 60 min after exercise. In combination these responses appear to result in lower muscle tissue disruption. Interestingly, mood state, sleep, and soreness ratings are not appreciably impacted although a great deal of variance exits. Such data may also be relevant resilience and recovery interventions for physical work in middle-aged men and women. Finally, this study provides some initial novel data for subsequent studies to build on from both performance outcomes and other cellular mediating mechanisms in future study designs.
Footnotes
Acknowledgment
Funding for this study and the costs to publish in open access was provided by ILHWA Co. LTD, South Korea.
Author Disclosure Statement
No competing financial interests or conflicts of interest exist for this study.