
Abstract
Inflammatory bowel diseases (IBDs) are mainly represented by ulcerative colitis and Crohn's disease, and the increase in the incidence tends to follow the rapid industrialization and lifestyle of modern societies. FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) consist of molecules that are poorly absorbed in the small intestine and are fermented by bacteria in the colon leading to symptoms such as bloating, flatulence, diarrhea, and abdominal pain. Reduction of the ingestion of FODMAP could reduce the symptoms and improve the quality of life. This review aimed to summarize some important aspects of IBD and evaluate the effects of this diet on this inflammatory condition. Studies including the term FODMAP (and similar terms) and IBD were selected for this review (MEDLINE database was used PubMed/PMC). A low FODMAP diet may be an effective tool to the management of the common abdominal symptoms in patients with functional gastrointestinal symptoms once these molecules trigger these symptoms. This diet may also reduce the expression of pro-inflammatory markers such as C-reactive protein and fecal calprotectin and may interfere with the microbiome and its metabolites. The use of a low FODMAP diet can bring benefits to the IBD patients, but may also modify their nutritional status. Thus it should be utilized in appropriated conditions, and dietary supplements should be necessary to avoid deficiencies that could be caused by a low FODMAP diet over long periods. We suggest that further investigations are required to elucidate when and how to apply the FODMAP diet in IBD patients.
Introduction
T
IBD is mainly represented by ulcerative colitis (UC) and Crohn's disease (CD) that share similar triggering factors and differ in the incidence, the pattern of inflammation, and affected areas as seen in Figure 1. The increase in the frequency of this pathology tends to follow the rapid industrialization and lifestyle of modern societies. The highest rates are observed in North America and Western and Northern Europe, and the lowest rates are found in the Southern. Nearly 1 in 198 persons present UC, and 1 in 310 persons present CD. The prevalence of UC seems to be higher in men and CD in women. IBD patients normally present gastrointestinal symptoms that are related to the reduction of quality of life (QoL), and the diet may influence this panorama. 3 –6
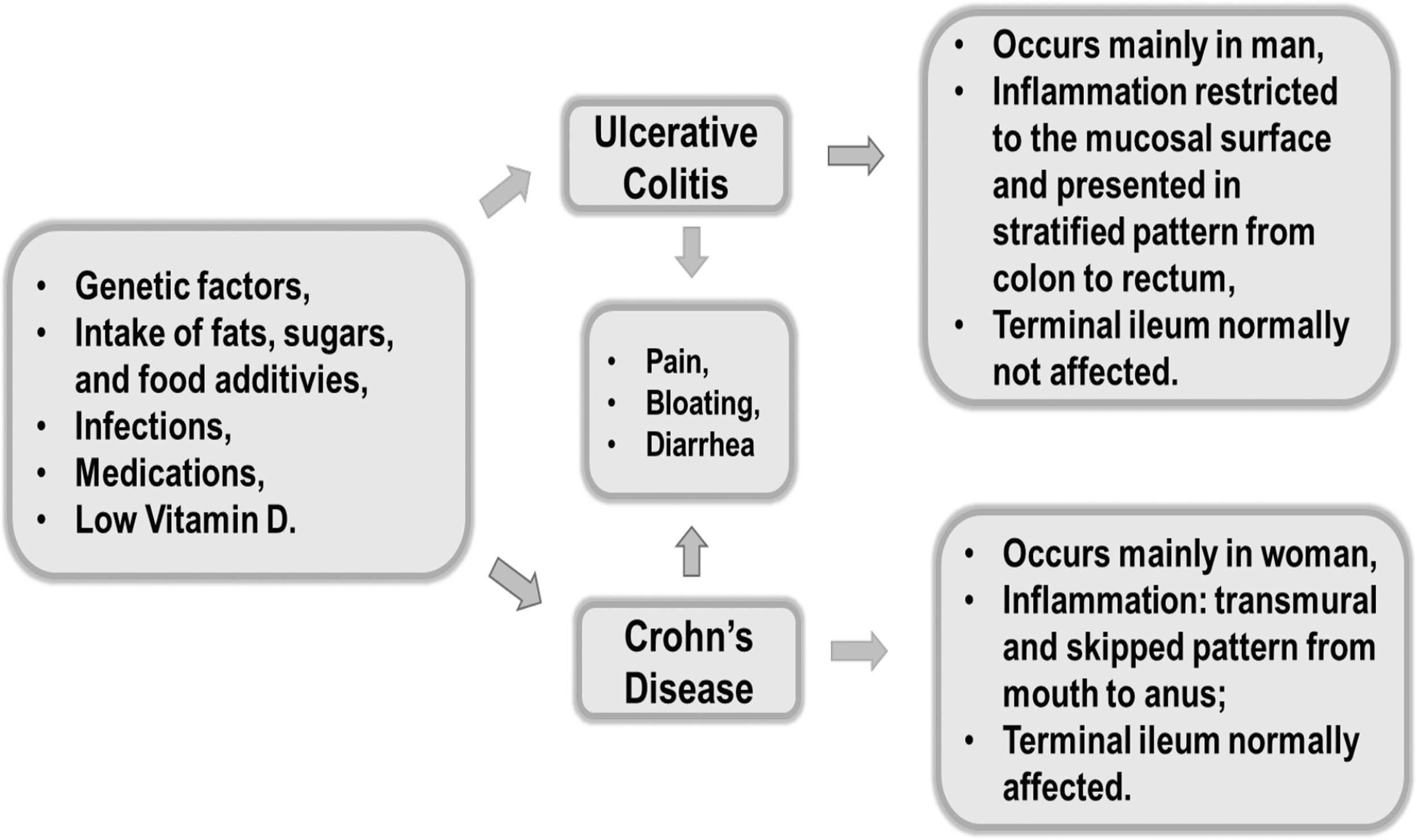
Triggering factors, symptoms, and key features of UC and CD (modified from Barbalho et al. 6 ). CD, Crohn's disease; UC, ulcerative colitis.
The FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides, and polyols) diet has emerged to deal with functional gastrointestinal disorders, such as the irritable bowel syndrome (IBS), which share similar symptoms as those presented in IBD. 7,8 The FODMAP consist of molecules that are poorly absorbed in the small intestine and are fermented by bacteria in the colon. This process may initiate the occurrence of undesired symptoms such as abdominal pain, bloating, gas, and diarrhea. For these reasons, reduction of these molecules may reduce the symptoms and improve QoL. 8 –10
To date, the relationship between IBD and FODMAP remains not elucidated, and this review aimed to summarize some important aspects of IBD and evaluate the effects of this diet on this inflammatory condition.
Materials and Methods
Focused question and language
Our focused question was “Is there an association between FODMAP and Inflammatory Bowel Disease?”
Only English articles were included.
Databases
The search for this review used the MEDLINE (U.S. National Library of Medicine's—NLM, National Institutes of Health)—PubMed/PMC.
The literature search was conducted with different combinations of terms such as (1) “Inflammatory Bowel Disease” and “FODMAP,” “fermentable oligosaccharides, disaccharides, monosaccharides, and polyols.” (2) “Ulcerative Colitis” and “FODMAP”; “fermentable oligosaccharides, disaccharides, monosaccharides, and polyols.” (3) “Crohn's Disease” and “FODMAP”; “fermentable oligosaccharides, disaccharides, monosaccharides, and polyols.”
Inclusion and exclusion criteria
Articles associating IBD and FODMAP were included (without restricting a period). We excluded poster presentation, letters, editorials, reviews, articles with repeated information, and articles not in English.
Results
Selected articles
The combination of the terms led to the selection of 6 studies that fulfilled the eligibility criteria for this review (Fig. 2). The original articles selected (Table 1) have included 336 IBD patients (140 were CD patients; 136 were UC patients; and 60 were not classified). The studies were elaborated in Universities and Healthcare Centers. Man and woman were included in these studies (18–85 years).

Flow diagram showing the combination of the terms and the final articles selected for this review. FODMAP, fermentable oligosaccharides, disaccharides, monosaccharides, and polyols; IBD, inflammatory bowel disease.
CD, Crohn's disease; FGS, functional gastrointestinal symptoms; FODMAP, fermentable oligosaccharides, disaccharides, monosaccharides, and polyols; IBD, inflammatory bowel disease; IBS, irritable bowel syndrome; QoL, quality of life; UC, ulcerative colitis.
Apart from these original articles relating to IBD and FODMAP, we performed another search to find relevant reviews involving these combinations of terms and articles that presented the pathophysiologic aspects of IBD and FODMAP definition. These topics are commented at the beginning of the Discussion section, and the results for the search are found in the Figure 2 and are discussed at the end of the Discussion section.
Discussion
IBD: Some pathophysiologic aspects
The adaptive immune system prosecutes a significant role in pathophysiological pathways of IBD. Authors have shown that the initial events in this inflammatory process involve, in sensitive subjects, modifications in the intestinal microbiota, as well as in the permeability of the epithelial barrier. These amendments are related to environmental factors such as high ingestion of sugar, fats, and food additives, infections, and medications (Fig. 1). 11,12
The above modifications drive to an impairment in the immune response leading to the inflammation. The antigens of the microbiota activate macrophages, and dendritic cells (antigen-presenting cells) and the subsequent cascade involve differentiation of naive T lymphocytes, into T helper cells (TH cells), and further expression and proliferations of cytokines such as TH1, TH2, TH9, TH17, and tumor necrosis factor-α (TNF-α) are shown in Figure 3. These cytokines are related to the bowel inflammation and, in IBD patients, interfere in the homeostasis of cells, including macrophages, dendritic cells, T cells, and fibroblasts. The pleiotropic effects of these cytokines induce death of Paneth cell and increase apoptosis of epithelial cells and tissue injury. 13 –15
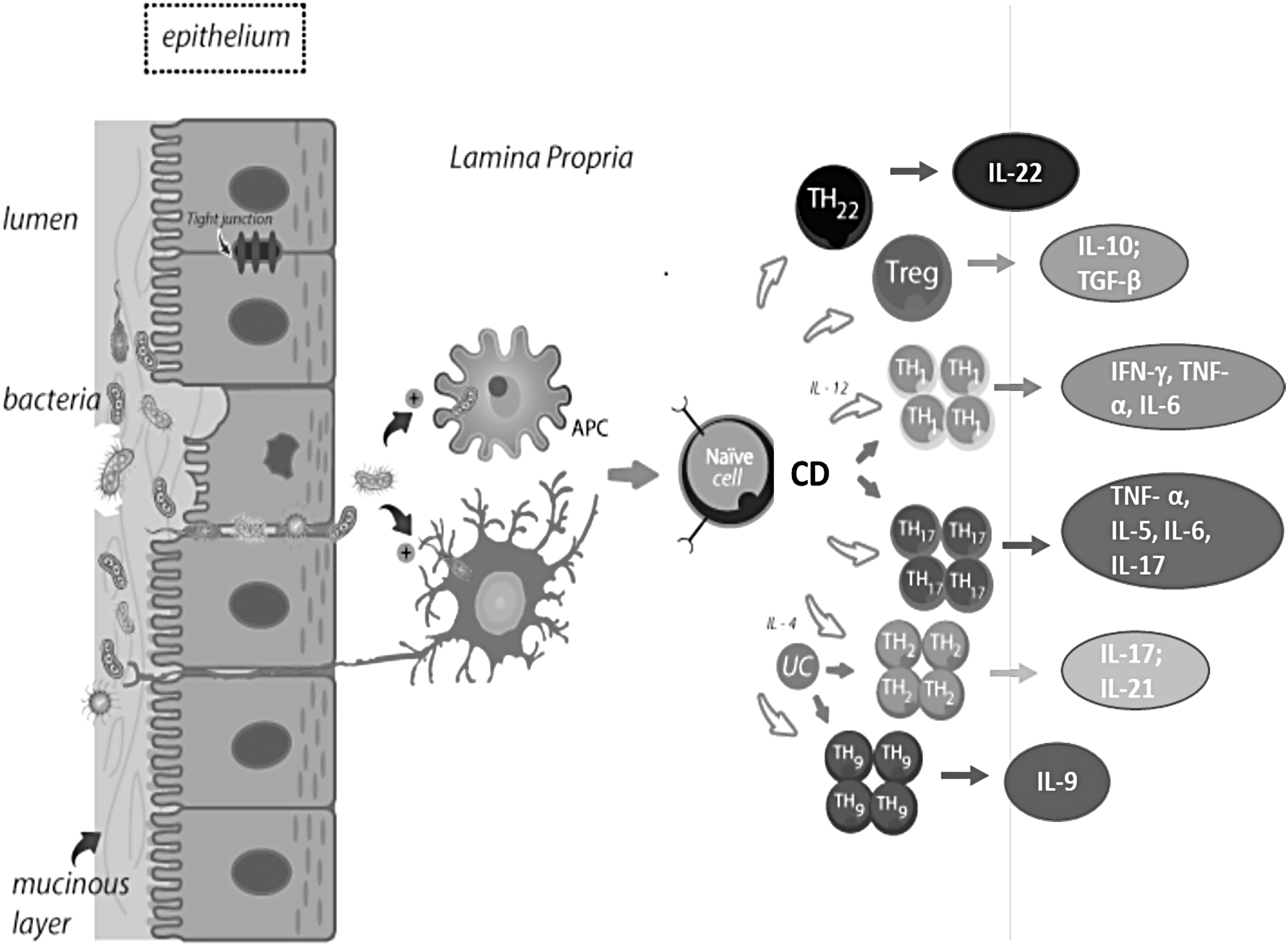
Imbalance in the bowel epithelium induces abnormal activation of the immune system (TH1, TH2, TH9, and TH17) and release of pro-inflammatory cytokines such as TNF-α, IFN-γ, IL-5, IL-6, IL-9, IL-13, IL-17, and IL-22. Treg cells are less stimulated resulting in minor expression of anti-inflammatory cytokines (IL-10 and TGF-β) and IL-22 in comparison with TH1, TH2, TH9, and TH17. IL-12 is related to the stimulation of TH1 and IL-4 with the stimulation of TH2 (based on Neurath 14 and Singh et al. 15 ). APC, antigen presenting cell; IFN-γ, interferon-γ; IL, interleukin; TGF-β, transforming growing factor β; TH, T helper; TNF-α, tumor necrosis factor-α; Treg, T regulatory cell.
As shown in Figure 3, CD and UC share some commons patterns in the inflammatory cascade. Interleukin (IL)-12 activates TH1 which is linked to the release of TNF-α, interferon-γ, and IL-6. IL-4 induces TH2 and the cytokines released are TNF-α, IL-5, IL-6, and IL-13. TH9 is related to the production of IL-9 and TH17 with the expression of IL-17 and IL-21. Activation of TH1 has been demonstrated in CD; TH2 and TH9 in UC, and TH17 in both. 14,16
These chronic inflammatory pathways besides resulting in several other consequences induce the recruitment of leukocytes and adhesion molecules perpetuating the cycle of inflammation and leading to pain, bloating bleeding modifications of the bowel habits, and increased risk of cancer. 17,18
Fermentable oligosaccharides, disaccharides, monosaccharides, and polyols
The designation FODMAP is an acronym standing for Fermentable Oligo, Di, Monosaccharides, and Polyols. These carbohydrates are grouped due to the length of the chain, and this union was performed by Australian researchers who postulated that the ingestion of this kind of molecules collaborate with the development of symptoms that appear in digestive diseases such as IBD. FODMAP are poorly absorbed in the small intestine and are highly fermentable and osmotic, resulting in the production of gas, bloating, distension, and diarrhea. 19,20 In contrast, they may play beneficial physiological effects such as modulation of immune function, enhancement of stool bulk and calcium absorption, and reduction in the levels of serum cholesterol and triglycerides. FODMAP also may induce selective stimulation of the growth of microorganisms as Bifidobacteria that play a prebiotic effect and are capable of protecting against colon cancer. These important actions of FODMAP are lost in individuals with diet poor in these molecules. 21 –23
The oligosaccharides (fructooligosaccharides) are not digested due to the lack of enzymes in humans and, in consequence, they are not absorbed. Disaccharides such as lactose are resulted by the ligation of two monosaccharides and are considered a FODMAP when the individual has insufficiency in the production of the enzyme lactase. Monosaccharides are single molecules of sugars such as glucose and fructose and do not need digestion, but when the amount of fructose is higher than glucose, it is necessary for an alternative absorption method that may be impaired in some individuals, resulting in malabsorption of fructose. The polyols are dietary sugar alcohols that present low absorption in the intestinal barrier, and it is believed that only one-third of the consumed amount is absorbed. As they are not entirely digested, they are less caloric and pass into the large intestine where they are fermented. These molecules are present in several processed foods and are largely used in food industry as thickeners and sweeteners. 19,24,25 Common foods with these short-chain carbohydrates are shown in Figure 4.
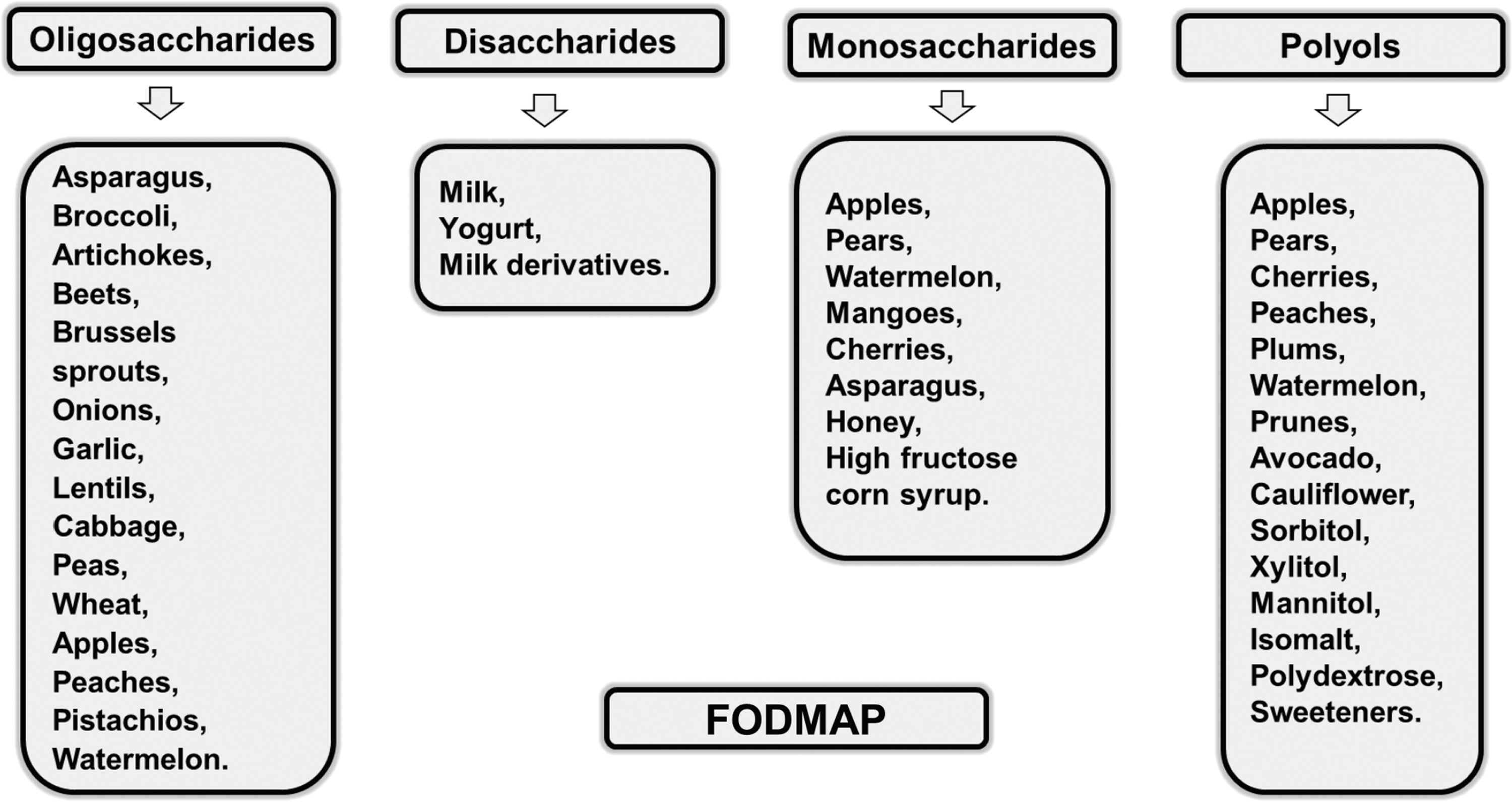
Examples of common foods with fermentable short-chain carbohydrates (FODMAP).
Some controversies are related to FODMAP once some concerns were raised. This diet is restrictive and may produce an impact on the nutritional adequacy and also can lead to patient withdrawal. Furthermore, the recommendations cannot be based only on clinical observations; there is a need of adequacies and a trained dietitian. 22,26
IBD and FODMAP: Benefits and risks
Pharmacological drugs are the main column for the treatment of IBD patients, but normally are linked to undesirable side effects. The nutritional approach is imperative in the clinical care of all IBD patients that are treated with the conventional medications. Some authors have shown that the use of a low FODMAP diet is an effective tool to the management of the common abdominal symptoms in patients with functional gastrointestinal symptoms once these molecules may trigger these symptoms due to the osmolality causing bloating, flatulence, diarrhea, and abdominal pain. 26 –28
In Table 1 we may find the results for the search for original articles that associate IBD and FODMAP. 8,9,29 –32 In general, these studies show benefits in the use of low FODMAP in patients with IBD once there is reduction in the IBS-like symptoms such as severity of flatulence, pain, bloating, fecal urgency, and stool consistency.
Symptoms such as distension, bloating, altered bowel habits, and pain are present both in IBD and IBS, and it is believed that 40% of IBD individuals may develop IBS-like symptoms. FODMAP may positively influence these symptoms once a diet with high amounts of these carbohydrates increases the gastrointestinal discomfort and, when reducing these molecules, there is an improvement of the symptoms. 8,33
A low FODMAP diet may reduce the expression of pro-inflammatory markers such as C-reactive protein and fecal calprotectin and may interfere with the microbiome and its metabolites. Besides that, it may reduce Faecalibacterium prausnitzii and Bifidobacteria. 31,34 –36
Authors believe that elevated concentrations of short-chain fatty acids in the intestinal lumen, owing to the metabolism of incompletely absorbed carbohydrates, could impair the bowel barrier function by leading to the apoptosis of epithelial cells. 20,27
Some components obtained from vegetables may interact with intestinal immune receptors playing a role in the intestinal immunity by activating the aryl hydrocarbon receptor (AhR). Intestinal lymphocytes highly express this molecule that is related to lumen defense, and during the inflammation, this receptor is downregulated in the bowel. Dietary components may interfere with AhR, affecting the expression of defensins, cytokines, and antimicrobial peptides and in the composition of the microbiome. The activation of this receptor may produce benefits in IBD. 37,38
Gibson 39 discusses the elimination of components of the diet and the following reintroduction of placebo-controlled specific foods in IBD patients. He showed that FODMAP intake induces luminal distension and functional gastrointestinal symptoms in IBD patients. Thus, the restriction of these foods may be useful for the functional bowel disorders but not in all patients.
Pedersen 40 analyzed four studies involving IBD patients with IBS and observed that a diet rich in FODMAP might be worsening in symptoms of IBS. This intake activates the bacterial fermentation increasing CH4 and H2 gas in the intestine and induces an imbalance on the absorption. Otherwise, a low FODMAP diet reduces overall symptoms, significantly decreasing the pain duration.
Ahmed et al. 41 considered that IBD is becoming an alarming situation, especially among people aging 15–35 years. Authors observed that patients on a low FODMAP diet had lower rates of abdominal pain, bloating, gas, and flatulence. Patients with IBD also showed that, even when the disease is in remission, they may have a clinical picture similar to IBS. For these reasons, the restriction of the diet should be considered even when the patient is not on the flare episodes. According to the review performed by Teruel et al., 42 some special foods and beverages may worsen functional gastrointestinal symptoms in IBD-IBS patients, but not immediately. Thus, a low FODMAP diet in these patients could reduce the symptoms.
Zhan et al. 7 performed a meta-analysis encompassing 319 quiescent IBD patients and observed that, except for constipation, there was an improvement of satisfaction with gut symptoms, diarrhea, bloating, pain, fatigue, and nausea supporting the idea that a low FODMAP diet brings benefits for decreasing gastrointestinal symptoms. This relief has been observed both in individuals with quiescent IBD and ongoing gastrointestinal symptoms. 24,43
In another meta-analysis, authors showed that the adherence to a low FODMAP diet results in general improvement of those symptoms related to IBD and IBS and lead to significant reduction of the symptom severity and patient QoL scores compared with patients that used a normal Western diet. 44
The majority of patients with functional gastrointestinal symptoms may present improvement with the intake of a low FODMAP diet as long as the disease is organic or functional, for example in IBD. This therapy improves abdominal symptoms both in adult and child IBD patients. However, these authors draw attention to the restriction of this diet that has been the subject of abuse and misconceptions and should be prescribed by a trained professional. 26,45,46
Other reviews consider the use of a low FODMAP diet in the treatment of IBD and IBS patients and show that it may reduce symptoms and improve QoL. 34,47 –49
In contrast, a low FODMAP diet may bring risks for symptomatic individuals with quiescent IBD due to the potential danger of a restrictive diet that may compromise the nutritional status (due to the reduction of many types of foods) of this kind of patient where malnutrition is common. This restrictive diet showed pouchitis in patients with an ileal pouch in a study from Croagh et al. 50 The removal of these natural carbohydrates that play prebiotic effects may lead to a remarkable impact on the bowel microbiome with unpredictable long-term effects on health. 42,51,52
There is an impact of prebiotics on the bacterial growth and metabolism that may exert influence on the immune signaling. It was observed that there might occur a dysbiosis pattern on the microbiome of patients with IBS or CD and substantially decrease the abundance of butyrate–producing Clostridium cluster XIVa and Akkermansia muciniphila that play a major role in the maintenance of homeostasis among mucosa and microbiota. It was also observed to augment in the mucus-degrading Ruminococcus torques. In addition, Bifidobacteria may be reduced, and stool pH becomes increased after the low FODMAP diet which could enable the growth of enteropathogenic colonization. For these reasons, it is of paramount importance that the restrictive low FODMAP diet should be considered only in the “induction” phase of prescribing the dietary modification. The nonresponding patients to the diet should cease FODMAP restriction. 10,24,31,34,51
The diet plays a major role in the modulation of the gut microbiome and is capable of influencing epigenetic changes. For these reasons, it should be taken into account as a therapeutic approach for the IBD patient. In contrast, the dietary recommendations for the management of this condition need to be more studied. 53
Although the low FODMAP diet shows beneficial aspects in treating the symptoms of patients with IBD and IBS and could be used as supporting the medications traditionally used in the treatment of these diseases, caution should be exercised so that this intervention does not lead to deficiencies in patients who are already vulnerable. Therefore, the professional must be qualified and must be attentive to the needs of the patient. 26
Conclusion
The use of a low FODMAP diet may not only result in the relief of the symptoms presented by patients with IBD but also may modify their nutritional status. Thus it should be used in appropriated conditions, and dietary supplements should be necessary to avoid deficiencies that could be caused by a low FODMAP diet over long periods.
We suggest that further investigations are required to elucidate when and how to apply the FODMAP diet in IBD patients once it should be compatible with the symptoms but should not cause nutritional deficiency and induce undesirable consequences for these patients and lead to the worsening of the QoL.
Footnotes
Acknowledgments
We thank Silmara Eliana Barbalho for help with the reference formating.
Author Disclosure Statement
No competing financial interests exist.