
Abstract
Excessive sugar consumption is associated with many chronic inflammatory diseases in adults. The effects of excessive sugar consumption in children have not been determined. In this study, we hypothesized that sinonasal symptoms and proinflammatory cytokine levels would be related and could be altered through reduction in sugar-sweetened beverage (SSB) consumption. To test this, we conducted a pilot study involving behavior modification and a 2-week follow-up. Seventeen children participants were recruited, and eleven completed the study. The experimental group presented with chronic nasal congestion or rhinorrhea defined by daily symptoms without acute illness for at least 3 months. The control group presented for non-nasal problems. Both groups received counseling to decrease SSB consumption. The Sinus and Nasal Quality of Life (SN-5) Survey was administered, and a blood sample was obtained by venipuncture at baseline and 2 weeks after counseling. Participants kept a 2-week food diary to document sugar intake. Serum lipid profile and inflammatory cytokines were measured. The experimental group reduced daily sugar intake, 46% versus 11% in the control. Baseline SN-5 scores were significantly worse in the experimental group and normalized to controls after intervention. Inflammatory cytokine levels were not different at baseline, but the experimental group significantly reduced in proinflammatory markers and increased the levels of anti-inflammatory markers after intervention. Our pilot data demonstrate higher sugar consumption may be associated with increased inflammatory stress and sinonasal symptoms. Reducing SSB and controlling inflammation in early childhood may have future health benefits.
Introduction
O
Few studies have investigated SSB and inflammation in children. 5 Based on these studies and clinical practice, we hypothesized that nonallergic chronic nasal symptoms and rhinorrhea in young children may be caused by chronic inflammation from excessive sugar and carbohydrate consumption. A controlled dietary change study is challenging due to the complexities of patient compliance and follow-up, sample processing between a clinic and research laboratories separated by moderate distances, and the subjective nature of only validated reporting tool for sinonasal health. Therefore, we sought to perform a pilot study to investigate the relationship between SSB and sinonasal inflammation in children at our clinic and to establish necessary parameters for a larger controlled study.
Methods
Study population
We conducted a prospective, nonrandomized cohort pilot study in children, aged 2–6 years, born full term, and without medical comorbidities, who presented to the Nemours Children's Hospital outpatient otolaryngology clinic in Orlando, Florida, between May, 2015, and October, 2015. The exclusion criteria were medical comorbidities such as liver disease, diabetes, autoimmune disorders, adenoid hypertrophy, and any other known inflammatory diseases.
As a part of the routine office visit, dietary habits, including typical daily consumption of SSB, were obtained by the pediatric otolaryngologist. A thorough patient history also verified whether patients had undergone formal allergy testing. Patients were then examined to ensure no anatomical obstruction was present as the cause of chronic nasal symptoms. Patients whose parents reported frequent SSB as a part of daily diet (more than 4–6 oz per American Academy of Pediatric [AAP] guidelines) were noted as potential subjects. The experimental group consisted of children presenting with chronic nasal congestion or rhinorrhea defined by daily symptoms without acute illness for at least 3 months or greater in duration. The control group consisted of children who came to the otolaryngology clinic for scheduled follow-up appointments for non-nasal problems (e.g., routine check-up for tympanostomy tubes). This study was approved by the Nemours Office of Human Subjects Protection (approval number 634907). All parents or legal guardians were fluent in English and gave written informed consent before beginning of the study.
Study procedures
Upon enrollment for patients in both groups, parents completed a baseline survey about their child's daily beverage intake, which included estimated daily consumption of SSB. Parents were also asked to complete a Sinus and Nasal Quality of Life (SN-5) survey. The SN-5 survey is a validated instrument consisting of five symptom-cluster items: areas of nasal obstruction, sinus infection, allergy symptoms, emotional distress, and activity limitations related to rhinorrhea. 6
All parents/legal guardians received ∼30 min of counseling with the pediatric otolaryngologist. An overview of the counseling is provided in Table 1. Parents/guardians maintained a 14-day beverage intake log. Each was given a 9-oz cup to use during the study period and asked to document the amount of SSB their children had each day. Participants in the experimental group were recommended a dietary change of decreasing sugar intake (especially from SSB) to less than 50 g per day.
SSB, sugar-sweetened beverage.
At the beginning and end of the study, nonfasting 3-mL blood samples were drawn to measure the serum inflammatory markers and blood lipid profiles. The serum concentration of inflammatory marker TNF-α, interleukin-1 beta (IL-1β), IL-6, IL-5, IL-10, and IL-13 levels were measured in duplicate using commercially available quantitative sandwich enzyme immunoassays (R&D Systems, Minneapolis, MN, USA), following the supplier's protocol. Sensitivity of all the cytokines was 15.6 pg/mL, with an assay range from pg to ng; the interassay variability was <6% and intra-assay variability was <5%, which were within manufacturer's specifications. Blood lipid profiles of total cholesterol (TC), triglycerides (TRG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein-cholesterol (LDL-C) measurements were determined by using the Cholestech L*D*X analyzer (Cholestech, Hayward, CA, USA).
Statistical analysis
Patient demographics, including all baseline variables, are reported using descriptive statistics. Continuous variables are reported as mean (±SD) or median (IQR) according to Kolmogorov–Smirnov results for normality. Student's t-test and the Mann–Whitney U-test were used for between-group comparisons for normally and non-normally distributed continuous data, respectively. Paired Student's t-test or Wilcoxon signed-rank tests were used for the baseline and end–of-trial period data on the same patients in the experimental group for normally or non-normally distributed continuous data, respectively. Comparisons of categorical data were performed using Fisher's exact test. Comparisons of ordinal data (e.g., SN-5 scores) were performed using Mann–Whitney U or Wilcoxon signed-rank tests as appropriate. All statistical tests were performed using SPSS software (v23; IBM Corp., New York, NY, USA). Test results with P < .05 were considered statistically significant.
Results
Seventeen total participants were recruited for this study. No participant presented with lower airway hyperresponsiveness or obstruction, or had documented allergy testing. Eleven participants completed the study with two visits (day 1 and 14). Six participants completed day 1, but not day 14, and were excluded from our data analysis. Among the eleven, three did not have any nasal symptoms (control group) and eight did (experimental group). Patient demographics, sex, mean body mass index (BMI), age, body temperature, baseline and final glucose levels, and sugar consumption for control and experimental groups are summarized in Table 2. There were no significant differences in age, BMI, sex, body temperature, or baseline or ending sugar intake between the control and experimental groups. There was a slight trend toward lower sugar intake in the experimental group, but this difference was nonsignificant. There was also no difference in the baseline nonfasting blood glucose level, which was 84 (15) mg/dL and 79 (6) mg/dL for the experimental and the control group, respectively. At the end of the study, there was no difference in sugar intake or glucose levels between groups. However, the experimental group did demonstrate a significant reduction in sugar intake in the experimental group, which amounted to a nearly 50% reduction (P < .01).
Results presented as mean (±SD), median (IQR), or number of participants.
P < .05 for control versus experimental comparisons at baseline.
BMI, body mass index; HDL, high-density lipoprotein; IL, interleukin; LDL, low-density lipoprotein; QOL, quality of life; TC, total cholesterol; TNF-α, tumor necrosis factor-α; TRG, triglycerides; VLDL, very low-density lipoprotein cholesterol.
SN-5 survey
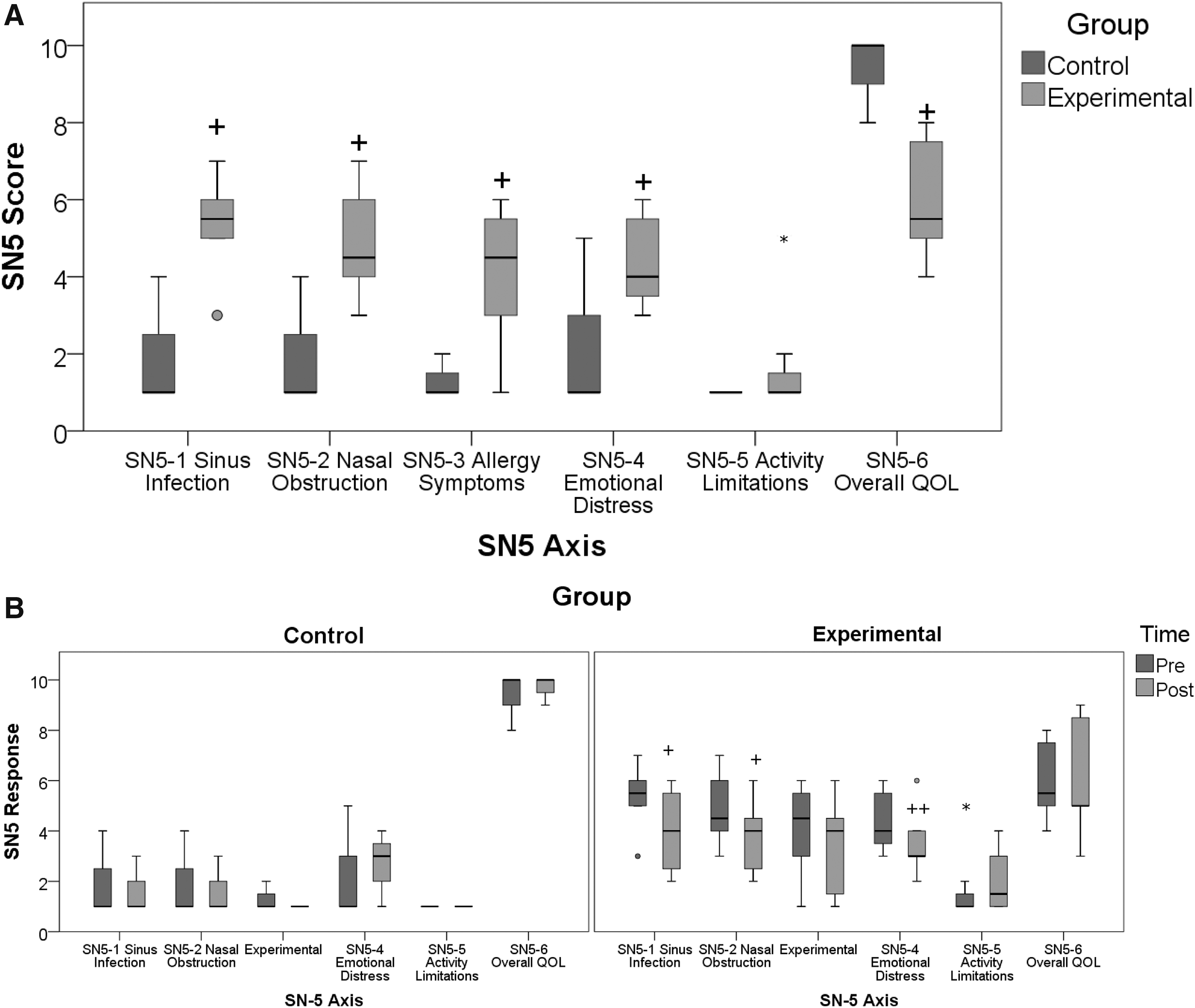
As shown in Figure 1A, there were statistically significant differences (P < .05) in sinus infection symptoms (SN5-1, which include post-nasal drip, bad breath, daytime cough, and nasal discharge), nasal obstruction (SN5-2), allergy symptoms (SN5-3, which include sneezing and itchy/watery eyes), emotional distress (SN5-4), and the overall quality of life (SN5-6) between the control and experimental groups at the baseline visit. Only activity limitation (SN5-5) was not different between control and experimental groups at baseline (P = .20). In the experimental group, following the intervention, Wilcoxon signed-rank testing demonstrated significant decreases in sinus infections (Z-score = −2.0, P < .05) and nasal obstruction (Z-score = −2.1, P < .05). There was a trend toward decreased emotional distress (Z-score = −1.8, P < .1). We found no changes in the activity levels or quality of life. As expected, we saw no changes in any of the SN-5 scores for the control group (Fig. 1B).
SN-5 survey.
Inflammatory markers
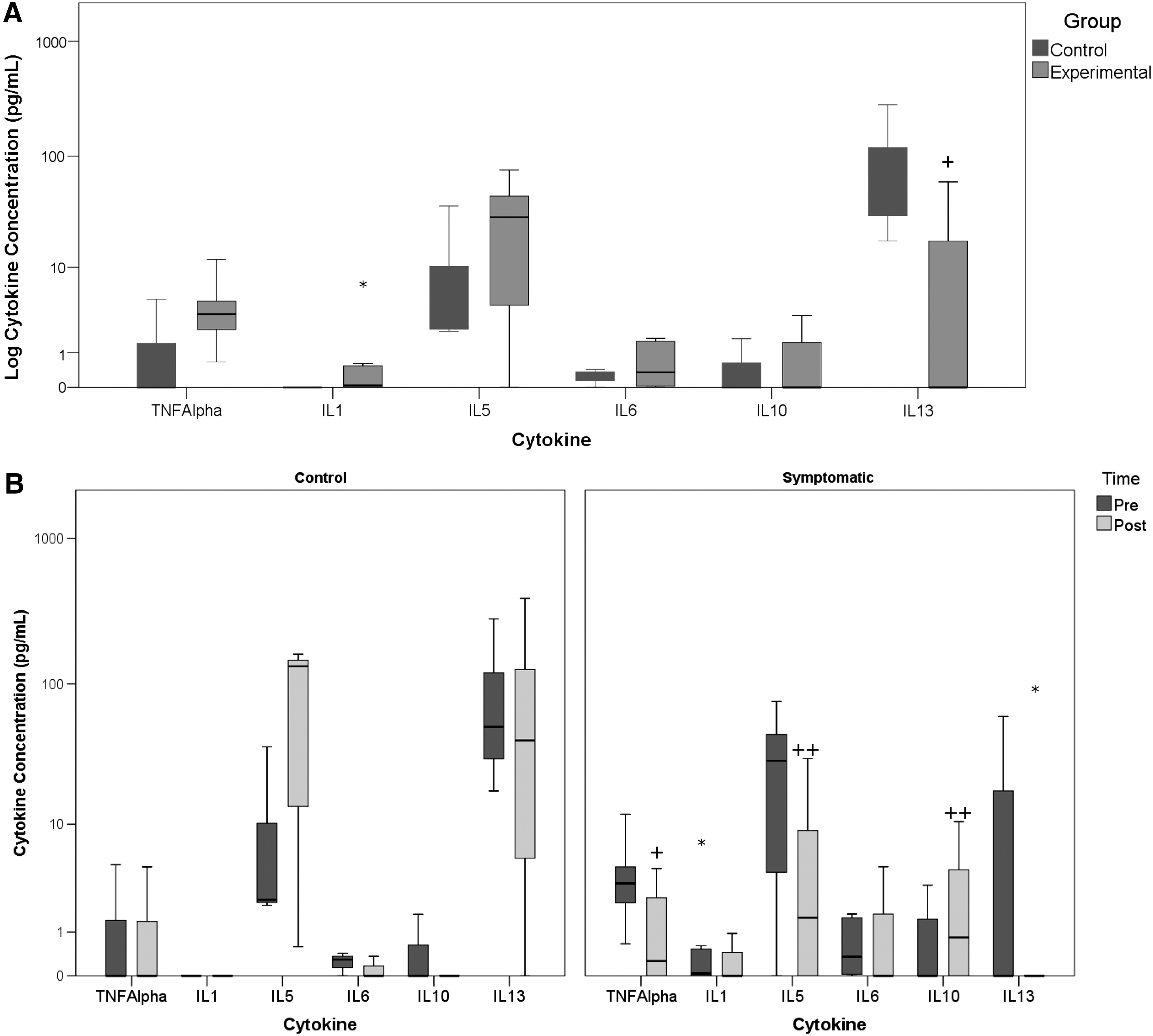
There was no statistical difference in the baseline proinflammatory markers TNF-α, IL-1β, and IL-6 or anti-inflammatory markers IL-5 and IL-10 in the experimental group compared to the control group (Table 2). However, there was a trend (P < .1) toward higher IL-13 levels in the control group. Following the 2-week decrease in SSB modification, there was no change in the TNF-α levels of the control group, but there was a significant decrease in TNF-α in the experimental group (Wilcoxon signed-rank test, Z = −2.38, P = .02). Similarly, the Wilcoxon signed-rank test showed a trend toward higher IL-10 levels in the experimental group (Z = 1.8, P = .07), but no change in the control group. There were no other differences noted for the remaining cytokines (Fig. 2).
Inflammatory markers.
Plasma lipid profiles
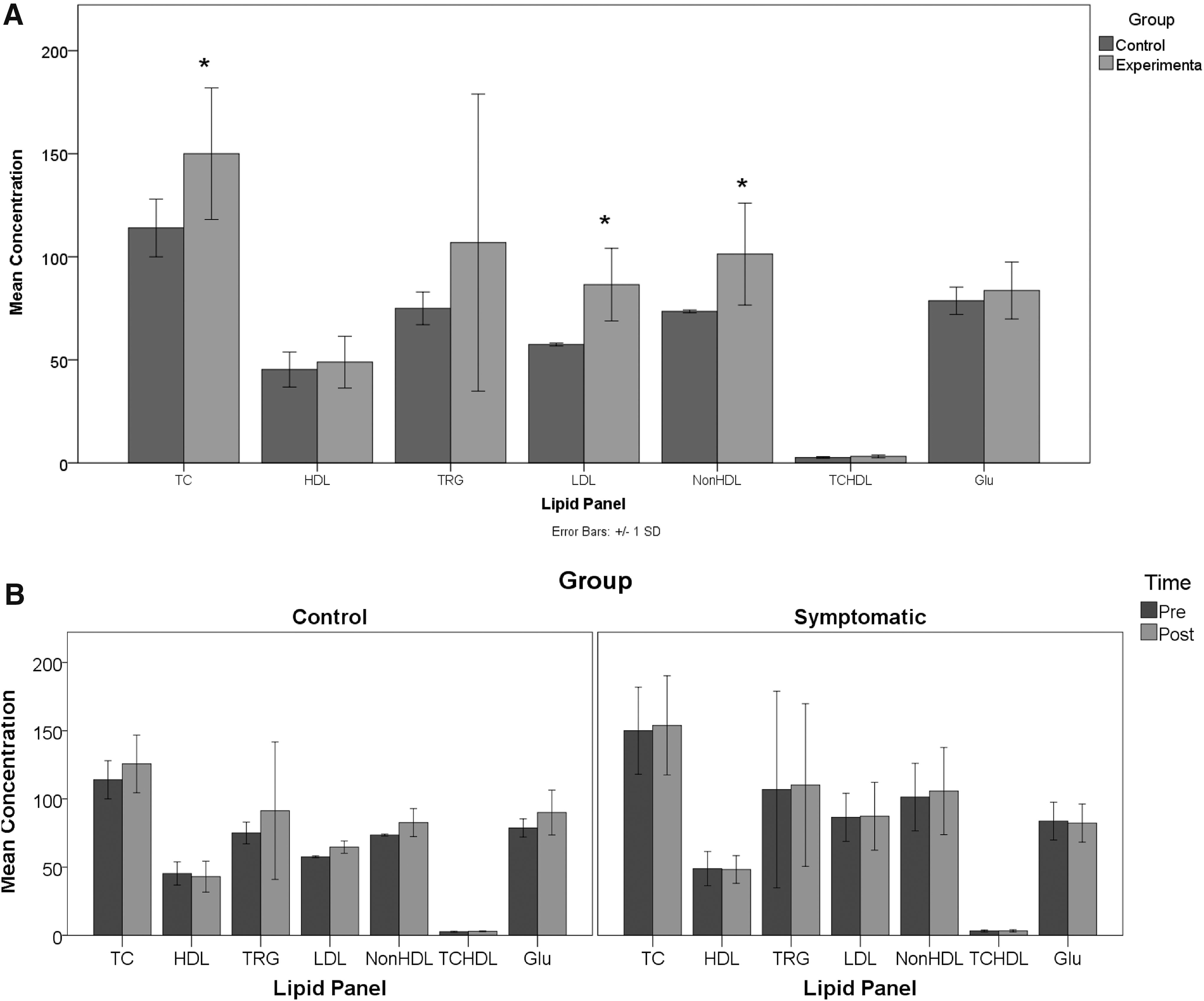
At baseline, the experimental group had significantly higher levels of TC, LDL, and non-HDL (P < .05; Table 2). The baseline levels of HDL-C, TRG, and TC/HDL ratio were also higher in the experimental group (Table 2), but the results were not statistically significant. Following intervention and 2-week diet modification, as shown in Figure 3B, there were no changes in fasting plasma lipid profiles or the fasting glucose levels of the participants, indicating that although there was a trend toward reduced sugar intake in the experimental group (83 ± 64 g vs. 47 ± 23 g, P < .1), there was no net effect on basic metabolism or nutritional status of the participants.
Plasma lipid profiles.
Discussion
In our pilot study, we examined the differences in inflammatory markers and sinonasal quality of life as related to consumption of sugar in pediatric patients. Our pilot study participants tended to have higher inflammatory markers between the experimental and the control groups (Table 2), and there was a statistical trend toward lower anti-inflammatory markers (e.g., IL-13) in the experimental groups. We saw more striking changes within the experimental population between the baseline and study endpoints—a 50% reduction in sugar intake, significant reduction in TNF-α, and an improved SN-5 profile.
In the clinical setting, preschool aged children who have nasal symptoms are commonly assumed to have allergic rhinitis as the cause of their daily symptoms. Nasal steroid spray and/or oral antihistamines are prescribed as treatments for the presumed diagnosis of allergic rhinitis. Current practice does not explore nonallergic causes of chronic nasal symptoms in otherwise healthy children, and often lack standard evaluation for testing before empiric diagnosis of “allergic rhinitis.” The relationship between inflammatory markers and allergic rhinitis has previously been defined in a framework of interaction between environmental allergens and immunoglobulins. 7 Our pilot data are intriguing as none of the children in this experimental group had hay fever symptoms, such as itchy eyes/nose and watery eyes. Furthermore, reversal of this trend after just 2 weeks of reduced sugar consumption suggests that the dietary sugar intake could have acute effects on inflammatory mediators. TNF-α is a crucial inflammatory marker that induces the production of other proinflammatory markers, such as IL-1β and IL-6. 8 Previous studies have suggested that high sugar consumption could increase TNF-α. 9 Thus, one would expect that a reduction in proinflammatory mediators would have a beneficial effect on sinonasal symptoms. Indeed, we found that after reducing sugar intake without changing other variables in their environment, the participants' TNF-α levels were decreased and their sinonasal symptoms were reduced as reported on SN-5, leading to the hypothesis that their sinonasal symptoms were less likely caused by environmental allergens.
A potential added benefit from the reduction of SSB may also have impacts beyond sinonasal symptoms. Chronic consumption of SSB—in particular, fructose-sweetened beverages—can lead to increased de novo lipid synthesis in the liver, as well as increased hepatic and muscle resistance to insulin. 10 Studies in adults have shown increased LDL-C and serum TRG levels, 11 body weight, 12 and body fat composition as a consequence of a diet high in fructose. 13 Our study is unique in that we explored this relationship in a younger patient population without asthma, who presented with chronic nasal congestion and rhinorrhea. We found elevated levels of TRG, TC, and LDL at baseline in the experimental group, which is consistent with previously published animal studies that have found increased TRG levels after 1 week of a high sucrose diet, 14 as well as work showing the association between lipid levels and childhood asthma. 15 In addition, TNF-α increases insulin resistance 16 and is intimately involved in obesity and metabolic syndrome. 17 This can be contrasted with IL-13 having the opposite effect of reducing the production of proinflammatory markers and increasing insulin sensitivity. 18 Cytokines IL-10 and IL-5 may also increase insulin sensitivity. 16,19 Thus, a long-term goal of a future study may be to also evaluate changes in insulin sensitivity and potential reduction in obesity rates in our population.
One of the challenges of our study was the high attrition rate. Some participants did not follow through to the second session and were therefore excluded from data analysis. We observed that elective peripheral blood draws in a preschool aged child and the pain and emotional distress associated with this was the most common reason cited by parents for not completing study. Future protocols should consider enrolling preschoolers undergoing elective otolaryngology procedures (tympanostomy tubes, adenoidectomy, tonsillectomy, etc.), which would allow at least baseline blood drawn to be a fasting sample and minimize pain associated with needle stick. Another limitation for this study was recall bias, which could affect the accuracy of the documentation necessary for proving a link between SSB consumption and the endpoints of the study. We acknowledge that this may not have been done daily and some participants may have completed all the surveys toward the end of the 14 days. In addition, children are not with their parents at all times and may have consumed beverages not reported to their parents. Therefore, the beverage intake may be underreported. Introduction of an app for time-stamped reporting during the larger trial might help to document the validity of the food logs and may increase compliance and reduce bias.
In summary, we describe the first pilot study in 2–6-year-old children to investigate the relationship between SSB and chronic nasal congestion mediated by inflammatory markers. The purpose of this pilot was to determine feasibility of enrollment, data collection, and sample handling. 20 Taking a very conservative approach by using the small effect size (0.37) for TNF-α between control and experimental groups at baseline found in our study (Z-score = 1.23 with 11 observations), we would estimate that an expanded study could be performed with a target enrollment of 227 patients in each arm to achieve the requisite sample size, using a paired t-test with α = 0.05, power (1 − β) = 0.9, and correcting for nonparametric testing (15% increase over parametric result), and a similar 36% attrition rate from the trial (GPower, 3.0; Universitat Kiel, Germany). We believe that such a trial would be feasible if it is conducted over at least two centers and would take ∼1 year to complete enrollment and analysis.
Limitations
For this pilot study, we focused on reduction of sugar intake through SSB only, and were unable to account for other sugar sources. Any attempt to control for other sugar source in food intake would require complete daily food intake diaries. We acknowledged this limitation during the design of the study, recognizing that attempts to control for all sources of sugar intake would require control for what children eat during all three meals and snacks. When asked, most parents were unaware what their child was given and consumed in beverages and/or foods when outside the home in child care settings. Given a potentially high variation in meals and snacks consumed at home versus daycare and preschool settings, we chose to focus only on SSB. Furthermore, our division serves a population that is highly diverse (52% Hispanic where English may not be their primary language, and 70% Medicaid or managed Medicaid for insurance). We perceived high variations in nutrition and health literacy and cultural influences on dietary habits that could be a confounding factor when conducting research and trying to counsel families to reduce sugar intake or make any other changes. Introduction of an app in the preferred patient/parent language for time-stamped reporting during the larger trial might help to document the validity of the food logs, increase compliance, and reduce bias.
A significant challenge for this study was the high attrition rate. Participants who did not follow through to the second session were therefore excluded from data analysis. This significantly contributed to our study being underpowered and led to a lack of observable difference in cytokine levels at baseline between the two groups. We observed that elective peripheral blood draws in a preschool aged child and the pain and emotional distress associated with this was the most common reason cited by parents for not completing study. Future protocols should consider alternative methods for measuring cytokines in this population. One promising methodology may be through urine analysis. 21 However, we did show significant difference in SSB reduction compliance, 11% in the control group without nasal symptoms compared to the 46% compliance reported in the symptomatic group. This may be due to the control group reporting low nasal symptoms in the first place, hence lack of perceived need to make any dietary changes. In contrast, parents/caretakers of children with chronic nasal symptoms refractory to “standard” medical therapies are like more motivated to try yet one more intervention in hopes of reducing clinical symptoms.
There are other factors our pilot study did not account for, including levels of physical activity at baseline and at times leading up to the blood draw, which may have an impact on cytokines and other inflammatory markers. Similarly, as we measured inflammatory markers and lipid markers using nonfasting blood, there are potential differences in findings between subjects during first visits and within same subject between visits.
Despite all these limitations, we learned, from this pilot study, approaches to measuring markers of inflammation in preschool aged children. Despite high attrition rate, we believe it is feasible and possible to increase parental awareness and positively influence parental behaviors affecting sugar consumption in SSB. We have demonstrated that prospective clinical trial can be performed to assess the impact of sugar intake on markers of inflammation and lipids.
Future directions
We plan to continue researching the relationship between sugar consumption in SSB and impact on markers of inflammation and lipids in preschool aged children. Soliciting patients and parents who would support preschool aged children to undergo venipuncture is difficult. The opportunity to use inflammatory markers in urine or even saliva would likely decrease attrition rate and minimize pain to subjects. Future studies may help elucidate correlation between sugar consumption and TNF-α, and ultimately answer trigger points and onset for pediatric chronic diseases based on inflammation. Regardless of study design, it is clear that a larger experimental trial is needed to answer these questions. We hope our report will stimulate other researchers to consider research in this area.
Currently, many chronic diseases are thought to be inflammatory in nature. Our desire is to create an awareness that childhood inflammation, promoted by high sugar intake, may send an ominous message that, if uncontrolled, such inflammatory stress might lead to more serious health consequences during later years.
Summary
Our pilot study indicates that reduction of SSB may improve otherwise healthy preschool aged children's chronic sinonasal symptoms, and there is likely a relationship between the consumption of SSB and rhinitis that is mediated by proinflammatory markers TNF-α, IL-1β, and IL-6, and a reduction of anti-inflammatory markers IL-5, IL-10, and IL-13. Further investigation with a larger sample size is needed to assess the significant differences with high confidence. Subsequent studies should explore measurement of inflammatory markers in urine instead of serum, and perhaps following subjects longitudinally to investigate the effects of long-term reduction of SSB on chronic nasal congestion.
Footnotes
Acknowledgments
This project was supported by a University of Central Florida College of Medicine Research Grant (2015).
Author Disclosure Statement
No competing financial interests exist.