
Abstract
We tested the hypothesis that exaggerated pressor responses observed in prehypertensive males (N = 9) during dynamic exercise are attenuated following acute dietary supplementation with grape seed extract (GSE) (i.e., a single dose). Effects of placebo and GSE (300 mg) on systolic blood pressure, diastolic blood pressure, mean arterial pressure (MAP), cardiac output (CO), stroke volume (SV), total vascular conductance (TVC), and rate × pressure product (RPP) in response to two submaximal cycling workloads (40% and 60% VO2peak) were compared 2 h after ingestion of GSE or placebo on different days, 1 week apart. Endothelial function was also evaluated using flow-mediated dilation (FMD). Placebo treatment had no effect on any of the variables. GSE supplementation attenuated MAP at both workloads (40% VO2peak: 115 ± 1 vs. 112 ± 2 mmHg; 60% VO2peak: 126 ± 2 vs. 123 ± 2 mmHg) and RPP at the lower workload. Conversely, SV, CO, and TVC were augmented during both workloads. FMD was augmented by GSE (18.9 ± 2.0 vs. 12.4% ± 2.0%). These findings indicate that in exercising prehypertensive males, a single dose of GSE reduces blood pressure, peripheral vasoconstriction, and work of the heart and enhances O2 delivery; effects that may be due, in part, to endothelium-dependent vasodilation. We propose that acute GSE treatment represents an intervention that may minimize potential increases in the risk of cardiovascular events during dynamic exercise in prehypertensives.
Introduction
T
There is evidence suggesting that progression from prehypertension to hypertension is reduced in individuals who participate in regular exercise. 3 Moreover, higher levels of aerobic fitness have been associated with lower resting BP in prehypertensive individuals. 4 . Thus, long-term exercise training may benefit these individuals by lowering BP. Conversely, exaggerated SBP and DBP responses during exercise have been reported in this group. 5,6 While potential adverse effects of these exaggerated responses are not clear, they may adversely affect the risk-to-benefit ratio of aerobic exercise as a clinical intervention for prehypertensives.
Our laboratory found that reflex-initiated increases in BP (evoked by forearm static contraction) are exaggerated in prehypertensives compared with control subjects and that this augmented response is related to increases in peripheral vasoconstriction (i.e., increased vascular resistance 7 ). Results of other studies have provided information indicating that impaired endothelium-dependent vasodilation is likely associated with prehypertension 8 and that this impairment contributes to exaggerated BP responses seen during exercise. 9 Accordingly, the endothelium may be a possible target for interventions that can modify the exaggerated blood response to exercise and reduce the risk of developing full blown hypertension in these individuals.
Dietary therapy using nutritional supplements represents a potential approach for managing prehypertension. For example, grapes are rich in polyphenols, found mostly in the seeds (60–70%). Grape seed extract (GSE) consists primarily of flavanols (flavan-3-ol derivatives) that occur in both monomeric and polymeric forms, and are the principal active compounds. 10 These active compounds contain monomers of (+)-catechin and (−)-epicatechin, and their gallic acid esters. 10 The remaining high-molecular-weight forms are poorly absorbed in the digestive tract, but along with the monomeric forms, they are subject to colonic bacterial degradation into bioavailable lower molecular weight forms. 11
Two recent studies have found that GSE supplementation can reduce resting BP in prehypertensives. 12,13 Another recent investigation has demonstrated that the mechanism underlying the antihypertensive effects of this extract in rats involves activation of endothelial nitric oxide synthase (eNOS), probably leading to an increase in nitric oxide (NO) bioavailability. 14 However, potential beneficial effects of GSE on hemodynamic responses to dynamic exercise in prehypertensives have not been examined.
These observations led us to hypothesize that a single dose of GSE (300 mg) (a) reduces BP at rest and during submaximal dynamic exercise and (b) is associated with improved endothelial function as characterized by increases in flow-mediated dilation (FMD) in the brachial artery.
Materials and Methods
Study population
The study was conducted in sedentary men (n = 9) aged 20–24 years who were recruited from the Kyung Hee University campus. This study was approved by the Institutional Review Board at Kyung Hee University. Subjects were only studied after they provided written informed consent. Only male subjects were studied because resting and exercising BP fluctuates during the phases of the menstrual cycle. 15 Consequently, detection of effects of dietary supplementation with GSE on resting and exercising BP will likely be less reliable if the phase of the menstrual cycle is not held constant. Exclusion criteria included any known systemic disease such as diabetes, alcohol consumption of more than one to two drinks per week, and/or taking of any medications or supplements that affect metabolism, BP, ability to exercise, or oxidative status.
Study design
A randomized, double-blind, crossover trial was used. After completion of initial screening and testing procedures, subjects were randomly assigned to initially receive either a single dose of placebo (PL) or GSE. After a washout period of 1 week, crossover treatment with the other supplement was conducted. During this time period, the subjects maintained their usual daily activities and diet, compiled a daily log of their activities, and completed a 3-day food diary. Before ingestion of each supplement, specific cardiovascular responses (BP, heart rate [HR], stroke volume [SV], cardiac output [CO], total vascular conductance [TVC], and rate × pressure product [RPP]) and FMD responses were evaluated at rest and during exercise. Following testing, they ingested either PL or GSE and then rested for 2 h. Subsequently, the testing procedures were repeated. Subjects were asked to rest, hydrate, and follow an identical diet for 24 h before all test days.
Exercise protocols
Resting BP was measured in the brachial artery while each subject was in a seated position. After 5 min of rest, at least three measurements were obtained 5 min apart, using a sphygmomanometer. For baseline BP, the mean of the three individual measurements was used. To determine the relative exercise intensities of the two workloads used in this study (i.e., 40% and 60% of peak O2 consumption), a peak exercise test was performed on a bicycle ergometer (Monark 828, Sweden).
The protocol began with 2 min of unloaded cycling followed by increases of 30 watts/min until the subjects could no longer maintain a cadence of 60 rpm. Breath-by-breath pulmonary gas exchange data were collected continuously with an Ultima CPX Metabolic Measurement Cart (Medgraphic, St Paul, MN, USA). The VO2peak (peak O2 consumption) obtained from this test was used as an index of functional capacity. Subjects then completed two bouts of cycling exercise at the two predetermined submaximal workloads (5 min at 40% VO2peak followed immediately by 5 min at 60% VO2peak). When cycling exercise was initiated, the workload was gradually increased until a steady state was achieved (typically 3–5 min). The workloads selected for this study were used to assess effects of dietary supplementation on hemodynamic responses during exercise. 16,17 Subjects exercised at the same absolute workloads before and after PL or GSE supplementation.
Supplementation
Twenty-four hours after the VO2peak exercise test, a double-blind, randomized, crossover study design was initiated to determine effects of acute dietary GSE supplementation (administrated as a single dose of 300 mg in capsule form; MegaNatural®-BP, Polyphenolics Inc., Madera, CA, USA) compared with PL treatment (300 mg of starch). This GSE product is a highly concentrated, purified source of polyphenolic flavan-3-ols. Total phenol content determined by the Folin–Ciocalteu method was 95.3% (grams gallic acid equivalent/100 g) and contained 2.8% gallic acid, 5.1% catechin plus epicatechin, and 87.4% total oligomers as determined by high performance liquid chromatography. It was manufactured via hydrolysis using specific, proprietary enzymes 18 to produce a product rich in polyphenolic compounds. The PL capsule was made by using starch to look identical to that of GSE. The investigator administering the exercise tests was blinded to the order of treatment.
FMD test
Measurement of FMD was performed to assess endothelial function in the brachial artery before and after PL or GSE supplementation. FMD was assessed by high-resolution ultrasound, which is widely used to evaluate peripheral endothelial function and involves the release of a temporary occlusion of the arm vasculature to generate acute increases in shear stress. 19 These measurements were performed in a quiet room at ∼22°C. The effect of GSE on endothelial function via FMD was assessed in subjects by measuring brachial artery diameter in the right arm using a high-resolution ultrasound machine (ClearVue 550, USA) and a 12 MHz transducer to image the brachial artery. The images were obtained and analyzed by the same investigator who was blinded to the treatment order. Baseline end-diastolic brachial diameters were measured with the transducer placed on the antecubital fossa 3–5 cm above its bifurcation. To provoke reactive hyperemia, the pressure cuff was placed on the upper arm and inflated to 200 mmHg for 5 min and then rapidly deflated. Images of the brachial artery were then recorded for 2 min. The absolute change in diameter was determined and FMD expressed as the highest percent change (% FMD) in brachial diameter from baseline.
Measurement of hemodynamic variables
Impedance cardiography (Physio Flow; Manatec Biomedical, France) was used to continuously measure SV and HR. The device allows for the calculation of real-time CO in healthy subjects. 20 –22 The bioimpedance device consisted of two impedance cardiography electrodes placed above the supraclavicular fossa at the base of the left side of the neck, two electrocardiography electrodes used for recording the electrocardiogram (ECG), and two electrodes placed at the xiphoid process. The Physio Flow measured the change in transthoracic impedance during the cardiac cycle. 23 CO was calculated according to the following formula: CO = HR × SVI × BSA, where HR was measured from the R-R interval determined from the first derivative of the ECG. SVI is the SV index (i.e., SV/BSA). BSA (body surface area) (meters squared) was determined according to the Haycock formula: BSA = 0.024265 × BM0.5378 × H0.3964, where BM was the body mass in kilograms and H was height in centimeters. The Physio Flow has been previously validated and found to be highly correlated with the direct Fick method at rest and during submaximal and maximal exercise. 21,24
Exercise BP was measured in the brachial artery during steady-state conditions using sphygmomanometry. All measurements in each subject were made by the same investigator. Mean arterial pressure (MAP) was calculated using the following formula: MAP = [(SBP−DBP) × 1/3] + DBP. TVC (an index of vasoconstriction) was calculated as Q/MAP. We chose to assess vascular conductance as opposed to vascular resistance because it tends to be a more reliable index of vascular tone in situations where blood flow changes to a greater extent than pressure (e.g., dynamic exercise). 25 The RPP (an index of work of the heart) was calculated as HR × SBP.
Data analysis
SV measurements using impedance cardiography (i.e., during steady-state conditions) have been reported to be reliable and valid in healthy subjects. 20 –22 Accordingly, this technique accurately measures the absolute values of CO at rest and during dynamic exercise.
The mean values of HR, SV, and CO at each 30-sec interval at rest and during mild and moderate exercise were used for comparison purposes. BP was measured between the fourth and fifth minutes of each workload during steady-state conditions. To compare effects of GSE supplementation over workloads and between groups, two-way repeated-measures ANOVA and Tukey's post hoc test were used. Means were considered to be statistically different at P < .05.
Power calculations indicated that a total sample of nine subjects was sufficient to detect estimated differences in exercise-evoked increases in BP between conditions (i.e., ≥0.80).
Results
Descriptive characteristics of the subjects are presented in Table 1.
BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; MAP, mean arterial pressure.
Absolute values of all hemodynamic variables at rest and during dynamic exercise were similar when compared between pre-PL and pre-GSE supplementation conditions.
When compared with pretreatment conditions, no effects of PL supplementation were observed on SBP, DBP, HR, MAP, SV, CO, SV, TVC, or RPP at rest or during both workloads (Figs. 1 and 2).
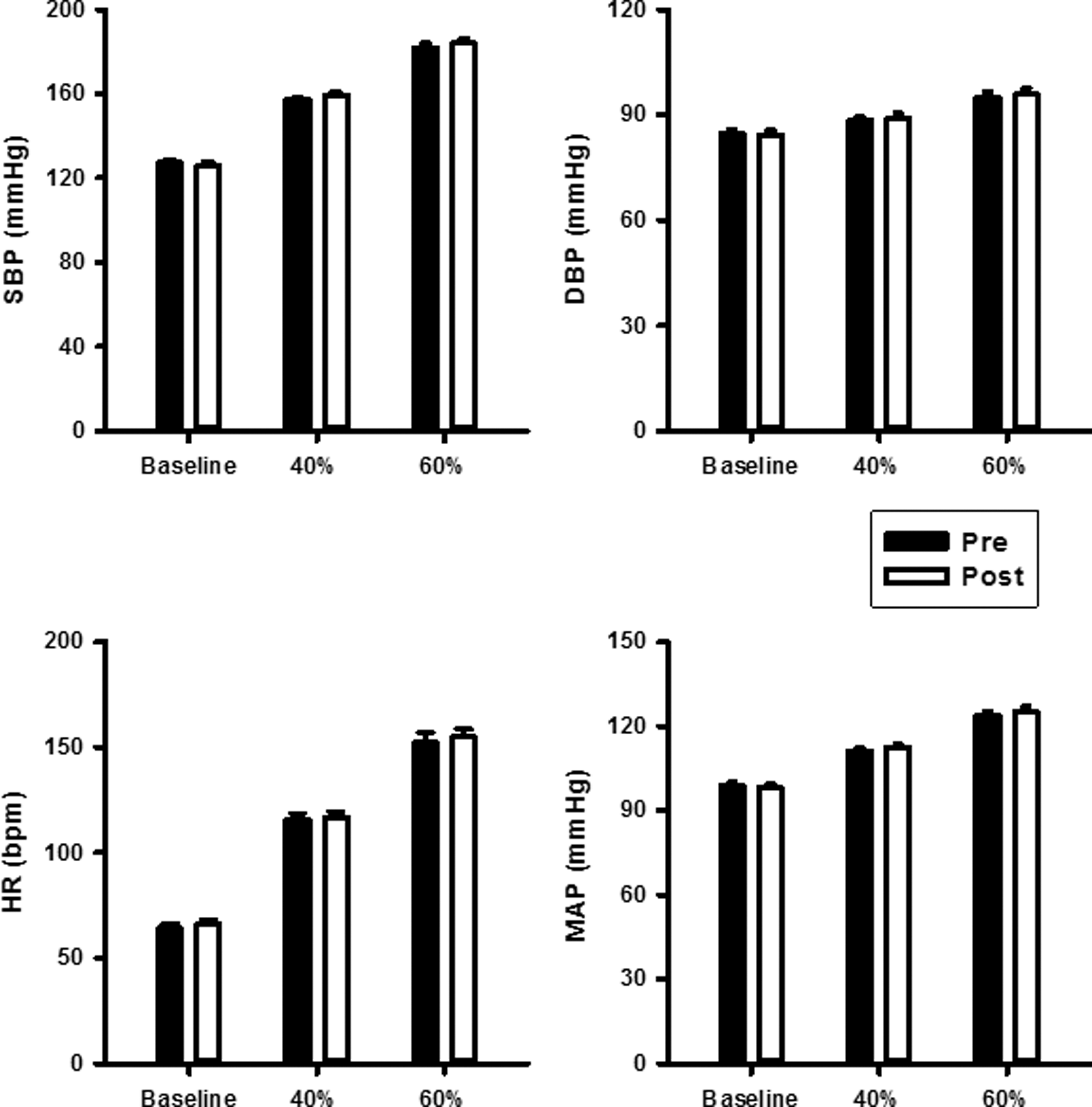
Effects of PL supplementation on SBP, DBP, MAP, and HR at rest and during dynamic exercise (n = 9). PL, placebo; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate; MAP, mean arterial pressure.
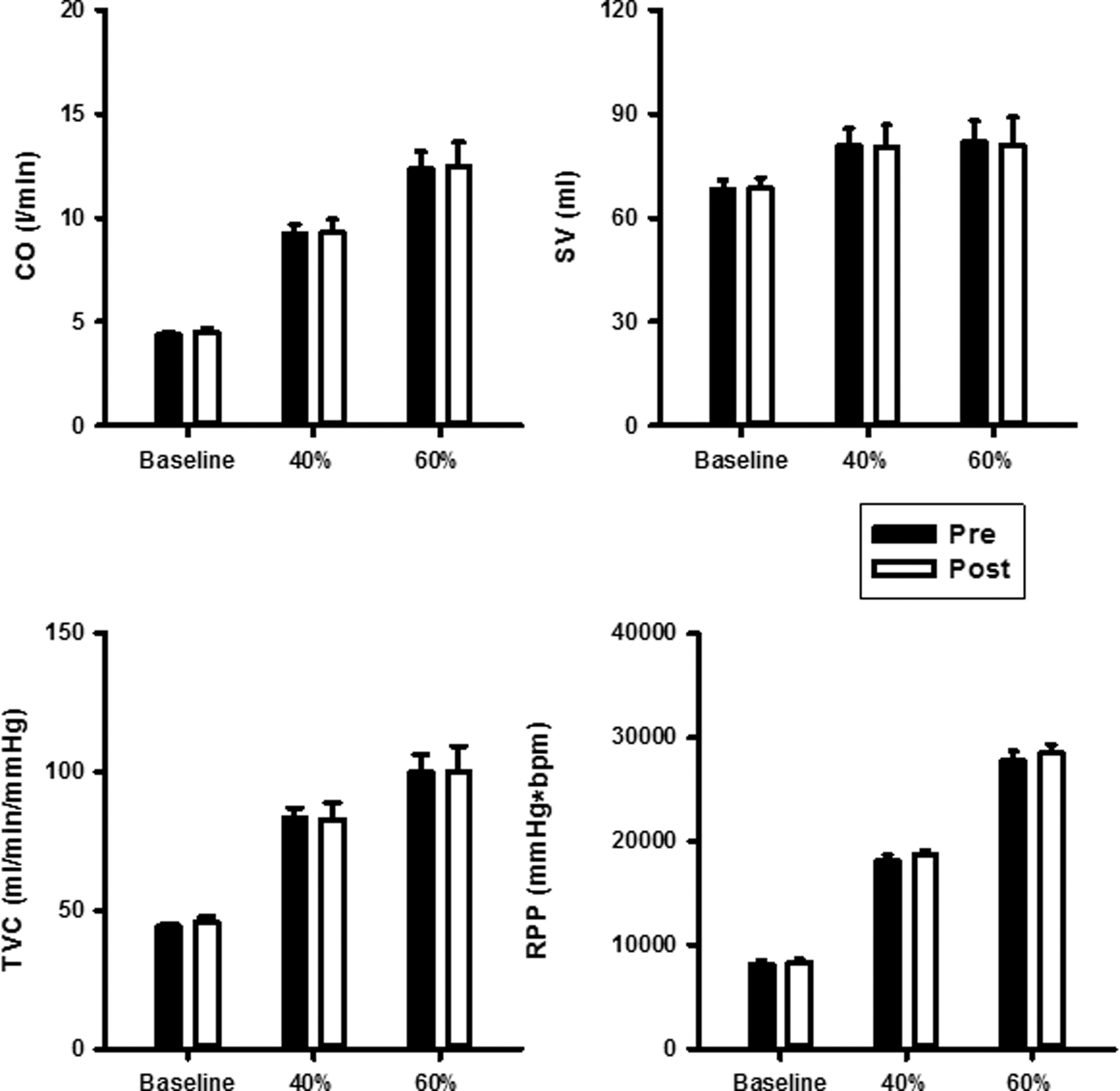
Effects of PL supplementation on CO, SV, TVC, and RPP at rest and during dynamic exercise (n = 9). CO, cardiac output; SV, stroke volume; TVC, total vascular conductance.
Compared with pretreatment conditions, GSE attenuated SBP, DBP, and MAP at rest and during exercise (P < .05) (Fig. 3). HR was significantly higher following GSE treatment at the 40% VO2peak workload, while no differences between conditions were observed at rest or during the 60% VO2peak workload (Fig. 3). GSE enhanced SV, CO, and TVC at both 40% and 60% VO2peak workloads but had no effect on resting values (Fig. 4). RPP was reduced at rest and during the higher workload only (Fig. 4).

Effects of GSE supplementation on SBP, DBP, MAP, and HR at rest and during dynamic exercise (n = 9). *P < .05 versus presupplementation (PRE). GSE, grape seed extract.
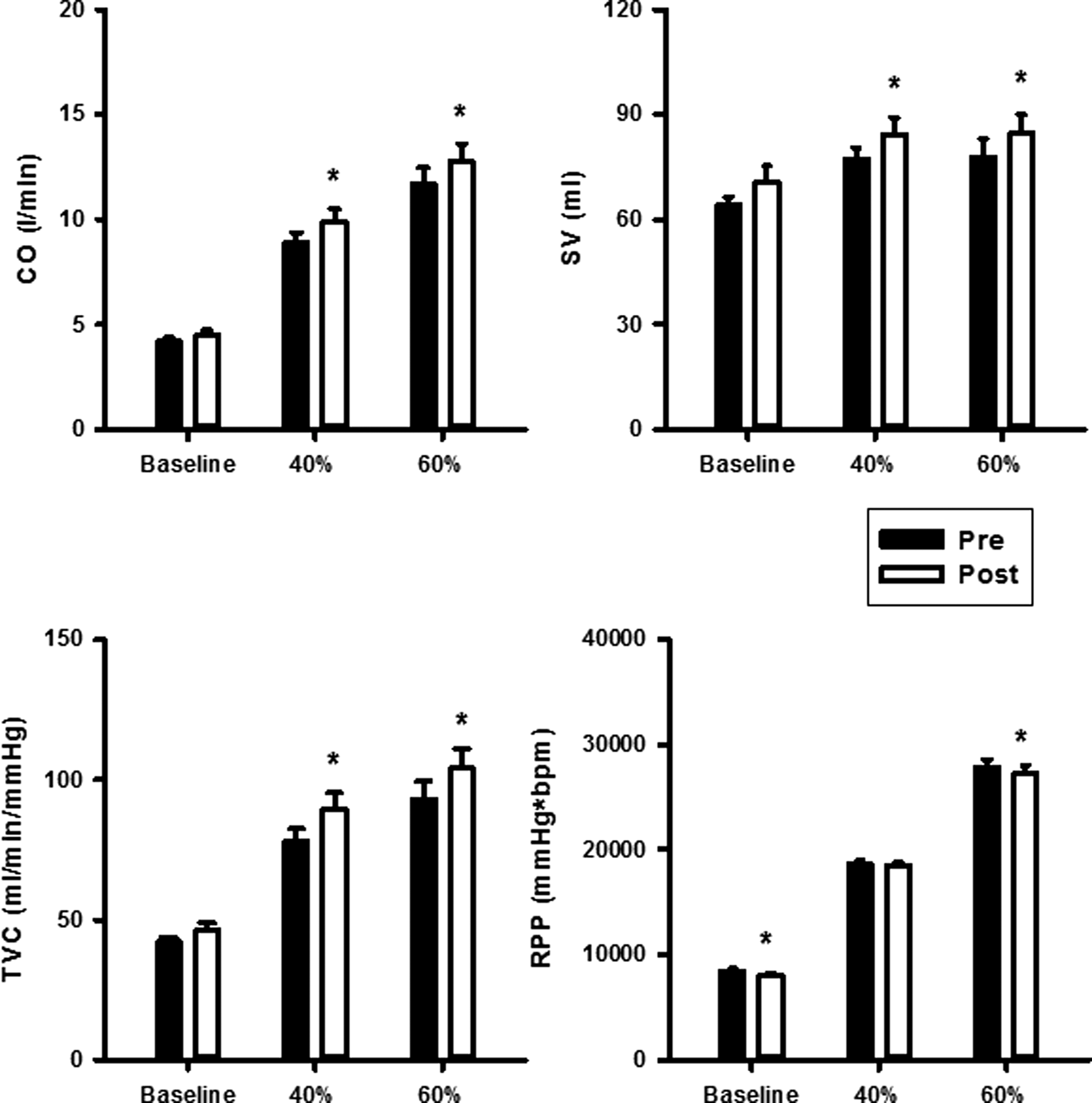
Effects of GSE supplementation on CO, SV, TVC, and RPP at rest and during dynamic exercise (n = 9). *P < .05 versus presupplementation (PRE).
GSE supplementation heightened both FMD responses and changes in brachial artery diameter (Fig. 5). PL treatment had no effect on either variable.
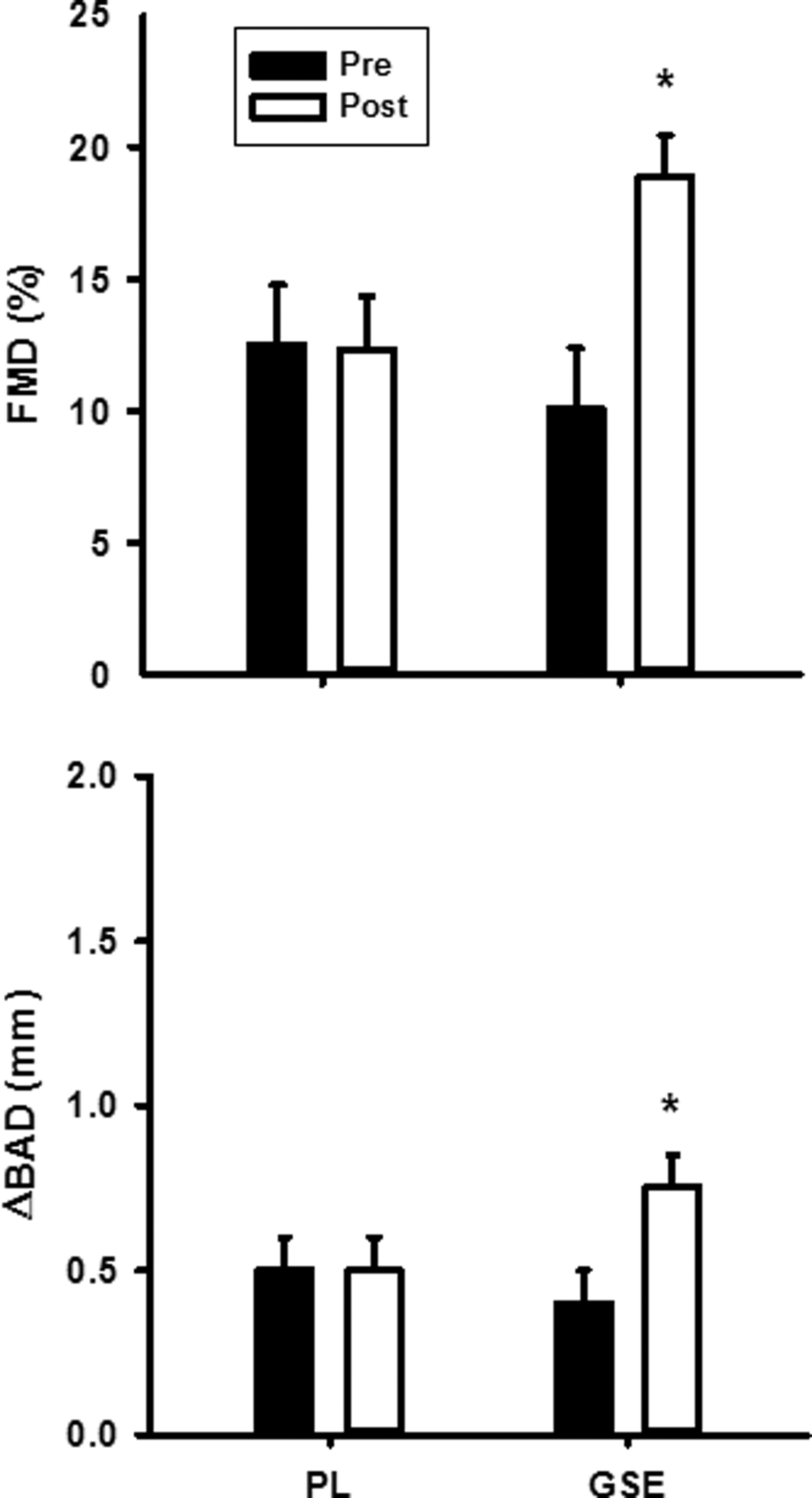
Changes in FMD and BAD before and after PL and GSE supplementation (n = 9). *P < .05 versus presupplementation. FMD, flow-mediated dilation; BAD, brachial artery diameter.
Discussion
The results of this investigation confirmed our hypothesis that a single dose of GSE reduces BP at rest and during submaximal cycling exercise. During exercise, this reduction was associated with increases in TVC that were likely linked to improvements in endothelial function (i.e., increases in FMD). Notably, attenuations in BP were modest (e.g., 3–4 mmHg reductions in MAP in response to both workloads). This outcome may have been due to opposing effects of concomitant increases in CO according to rearrangement of the Basic Flow equation, where MAP = CO ÷ TVC. However, the combination of reductions in BP and RPP, along with increases in TVC, SV, and CO, supports the contention that acute GSE supplementation enhances O2 delivery (i.e., CO × arterial O2 content) and attenuates peripheral vasoconstriction, afterload, and work of the heart in prehypertensive males during exercise.
On the contrary, it is not clear which hemodynamic mechanisms were responsible for GSE-evoked reductions in resting BP, because neither CO nor TVC was statistically different compared with presupplementation values. Yet, GSE supplementation did increase TVC in six of our nine subjects. This outcome suggests a trend for a reduction in this variable. It is also possible that a larger sample size may be necessary to detect actual statistical differences in this variable between pre- and postconditions.
Our study is the only one that has examined the effects of an acute dose of GSE in prehypertensives and found that it can enhance endothelial function (i.e., increase FMD). The only other study of FMD in individuals reported that chronic GSE supplementation (6 weeks with a similar dose) had no effects, even though resting BP was reduced. 12 Consequently, it may be that acute/single-dose effects of GSE on endothelial function are not maintained over time. However, age and gender differences may also have been intervening factors as the subjects in the previous study were older (25–65 vs. 20–24 years) and included females. Thus, investigation of chronic effects of GSE supplementation on endothelial function and hemodynamic responses to dynamic exercise (using a subject population similar to ours) is needed to determine if this is actually the case.
Identification of mechanisms underlying the action of flavanols is problematic due to the plethora of phytochemical factors that may cause as-yet-unidentified effects. 26,27 However, acute supplementation with flavanol-rich foods such as cocoa and dark chocolate (as a single dose or 5–14 days of treatment) has been reported to cause vasodilation and/or enhance endothelial function in humans (i.e., elevations in FMD) 28 –31 via activation of the NO system. 29 Short-term supplementation (5 days) with cocoa that is rich in (−)-epicatechin and (−)-catechin produces marked vasodilation that can be reversed by eNOS inhibition (L-NAME). 29 More specifically, single doses of (−)-epicatechin (1 or 2 mg/kg), similar to those found in a high flavanol cocoa drink, are capable of causing relaxation of preconstricted rabbit aortic rings; effects that were reversed by NOS blockade. 27 These observations are relevant to the present study because (−)-epicatechin is an abundant flavanol in GSE. 10
It is believed that the primary molecular pathway underlying the actions of polyphenols such as (−)-epicatechin involves Src-dependent activation of phosphatidylinositol 3 kinase, which phosphorylates Akt kinase, an important protein involved in the phosphorylation and subsequent activation of eNOS. 26 Subsequent increases in NO can lead to consequent activation of soluble guanylate cyclase, cyclic GMP, and protein kinase G phosphorylation to cause vascular smooth muscle relaxation. 32 Evidence supporting these possible mechanisms comes from studies using grape skin extract, 33,34 which like GSE contains epicatechin, catechin, and gallic acid. 35 The investigators found that this extract causes dose-dependent endothelium vasodilatory effects in the perfused mesenteric vasculature of the rat that can be attenuated by inhibition of eNOS.
Another potential mechanism underlying possible effects of (−)-epicatechin on BP and endothelial function is related to its effects on endothelin-1 (ET-1); a potent vasoconstrictor released from the vascular endothelium. 26 Results from a study of healthy humans revealed that an oral dose of 300 mg of (−)-epicatechin decreased plasma concentrations of ET-1 and increased those of NO metabolites in plasma (i.e., nitrates), suggesting that this flavanol can also increase NO bioavailability via reductions in the synthesis of ET-1. 36 This phenomenon appears to be due to the ability of (−)-epicatechin to diminish ET-1-induced generation of the superoxide radical (O2 −) via the ET-1 ETA receptor/NADPH oxidase pathway. 37 As a result, the reaction of O2 − with NO to produce peroxynitrate is reduced to the point where NO bioavailability increases. 38
The outcome above implies that (−)-epicatechin can lessen the effects of oxidative stress by attenuating levels of reactive oxide species. Other flavonoids found in GSE have also been shown to mediate reductions in oxidative status that may lead to increases in NO bioavailability. These compounds, whose antioxidant activity has been characterized by reductions in urine redox potential, were in addition to (−)-epicatechin and (+)-catechin, procyanidin dimers B1–B4. 39
In an earlier study, we determined that the elevated BP response to static handgrip contraction in prehypertensives was related to an increase in the production of skeletal muscle metabolites (i.e., lactic acid and H+) 40 that can activate the exercise metaboreflex. 41 Prehypertensives are prone to insulin resistance and reductions in glucose tolerance. 42,43 If this were the case in our subjects during dynamic exercise, then changes in skeletal muscle glucose uptake and metabolism may have occurred such that concomitant increases in lactic acid and H+ were heightened. Since GSE supplementation can improve postprandial glucose responses in humans 44 and prevent insulin resistance in rats fed a fructose diet, 45 it is possible that GSE lessened exercise-evoked production of these two metabolites in our subjects; an effect that might have tempered activation of the muscle metaboreflex. However, we have no evidence to support this contention. We did not assess lactate or pH, due to the difficulty involved in obtaining venous blood samples from dynamically contracting skeletal muscle.
We selected the 300 mg daily dose of GSE based on the results of previous studies where a similar dose lowered resting BP in prehypertensives. 12,13 Our acute treatment protocol was chosen because preliminary findings in our laboratory demonstrated that a single dose of GSE can reduce resting BP in prehypertensive men. Our single-dose treatment was different than those used in the two studies above, where GSE was chronically administered for 6 or 8 weeks, indicating that attenuating effects of GSE supplementation on resting BP can occur in a very short period of time.
Limitations to the study
One limitation of our study was that no indices of NO bioavailability (e.g., nitrates and nitrite concentrations) were assessed. Measurement of these indices would have allowed us to draw stronger conclusions concerning the contribution of NO bioavailability to GSE-induced improvements in endothelial function.
In conclusion, results of this investigation indicate that a single dose of 300 mg of GSE causes moderate reductions in SBP, DBP, and MAP at rest and during exercise. This reduction was associated with increases in SV, CO, and TVC and a decrease in RPP during exercise. These outcomes indicate that the primary hemodynamic mechanism responsible for the reduction in BP during exercise was a decrease in peripheral vascular resistance. The increases in SV and CO during exercise suggest that GSE enhanced O2 delivery, while the corresponding decrease in RPP provides evidence that work of the heart was lessened. Thus, GSE may act as a nutraceutical that acutely provides a two-pronged intervention in prehypertension. On the one hand, it has the potential to reduce ambient BP. On the other hand, it appears to be capable of attenuating the exaggerated BP to dynamic exercise; an outcome that could minimize the potential increased risk of cardiovascular events during this type of activity. 46
Footnotes
Acknowledgments
The authors sincerely thank the subjects for volunteering to participate in the study. This study was supported by a grant from Kyung Hee University.
Author Disclosure Statement
No competing financial interests exist.