
Abstract
Inflammatory bowel diseases (IBD), including Crohn's disease and ulcerative colitis, are chronic inflammatory disorders of the gastrointestinal tract whose prevalence has been dramatically increasing over the past decade. New studies have shown that IBD is the second most common chronic inflammatory disease worldwide after rheumatoid arthritis, affecting millions of people mainly in industrialized countries. Symptoms of IBD include frequent bloody diarrhea, abdominal cramping, anorexia, abdominal distension, and emesis. Although the exact etiology is unknown, it has been postulated that immunological, microbial, environmental, nutritional, and genetic factors contribute to the pathogenesis and severity of IBD. Today, no treatment has consistently been shown to be successful in treating IBD. This review summarizes current research on the epidemiology, etiology, pathophysiology, and existing treatment approaches, including pharmaceutical and nutritional options for IBD.
Introduction
I
CD, Crohn's disease; UC, ulcerative colitis.
IBD is an idiopathic disease, however, various environmental, genetic, and immunological factors are hypothesized to be involved in disease etiology. Complex interactions among the host's immune system, environmental antigen entry into the gut lamina propria, and host genotype are thought to be involved in IBD development. 6 –8 Sewell et al., (2009) 9 describes the immunopathogenesis of IBD as a three-stage model involving (1) luminal antigen penetration of the lamina propria, (2) impaired natural antigenic clearance, and (3) compensatory immune response. The proposed etiopathological model has been represented in Figure 1. In brief, an antigenic stimulus triggers mucosal immune cells of the gut to secrete several pro- and anti-inflammatory cytokines such as TNF-α, INF-γ, IL-6, IL-1β, IL-12, IL-22, and IL-10. The dysregulation of these cytokines likely results in IBD pathology, which are the current focus of targeted therapeutics. 10 For example, in human IBD subjects, TNF-α levels have been reported to be several orders of magnitude higher compared with those of control subjects and have prompted the adoption of anti-TNF-α therapeutics, such as adalimumab, in conventional therapy. 11,12
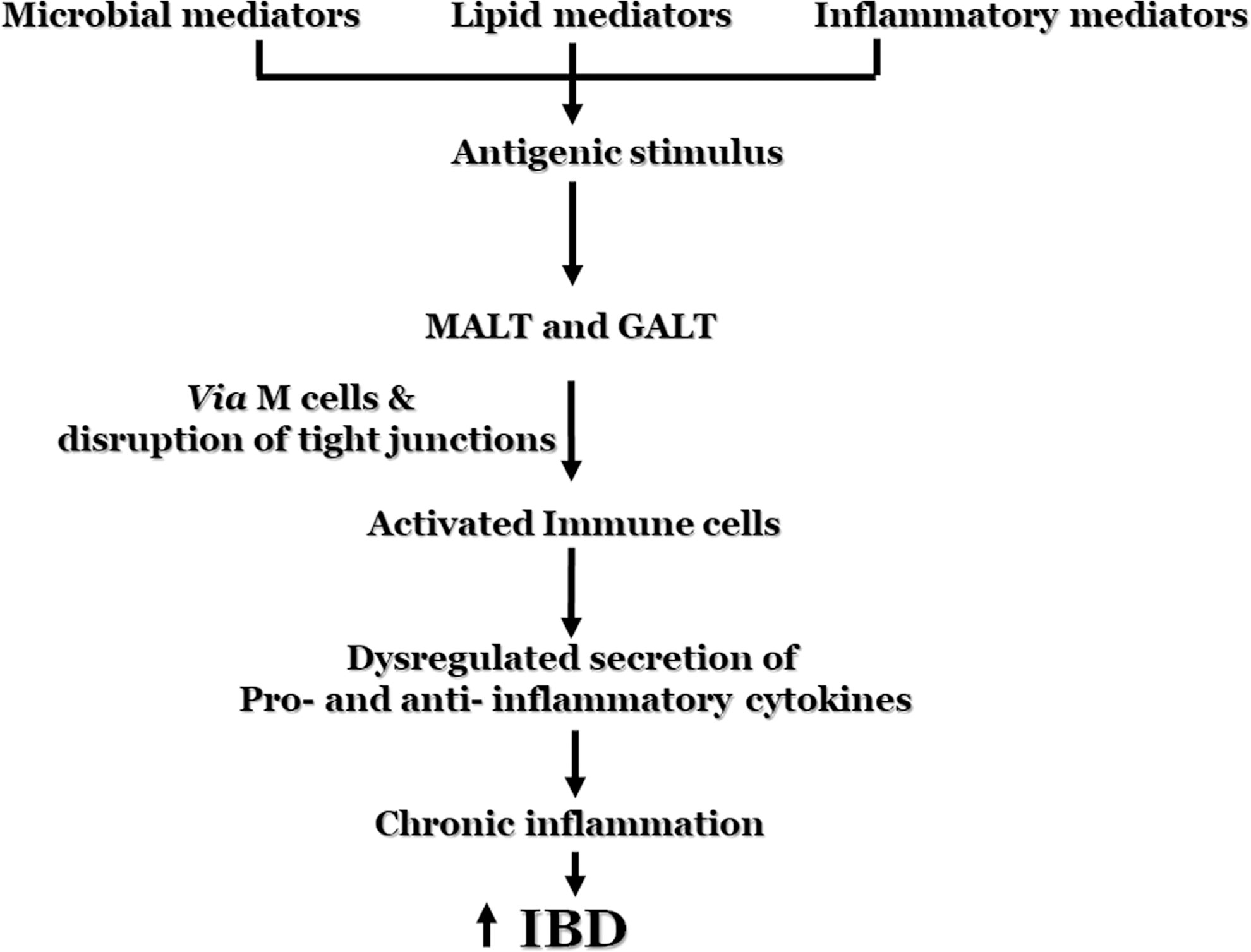
Mechanism involved in the pathogenesis of IBD. GALT, gut associated lymphoid tissue; IBD, inflammatory bowel diseases; MALT, mucous associated lymphoid tissue.
In this review, we emphasize on clinical manifestations of IBD followed by etiology diagnostic tools and future therapeutic approaches.
Clinical manifestations of IBD
CD and UC are chronic, relapsing inflammatory intestinal diseases, but have different clinical aspects. One of the most common and consistent features in UC patients is the presence of blood and mucus in the stool, which is less common in CD patients. 13 Consequently, bloody stools alarm patients resulting in earlier presentation to health professionals, and thus higher diagnostic rates of UC. 14 In addition, abdominal pain, especially during bowel movements, is observed in ∼50–90% of pediatric patients with UC. 15 Pain usually presents in the left lower quadrant of the abdomen and is associated with distal pancolitis.
Unlike UC, CD patients have fewer symptoms in the early stages, making diagnosis difficult. 14 Abdominal pain, anorexia, diarrhea, weight loss, early satiety, nausea, emesis, and dysphagia are common features of CD, 11 but are also common symptoms associated with many GI pathologies. 16 CD patients typically suffer from postprandial, periumbilical abdominal pain involving the ileum and proximal colon. Tenderness in the right lower quadrant and inflammatory masses are also observed. In CD patients, caloric intake is decreased in an effort to diminish postprandial discomfort, leading to poor nutrition, vitamin absorption, growth failure, and weight loss. Increasing abdominal cramping, distension, and emesis associated with borborygmi (rumbling or gurgling noise) are indicative of advancing inflammation leading to partial or complete intestinal obstruction via stricturing. 17
Extraintestinal features observed in IBD patients include fever, weight loss, poor growth, delayed sexual maturation, hepatic and renal diseases, arthritis, ophthalmologic, and bone diseases. 18
Incidence and prevalence of IBD
The incidence and prevalence of both CD and UC have been increasing worldwide among pediatric and adult populations in recent years. 19 The prevalence of CD and UC is the highest in Northern Europe and North America, however, the incidence rate (IR) has been rising continuously in Southern Europe and Asia as well. 20 According to CDC reports, 3.1 million Americans and 2.2 million Europeans currently suffer from IBD, and these rates are increasing annually 21 (Tables 2 and 3) and may be directly associated with the industrialization and westernization of diet (high saturated fat, high carbohydrate, and low fiber). 22 Because the diagnosis of UC before CD is typical, research should focus on prevention of CD by earlier diagnosis of UC.
Incidence is a measurement of the number of new cases arising in a population at a particular period of time.
Prevalence is a measurement of all individuals affected by the disease at a particular time.
Several factors are involved in the etiology of IBD with geographical location playing a major role (Fig. 2). One interesting observation is migration from low-prevalence areas to higher prevalence areas increases risk. 23 Specifically, one study showed children migrating to British Columbia (high-prevalance area) from South Asia (low-prevalance area) exhibited higher IBD rates compared with the rest of the pediatric population of British Columbia. 24

Etiological factors of IBD.
In addition to geography, age and gender are important factors in pathogenesis. Most Americans are diagnosed before the age of 35, the IR follows a bimodal distribution where the first peak is observed at 20–39 years of age and the second peak at 60 years. 25 Comparatively, most Asians are diagnosed later in life, most commonly above 60 years. 26 In terms of gender differences, only slight changes in IRs are observed across multiple studies. One study showed that males aged 5–9 years and 10–14 years old demonstrated a higher incidence of CD compared with females, but was similar between both genders in the 15–17-year age group. 27
Environmental Factors Responsible for the Etiology of Ibd
The GI tract is under constant environmental exposure. Although several environmental risk factors have been studied to date such as socioeconomic status and diet, none completely explains the determinants of IBD. 28 External stimuli, including antibiotics, nonsteroidal anti-inflammatory drugs, and other drugs such as isotretinoin, oral contraceptives, mycophenolate mofetil, etanercept, ipilimumab, sodium phosphate, rituximab, and microbes (either part of the normal microflora or newly introduced), are also risk factors. 29,30
Air pollution has been considered a major cause of several adverse health issues and is associated with a variety of diseases, including asthma, myocardial infarction, appendicitis, and rheumatoid arthritis. 31 –33 According to Kaplan et al., residential exposure to ambient air pollution, mainly sulphur dioxide, was significantly associated with the development of CD and UC in children and young adults. 34
Several neurobehavioral factors such as stress and depression increase the risk for IBD. 35 Although smoking has been found to be positively correlated with CD, it has been shown to be negatively associated with UC. 36,37 Many questions still exist such as whether any unknown environmental factors play a role in IBD or whether there is a common triggering reaction shared between these factors.
Gut Microbiota in the Etiology of Ibd
The mammalian GI tract is home to ∼1014 microbes, consisting of 450–500 species, 10 times the number of cells in the human body. 38 Host–microbe interactions are important to numerous aspects of normal mammalian physiology, ranging from metabolic activity to immune homeostasis. 39 Studies have confirmed that a balance in GI microflora is essential for proper care of health maintenance in host; microbial dysbiosis has been postulated to be involved in a wide variety of extraenteric diseases such as cardiovascular disease, diabetes, 40 obesity, 41 fatty liver, 42 inflammatory diseases, 43 anxiety, 44 aging, infectious diseases, autoimmune disease, and even cancer. 45
Gut microflora composition has been one of the most extensively studied environmental determinant implicated in IBD etiology. Intestinal microflora contains a rich diversity of bacteria that is generally beneficial to the host, but can be pathogenic when introduced into sterile tissue (opportunists) or when the native protective microflora diminish and are replaced. 46 The predominant species of microflora in humans differ according to the body niche (oral cavity, esophagus, stomach, ileum, jejunum, colon or urinary tract, and excretory pore). 47 –52 For example, the colon has neutral to mild acidic pH, which permits the largest microbial community to reside. In contrast, the small intestine provides a more challenging environment for microbial colonizers given the fairly short transit times (3–5 h) and high bile acid concentrations. 53,54 Molecular analysis has revealed that the jejunum and ileum are enriched with facultative anaerobes, including gram-positive streptococci, lactobacilli, and enterococci species and gram-negative Proteobacteria and Bacteroides. 53,54 They play a major role in nutrient metabolism, xenobiotic and drug metabolism, microbial protection, immunomodulation, preservation of gut barrier integrity, and structure of the GI tract. 55 About 90% of the resident microflora are considered probiotics, while the remaining are commensal and pathogenic microbes. 56
In a healthy gut, different populations of bacteria maintain interspecies communication, limiting potential opportunists and preventing overproliferation and out competition; when these interactions are disrupted, pathogenic species may proliferate leading to various pathological manifestations. Several studies have demonstrated that dysbiosis of the microflora composition is a key component in the pathogenesis of IBD. 57,58 For example, a decrease in Firmicutes (especially Faecalibacterium prausnitzii) with increases in butyrate-producing bacteria has been consistently observed in IBD patients across a number of studies. 59 Butyrate plays an important role in maintenance of gastroinstestinal health, and it has been considered as potentially therapeutic due to its ability to reduce inflammation and enhances epithelial barrier integrity. 60 –63 According to Hamer et al. 2008, 61 human clinical trials have been performed in UC patients to evaluate the therapeutic effect of pure butyrate administration by means of tablets or enemas. However, due to its short and discontinuous exposure in addition to poor patient compliance, these trials were not always successful. Furthermore, the studies also suggested another approach that the direct consumption of butyrate-producing bacteria would be more beneficial and increases the in situ butyrate production, which might lead to gut homeostasis restoration and health improvement in IBD subjects. 64
Studies on the dysbiosis of other enteric microbes such as Enterobacteriaceae, Bacteroides, Bifidobacteria spp., Lactobacillus spp., and Escherichia coli have been ambiguous. 65,66 Several factors, including sample source (stool or biopsy), location of the sample, disease activity (active or latent), diet, age, medication, and methods used for analyzing the microbes may account for these differences. Although dysbiosis has been implicated in GI-related diseases, the mechanism of how it specifically contributes to IBD has not been fully elucidated, but it is well known that therapies, including fecal microbiota transplantation (FMT) and probiotics, correct dysbiosis and significantly improve IBD symptoms. 67 Conflicts exist in using the FMT for IBD treatment. One recent meta analysis revealed that FMT actually worsens IBD. Furthermore, this study also raised the question that it is unknown whether FMT is responsible for the development of other diseases or adverse outcomes. 68 However, in contrast, other recent studies supports the notion that FMT is a promising therapeutic approach, not only for IBD but also for type 2 diabetes and even nonalcoholic steatohepatitis. 69,70 Moreover, to a lesser extent, antibiotic treatment has been shown to be effective in treating IBD, again supporting the importance of gut microbes as a possible pathognomic factor. 71
Although no specific pathogen has yet been clearly identified as a causative agent of IBD, some studies hint toward Mycobacterium avium subspecies paratuberculosis (MAP) as a likely progenitor. 72 Naser et al. 73 demonstrated that MAP was not only present within the inflamed mucosal tissue of CD patients, but that blood levels of culturable MAP were elevated in CD compared to UC. 74 In addition, other recent studies have shown the serum of patients with CD containing significantly higher levels of anti-MAP and antityrosine phosphatase (a component of mycobacterial cell walls) antibodies compared with UC and healthy controls. 75,76 The role of MAP is still controversial, as long-term (2 years) combinational therapy of antibiotics with antituberculosis drugs (clarithromycin, rifabutin, and clofazimine) had little efficacy in CD patients; a recent study recommended this therapy in combination with periodic exposure to radiation. 77,78
In contrast, Fusobacterium varium is present in inflamed mucosal tissue of UC patients, in which combinational therapy (amoxicillin, tetracycline, and metronidazole) showed efficacy in active UC patients when given for 2 weeks. 79,80 Other studies also point to the potential role of fungal microbiota dysbiosis in IBD pathogenesis. 81 For example, Candida albicans was isolated from intestines of CD patients and their healthy relatives. 82 Moreover, several investigations demonstrated a correlation between increased gut E. coli levels and occurrence of CD. 83,84 Specifically, a higher prevalence of adherent-invasive E. coli (AIEC) in ileal lesions was found in CD patients, indicating a potential association with CD. 85 In addition, AIEC proliferation and expression of the outer membrane protein, porin-C, were found to be higher in patients with CD. 86
One longstanding question is whether microbes directly cause IBD or whether IBD increases the risk of gut mucosal infection due to inflammation and structural alterations. Studies have found that the inflamed mucosa is colonized with multiple species of microbes (such as MAP, AIEC, and Clostridium difficile), is involved in dysbiosis, and in disease progression. 87,88 There is no existing evidence that IBD is caused by the imbalance of only one single microbe, but instead is an imbalance of commensal microflora associated with more complex interactions between the host and the entire intestinal microbiota. 89,90 Ultimately, the success of antibiotics in controlling IBD stems from reducing the numbers of potentially pathogenic microbes, although further research is necessary to uncover all potential pathogenic bacterial species that induce or precipitate the occurrence of IBD.
The Three-Prong Interaction in Gut
The three-pronged interaction among probiotics, prebiotics, and the gut is thought to control the activity of native pathogenic microflora represented in Figure 3. Probiotics produce short-chain fatty acids and essential vitamins while enhancing intestinal barrier function via modulating cytoskeletal and tight junction protein phosphorylation. 91 It has been found that different probiotic species have variable impacts on the immune system. 92 The host gut is also supportive to the microbiota by providing nutrition and space to 10–100 trillion bacteria. 93 These probiotic species have been shown to obtain energy by metabolizing dietary fibers (gut enzyme-resistant prebiotics) present in the gut, highlighting this important interaction. 94 Prebiotics (inulin and fructooligosaccharide) nurture a selected group of gut microorganisms, thus selecting for growth of beneficial bacteria. It is reported that prebiotics inhibit certain strains of potentially pathogenic bacteria. 95
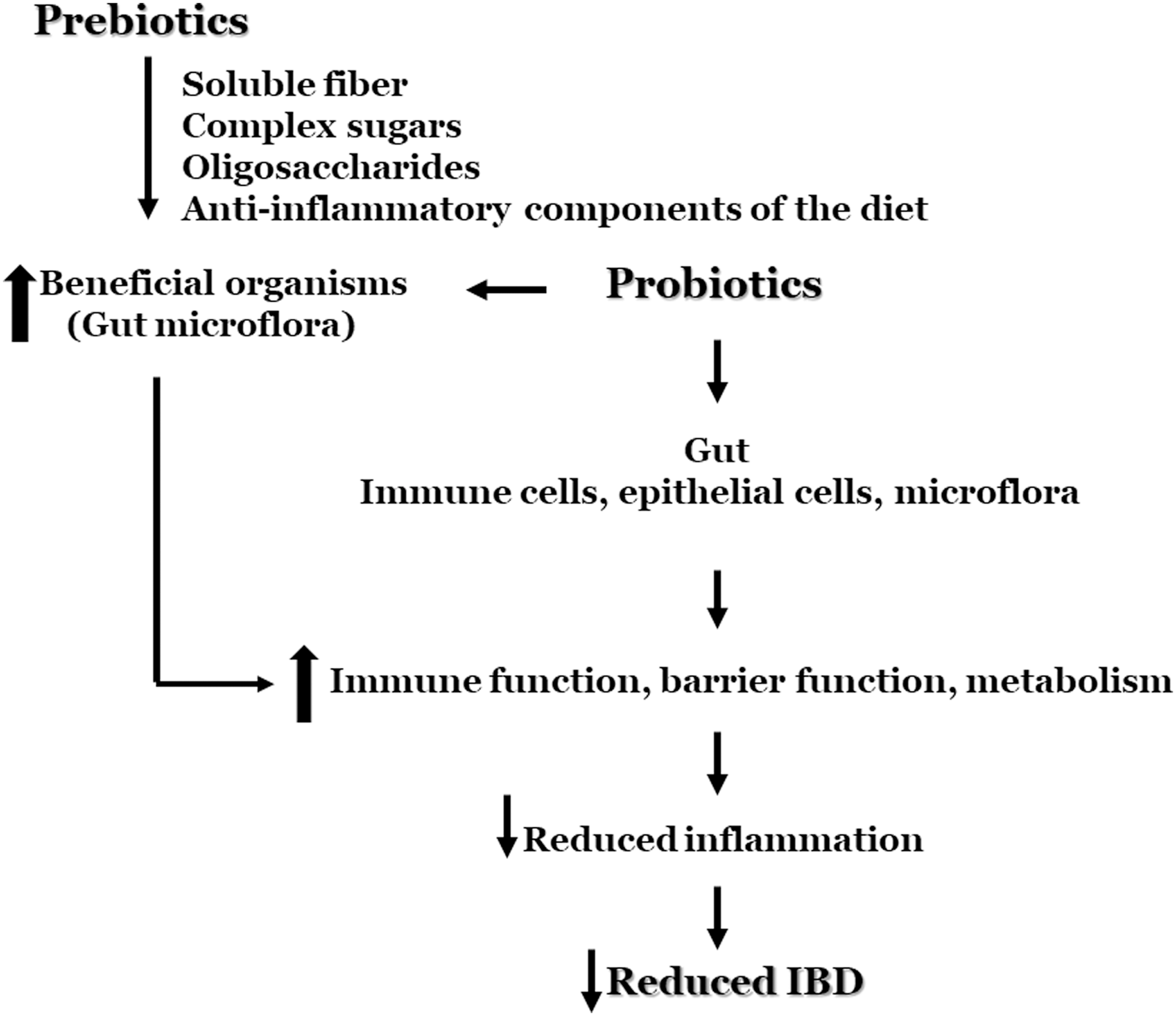
Three-prong interaction among probiotics, prebiotics, and gut tissue.
Food in the etiopathology of IBD
Three main concepts must be considered while studying nutrition and IBD: (1) influence of nutritional components on the etiology, (2) the impact of IBD on nutritional status, and (3) the importance of nutrition as a therapy. 96 Several dietary nutrients have been known to protect intestinal health, while others are known for their detrimental effects on the GI tract by inducing inflammation. 97,98 Composition of various fatty acids, vitamins, minerals, antioxidants, other nutrients, and food's glycemic index might affect its inflammatory potential. Excessive consumption of food and its associated inflammation have been summarized in (Table 4). 99 –102 Evidence revealed that people who consume meat and fats, particularly polyunsaturated fatty acids (PUFAs) and omega-6 (n-6) fatty acids in higher amounts have greater risk of developing IBD than those who consume diets rich in fiber, fruits, and vegetables. 103,104 The European Prospective Investigation into Cancer and Nutrition has shown that excess intake of linoleic acid, an n-6 PUFA, which is present in high concentrations in margarine, cooking oils, and red meat, is greatly associated with the incidence of UC. 105 Fried food containing high levels of peroxidized lipids and their decomposition products commonly consumed in western diet are considered inflammatory. 106 In contrast, a Nurses Health Study found that nurses who consumed higher levels of fiber, particularly fruits, had ∼40% less risk of developing CD; but no relationship was observed for UC. 107
IBD, inflammatory bowel diseases.
In addition to macronutrients, micronutrients such as iron was shown to be positively associated with the development of IBD. Iron is preferentially absorbed in the duodenum and at high enough luminal concentrations causes intestinal inflammation and dysbiosis, induces stress in the endoplasmic reticulum of enetrocytes, and sensitizes the epithelium to cytotoxic T-cell-induced apoptosis. 108 It is known that iron catalyzes the formation of oxygen radicals, thereby instigating cellular injury, increasing intestinal permeability and activation of the transcription factor NF-kB, which induces expression of inflammatory intermediates. 109
Various dietary molecules play an important role in the etiology of IBD, although it has not yet been confirmed that any specific diet is responsible for IBD development. Future research is needed to answer if diet alone is a causative factor for IBD or if there is an interaction between microbes with specific diets which may play a role. Is the occurrence of IBD mainly dependent on genetic components or is it mainly environmental constituents? Specifically, there is high therapeutic potential in developing an evidence-based dietary plan that is effective in controlling IBD symptoms and slow progression.
Diagnosis of Ibd
IBD is diagnosed via a combination of biochemical assays, histological, endoscopic, and radiological investigations. 110 The various biomarkers used for detection of IBD are represented in Figure 4. Biochemical analysis, including complete blood count, liver function test, erythrocyte sedimentation rate, and C-reactive protein, were also performed during early investigations. Blood cytokine levels are also a diagnostic tool. Inflammatory cytokines such as TNF-α, IL-8, IL-4, IL-12, and IL-18 have been found in high concentrations in IBD patients' blood, however, cytokine-based diagnosis is still preliminary. 111 Sigmoidoscopy and colonoscopy allow both the visualization of the macroscopic changes of the gut unique to IBD. 112 For example, CD is characterized by cobblestoning, fissuring, and generalized mucosal erythema whereas UC is characterized by ulceration, bleeding, and luminal dilation. Biopsy of the rectal tissue is performed for histological investigations and can provide information on cellular changes. Radiographic imaging of the GI tract of small bowel postenema is still the tool of choice as it is the least invasive and provides observation of large and small intestine (which is not accessible by scope). 112
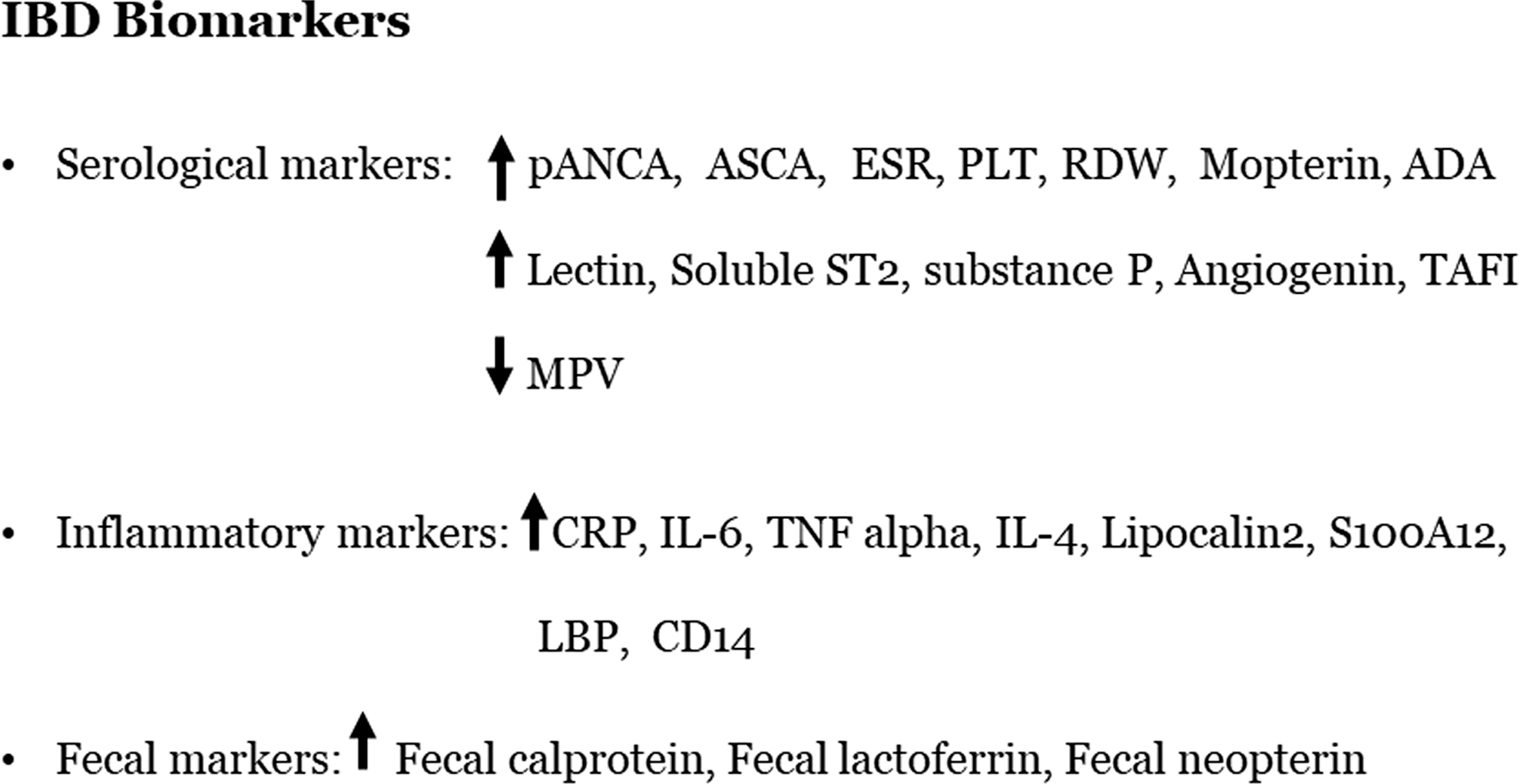
IBD biomarkers. ADA, adenine deaminase; ANCA, anti-neutrophil cytoplasmic antibodies; ASCA, anti-Saccharomyces cerevisiae antibodies; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; LBP, leukocyte binding protein; MPV, mean platelet volume; PLT, platelet count; RDW, red cell distribution; TAFI, thrombin activatable fibrinolysis inhibitor.
Treatment Options for Ibd
Bloody stools, substantial diarrhea, abdominal cramping, abdominal tenderness, and anemia alert patients to seek hospitalization for continuous clinical surveillance. 113 Hemodynamics are monitored carefully and intravenous administration of fluids, nutrients, and corticosteroids is given until the abdominal cramping recedes. 114 Specifically, the patient is restricted from eating spicy, fried, and low-fiber foods to provide relief for the diarrhea and other symptoms. 115,116
For the management of IBD, researchers have focused primarily on nutrition, anti-inflammatory and immunomodulatory agents, and combinatorial approaches. Clinicial treatment follows a “step-up” principle, in which the underlying IBD symptoms are characterized as mild, moderate, and severe, depending on the number of bowel movements per day/severity of symptoms, and treated sequentially. For mild IBD, induction and maintenance are usually achieved with 5-aminosalicylic acid (5-ASA) alone or enterocort. For moderate or refractory mild IBD, immunosuppresants such as corticosteroids, azathioprine, or methotrexate are typically used. Next, for severe or refractory moderate IBD, biologics such as small molecule inhibitors or immunoglobulins, such as anticytokine antibodies, are used. Finally, severe refractory IBD requires surgical resection of the affected bowel. However, with the recent emergence of the dysbiosis concept, new studies have focused on manipulating interactions between beneficial and pathogenic gut microbes as a potential route for IBD management. Different treatment modalities for IBD are summarized in the Table 5. 117 –135 These modalities are a bustling area of research discussed previously within this review. 136
Anti-inflammatory and immunomodulatory drugs
Aminosalicylates are anti-inflammatory compounds containing 5-ASA and have both oral and rectal formulations to treat IBD. 137,138 The first 5-ASA used to treat IBD was sulfasalazine and is still in use, however, about 30% of patients are unable to tolerate it due to side effects. 139 The newer mesalamine preparation, pentasa, has better outcomes in UC and is more tolerable by patients. 140 Like mesalamines, corticosteroids such as prednisolone, methylprednisolone, and budesonide have been found to be effective in both CD and UC, 141 however, concerns for their chronic-use toxicity are long standing, and it has been shown that corticosteroids are major contributors of infections in patients postsurgery due to their immunosuppressive effect. 142 Therefore, toxicity associated with these drugs dramatically limits their long-term use. 143
In contrast to anti-inflammatory drugs, which reduce the inflammatory response, immunosuppressive drugs inhibit proliferation and activation of lymphocytes. 144 Azathioprine, 6-mercaptopurine, methotrexate, cyclosporin, and tacrolimus are the main immunosuppressive drugs that have demonstrated some favorable results in treating IBD. 144 The use of thiopurines was found to augment the efficiency of anti-TNF therapy, however, it is still unclear whether thioprine therapy works independently of TNF-alpha therapy or if they are synergistic. Chaparro et al. 145 showed that 17% of patients discontinued thioprine treatment due to adverse effects. The withdrawal of azathioprine therapy has been proved to have the highest rates for IBD reoccurrence, 146 therefore, the drug is preferably not discontinued if it is well tolerated by patients. Methotrexate treats a wide sprectum of chronic inflammatory diseases, including IBD. It has been found to be effective in inducing remission of 65% of CD patients compared with placebo. 147 Nonetheless, more clinical trials are needed for the use of methotrexate against IBD. 148
Recenty anti-TNF agents, namely infliximab, adalimumab, and golimumab have been used as in the management of CD and UC. 149 Although anti-TNF agents have been found effective and safe, they were not effective in up to one-third of individuals. In addition, these drugs are also very expensive and require injections (which usually reduces patient compliance and thus drug effectiveness). 150
Clinical evidence has shown that enteric microbiota can induce chronic, intestinal inflammation in genetically susceptible hosts. 50 Therefore, therapeutic manipulations of intestinal dysbiosis may be a key beneficial approach and may involve antibiotics, probiotics, prebiotics, or combinations. 151 Antibiotics such as metronidazole, ornidazole, ciprofloxacin, tobramycin, clarithromycin, cotrimoxazole, and antituberculosis treatments have been found to be useful in the treatment of IBD. 152 In addition, it has been claimed that deficiencies in the mucosal peptide (defensins) may be involved in the pathogenesis of IBD. Conversely, other reports suggest that defensin deficiency might be a consequence of destruction in the mucosal surface due to inflammation, which indicates that reduced defensin expression is a result of the disease progression and not vice versa. 153 More research is required to understand this concept.
Probiotics have been recommended as preventive as well as therapeutic measures for IBD and for establishment of a healthy composition and function of the gut microbiome. 154 It has been identified that in IBD subjects, probiotic Lactobacillus strains increase the integrity of the intestinal barrier, induce immune tolerance, hinder pathogenic bacterial translocation, and reduce GI infections. 155 Probiotics also have the ability to modulate the intestinal immunity and regulate the intestinal cell responses. 156 A recent study demonstrated symptomatic relief in IBD subjects treated with a probiotic mixture of Lactobacillus acidophilus, Lactobacillus plantarum, Lactobacillus rhamnosus, Bifidobacterium breve, Bifidobacterium lactis, Bifidobacterium longum, and Streptococcus thermophiles. 157 Moreover, S. boulardii has been found to improve the intestinal permeability in CD patients. 158
Intestinal microbes also play a role in the development of neurological disorders, 159 which has been demonstrated in animal studies. 160 In those cases, probiotics 161 alleviated the clinical symptoms and reduced inflammation by suppression of IL-17 production and induction of regulatory T cell accumulation in secondary lymphoid organs. These studies suggest that probiotics could result in changes of the intestinal microbiome composition, which might be beneficial in subjects suffering from autoimmune diseases. 161 Overall, probiotics help to restore the healthy composition of the gut microbiome and present beneficial functions to gut microbial communities, resulting in prevention and reduction of gut inflammation. Studies show that specific probiotic species or strains demonstrate specific clinical effects. This has been considered as an effective and safe modality in achieving clinical remissions in patients with mild-to-moderate UC. 162 To date, few trials have been performed to study the effect of probiotics on IBD patients, and thus no clear definitive relationship has yet been established. Although the aforementioned evidence supports probiotics as a promising therapeutic agent, it has still not been acknowledged by the FDA as an approved therapy for treatment or prevention of diseases. At this point, we can consider probiotics as dietary supplements only.
Prebiotics, which is the method of altering diet to facilitate beneficial microbes and suppress pathogenic ones may represent a novel therapeutic option for IBD, especially when combined with probiotics (symbiotics). Although there is no evidence to support prebiotic monotherapy showing efficacy in treating IBD, a combinatorial approach in addition to more research is required to validate this.
Role of Nutrition in Ibd
Enteral nutrition therapy with elemental, semielemental, and defined formula has been studied for the clinical management of IBD, 163 however, the mechanism by which nutrition reduces disease activity, and its symptoms remain uncertain. It has been speculated that nutritional deficiencies in IBD patients may be corrected by some formulated diet. 164 The impact of diet on gut microbiome, epithelial function, and immune system might have importance in nutritional therapy of IBD. 165 Existing evidence suggests that dietary alterations may affect gut microbiome, 166 and because certain microbe species may be responsible in the pathogenesis of IBD, dietary manipulation of the gut microflora may prove an efficacious IBD treatment modality. To date, very few evidence exists for the benefits of any particular diet. Specialized dietary formulations have been studied in the treatment of IBD and shown to be effective in pediatric CD patients, but not in adults, which need to be further investigated. 166
Role of Genetics On Ibd
Genetics has been at the forefront in explaining part of the IBD pathogenesis, while aiding clinicians in judging lifetime risk of developing the disease. The idea of a genetic basis of IBD susceptibility was initially confirmed by monozygotic and dizygotic twin studies, which showed a concordance of 37% and 4% for CD; 10% and 3%, respectively, for UC. 167 In addition, studies reveal that 12% of all IBD patients have a positive family history, and susceptibility is directly dependent on degree of relative (CD RR 1st: 7.7, 2nd: 2.44, 3rd: 1.88; UC RR 1st: 4.08, 2nd: 1.85, 3rd: 1.51). 168 –170 Furthermore, Barrett et al. calculated that genetics contribute ∼20% to CD susceptibility. 171 As noted before, the pathogenesis of IBD is very complex, owing, in part, to the complex host-environment-genetics interplay, and with the advent of Genome Wide Association Studies (GWAS), this complexity has been slowly decoded and has directly resulted in the identification of more than 50 IBD-susceptibility genes, a number which is rapidly growing annually.
As mentioned previously, the intestines maintain an anti-inflammatory state via several mechanisms and genetic mutations in proteins that govern these functions render the intestines susceptible to uncontrollable inflammation. The first groundbreaking study to demonstrate a specific IBD-susceptibility locus was done by Hugot et al. who showed that an insertion mutation at position 3020 of the NOD2 gene was associated with increased susceptibility to developing CD. 172 Other inflammatory genes were then subsequently screened with GWAS for similar associations, which resulted in the identification of mutations involving IL23R, 173 its signaling mediators; JAK, 174 STAT, 175 and IL12B, 176 and resultant cytokines TNF-α 177 as IBD susceptibility genes. Other inflammatory mediator deficiencies were later linked with IBD, such as IL-10, 178 NLRP3, 179 and CCR6. 174 Moreover, genes associated with intestinal autophagy, including IRGM and ATG16L1, 180 and gut embryogenesis such as NKX2.3 180 and GLI1 181 were linked to heightened IBD developmental risk later in life. Interestingly, multiple GWAS analyses of various ethnic backgrounds revealed that there are staunch differences in hereditary susceptibility loci between ethnic groups, suggesting a more complex gene–environment interaction than once believed. 182,183
Conclusion
IBD, including both CD and UC, is a chronic, relapsing inflammatory disorder prominent in the United States and Europe. Recently, strides have been made to elucidate it's etiology. It is anticipated that understanding of the etiopathogenesis of IBD will lead to more efficient therapeutic approaches. The major goal is to elucidate the involvement of all factors; environmental, genetic, bacterial, nutritional, and immunological in the initiation and progression of this disease to uncover the most comprehensive treatment.
Take-Home Message
• Many factors, including diet, environment, genetics, and gut microbiome play a role in the etiopathogenesis of IBD. The complex interplay between these aspects makes delineating a universal cure very difficult.
• IBD consists of separate, yet, similar diseases, UC and CD. Both are associated with similar symptoms, but are differentiated by location of inflammation (CD: small and large bowel, UC: large bowel only) and bleeding (UC).
• The IR of IBD is correlated with the industrialization of countries where more industrialization is correlated with higher IR. This might be due to changes in diet associated with higher average incomes of families or other environmental factors.
• Diets associated with high quantities of PUFAs are at greater risk of developing IBD. This could be why increased industrialization equals higher IR. This also highlights the importance of an anti-inflammatory-component-rich diet, such as sesame oil use, as a nonpharmacological therapeutic agent to cure/prevent.
• The gut microbiota plays a greater role in the progression/prevention of gut-associated diseases, including IBD. A three-pronged interaction among probiotics, prebiotics, and the gut seems to verify their significance in the pathogenesis/prevention of IBD.
Footnotes
Acknowledgment
This work was supported by the State of Florida Legislative Crohn's grant program to UCF College of Medicine.
Author Disclosure Statement
No competing financial interests exist.