
Abstract
The efficacy and safety of Tremella fuciformis (TF) as a nutritional supplement were assessed in individuals with subjective cognitive impairment (SCI). Seventy-five individuals with SCI were enrolled in an 8-week, randomized, double-blind, placebo-controlled trial of TF (600 mg/day, n = 30 or 1200 mg/day, n = 30) or placebo (n = 15). The primary outcome measure was changes in total scores of the subjective memory complaint questionnaire. The secondary outcome measures were changes in performance on short-term memory and executive functions, which were assessed using standardized cognitive tests. In addition, voxel-based morphometry was performed to examine the effects of TF on changes in gray matter volume. The individuals in the TF group showed greater improvements in the total scores on the subjective memory complaint questionnaire compared with those in the placebo group. There were also significantly greater improvements in short-term memory and executive functions in the TF group relative to the placebo group. Exploratory analysis demonstrated that there were significant group-by-visit interactions on the left precuneus, right supramarginal gyrus, right middle frontal gyrus, and right postcentral gyrus at corrected P < .05. Overall frequency of adverse events did not differ among high-dose TF (40.4%), low-dose TF (35.1%), and placebo groups (41.4%). The current findings suggest that TF could be safely administered to relieve subjective memory complaints and enhance cognition in individuals with SCI.
Introduction
T
Recently, there has been increasing evidence that polysaccharides derived from medicinal mushrooms have neuroplastic effects. 1,2,9 TF significantly enhances neurite outgrowth, which was induced by nerve growth factor, and reduced the neurotoxic effect of β-amyloid peptide in PC12h cells. 3 TF also promoted peripheral nerve regeneration by increasing neurotrophic gene expression in the animal nerve injury model. 9
Although the evidence of neuroprotective and neurotrophic effects of TF is accumulating, the efficacy and safety of TF, as a nutritional supplement for cognitive improvement, have not yet been studied.
Self-reported memory complaints are common problems, which negatively impact the quality of life 10 in middle-aged and elderly persons. 11 Subjective cognitive impairment (SCI) could be defined when an individual has a self-perceived cognitive problem without any diagnosable cause. 12 Although the scores of cognitive tests are within a normal range, the presence of subjective cognitive complaints is acknowledged as an at-risk target population for early intervention to prevent future development of neurodegenerative disorders, including Alzheimer's dementia. 13 Nutraceutical approaches, administration of functional foods that exhibit neuroprotective effects, are increasingly studied to find an effective and safe intervention in the individuals with SCI. 14,15
Although the relationship between SCI and objective cognitive performance is inconsistently reported in the previous studies, 16 impaired short-term memory and executive functions are suggested to be critical to daily life and may be related to SCI. In addition, these cognitive domains may decline as aging progresses and be affected earlier during the neurodegenerative changes. 17
In this study, we conducted an 8-week, double-blind, randomized, placebo-controlled trial to examine the efficacy and safety of oral administration of TF in individuals with SCI. The primary outcome measure was change in the degree of subjective memory complaint. Changes in short-term memory and executive performance were measured as the secondary outcomes. The effects of TF administration on structural brain changes were also assessed using voxel-based morphometry to characterize the brain mechanisms underlying its therapeutic actions. We hypothesized that oral supplementation of TF would reduce memory complaints and enhance cognitive performance accompanied by regional gray matter volume alteration.
Materials and Methods
Participants
The community-dwelling subjects, aged from 40 to 65 years, were recruited through local advertisements. The inclusion criteria were as follows: 12 years or more of education and subjective cognitive complaints with no clinical impairments, which were obtained by medical history taking and evaluated by physical and neurological examinations, including laboratory blood tests.
The exclusion criteria were as follows: suspected or diagnosed as mild cognitive impairment (MCI) of Alzheimer's dementia (Mini-Mental Status Examination score ≤24 or Clinical Dementia Rating Scale ≥0.5); present axis I mental disorders; lifetime substance use disorders; severe major illness that requires proper treatment; history of loss of consciousness or seizure caused by head trauma; use of central nervous system medications within the last 3 months; intelligence quotient below or same as 80; or contraindications to magnetic resonance imaging.
Before any study procedure was conducted, written informed consent was obtained from the study participants. The study protocol and consent forms were approved by the Bioethics Committee of Ewha Womans University.
Study design and interventions
Seventy-five participants were enrolled in the 8-week double-blind, placebo-controlled trial (clinicaltrials.gov identifier: NCT002377024). Participants were randomly assigned to low-dose TF (600 mg/day, n = 30), high-dose TF (1200 mg/day, n = 30), or placebo (n = 15) groups in a 2:2:1 ratio. Each group received a total six capsules per day and ingested two capsules at three difference times. The appearance of each capsule did not differ, and placebo capsules were indistinguishable from TF capsules. After the baseline visit, participants visited at 4 and 8 weeks. The detailed preparation method of TF supplementation is described elsewhere. 2
The study participants were advised to discontinue any nutritional supplements. When the participants needed to be newly treated during the study period with the medication potentially affecting the central nervous system, their participation in this study was discontinued.
At each visit, the remaining capsules and diaries were returned. Compliance was monitored by the returned capsule counts, and the times of missed administration of the capsules were recorded.
Outcome measures
Assessments of the primary and secondary outcome measures were performed at baseline and 8 weeks after baseline.
Primary outcome measure
The primary outcome variable was changes in the Subjective Memory Complaints Questionnaire (SMCQ) scores that assess self-reported cognitive impairment and were validated questionnaires for SCI. 10,18 SMCQ contains 14 items and consists of two domains: global memory function and everyday memory function. Global memory function is assessed by asking the self-judgment of the subjects' memory: whether they have memory problems or recognize the cognitive decline. 10 Everyday memory function is assessed by asking common situations of memory difficulty such as remembering shopping items, recent events, and the location of objects. 10 The response is yes (1 point) or no (0 point) and the score ranges from 0 to 14 points. The optimal cutoff score suggested for screening dementia is 5 or 6 points. 10 The changes in the SMCQ scores have been used as outcome variables in the previous study of SCI. 18
Secondary outcome measures
The secondary outcome measures were changes in performance on short-term memory and executive functions as well as changes in gray matter volumes.
Short-term memory performance was evaluated at baseline and 8 weeks using the immediate recall domain from the pattern recognition memory task and the spatial span task, both of which are taken from the Cambridge Neuropsychological Test Automated Battery (CANTAB). 19 Executive function was assessed using the Wisconsin Card Sorting Test (WCST). 20 Each test score was standardized to Z scores, using the group means and standard deviation (SD) of the placebo group after adjusting for age, sex, intelligent quotient, and baseline performance. Total errors of the spatial span and preservative errors of the WCST were reversed to indicate that positive Z score means better performance. The composite score for each cognitive domain (short-term memory and executive functions) was calculated by averaging the standardized Z score of each test.
Using voxel-based morphometry of high-resolution three-dimensional T1-weighted magnetic resonance (MR) images, changes in gray matter volumes were assessed as the secondary outcome measure. Detailed information on image data acquisition and image data processing are described in the sections of Image data acquisition and Voxel-based morphometry analysis.
Safety measures
The Udvalg for Kliniske Undersogelser (UKU) Side Effect Rating Scale 21 was used to assess safety and tolerability of study medications, and spontaneous, self-reported, adverse events were also recorded. Vital signs, height, and weight were measured, and physical and neurological examinations were performed at each visit. Routine laboratory examinations, including the complete blood cell count, blood chemistry, differential white cell count, urine analysis, and urine pregnancy test were performed at baseline, 4 weeks, and 8 weeks (Green Cross Laboratories, Yongin, South Korea). Electrocardiograms were obtained at baseline and 8 weeks after baseline.
Image data acquisition
A 3.0 Tesla Philips Achieva MR scanner (Philips Medical System, Netherlands) equipped with a 32-channel head coil was used for acquisition of high-resolution multimodal neuroimaging data, including T1-weighted and resting-state functional images. Structural images were acquired using a three-dimensional T1-weighted magnetization-prepared rapid gradient echo imaging sequence with the following acquisition parameters: repetition time = 7.4 ms, echo time = 3.4 ms, flip angle = 8°, field of view = 220 × 220 mm2, slice thickness = 1 mm, number of excitation = 1, and 180 contiguous sagittal slices.
Voxel-based morphometry analysis
Optimized voxel-based morphometry was performed using the software of FMRIB's Software Library. 22 After performing skull stripping to remove nonbrain tissues on T1-weighted images, tissue-type segmentation was carried out using FMRIB's Automated Segmentation Tool. Gray matter partial volume images were aligned to the Montreal Neurological Institute standard space using FMRIB's Linear Image Registration Tool and averaged to create an initial template. The final study-specific gray matter template was created by averaging gray matter images, which were normalized to an initial template using FMRIB's Non-Linear Image Registration Tool (FNIRT). Individual gray matter images in the native space were nonlinearly registered to the study-specific template using FNIRT. The registered images were modulated by multiplying them with the determinant of the Jacobian of the warp field to estimate gray matter volume at each voxel 22 and were then smoothed with an isotropic Gaussian Kernel with a sigma of 3 mm.
Statistical analyses
Demographic and clinical characteristics were compared between the treatment groups by an analysis of variance (ANOVA) for continuous variables and a chi-square test for categorical variables. The intent-to-treatment population was used in the analysis.
The mixed-effects model for repeated measures data was performed for analyzing the primary outcome measure. SMCQ scores were adjusted for age, sex, intelligent quotient, and baseline value, and these adjusted SMCQ scores were used as the dependent variables. The secondary outcome measures for changes in short-term memory and executive functions were also analyzed using the mixed-effects model for repeated measures data. Treatment groups (high-dose TF vs. low-dose TF vs. placebo), visits, and treatment group-by-visit interaction were included as fixed effects. The within-subject factor was considered as a random effect.
Cook's distance, which is often used to assess the influence of individual observations on the regression analysis and identify statistical outliers, was estimated in each observation. 23 Four, three, and four observations with Cook's distance >0.058, were finally removed from the analysis of changes in SMCQ, short-term memory, and executive functions, respectively.
The secondary outcome measure for changes in gray matter volumes was assessed using voxel-based morphometry. Treatment group-by-time interaction on gray matter volumes was also analyzed on a voxel-by-voxel basis. The results were corrected for multiple comparisons using Monte Carlo simulation with 10,000 iterations implemented in the ClusterSim utility (
Proportional differences in all adverse events were assessed between the TF and placebo groups using a chi-square test. We further explored potential differences in the frequency of adverse events between the low and high dose within the TF group.
An α-level of 0.05 (two-tailed) was considered significant for all analyses. Data were analyzed using Stata v13.1 (StataCorp., College Station, TX, USA).
Results
Participant characteristics
Among the 88 subjects who were assessed for the study eligibility, 75 were randomly allocated to receive supplementation, and 69 completed the study (Fig. 1). The completion rates did not differ among the high-dose TF, low-dose TF, and placebo groups (93.3% vs. 90.0% vs. 93.3%, respectively). The demographic and baseline assessments were similar among the three groups (Table 1).
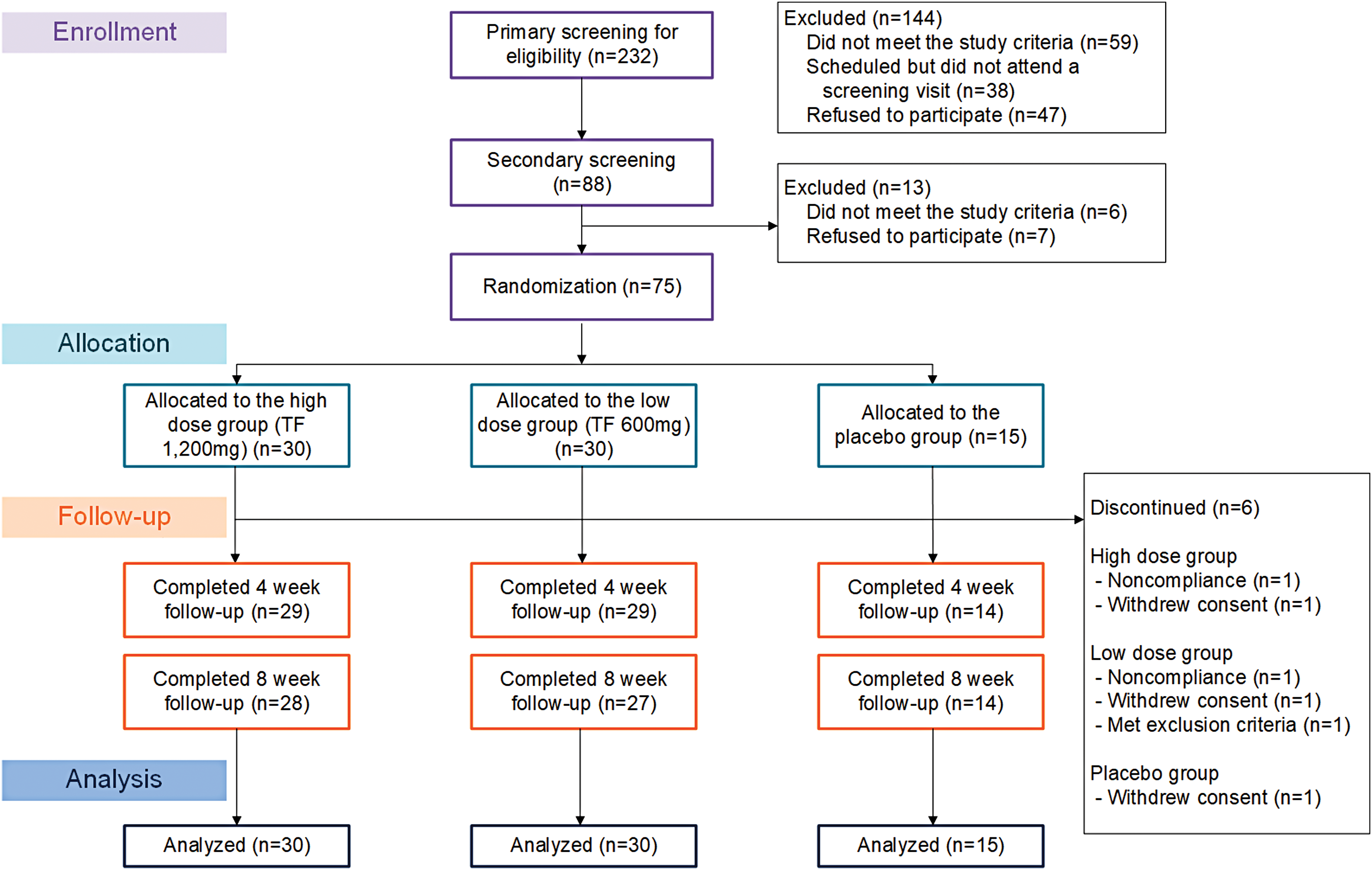
Screening, randomization, and disposition of participants with SCI randomly assigned to the high-dose TF (1200 mg daily), low-dose TF (600 mg daily), or placebo groups. SCI, subjective cognitive impairment; TF, Tremella fuciformis. Color images available online at
TF was administered in two different dosing schedules; a low-dose schedule with 600 mg and a high-dose schedule with 1200 mg of TF.
IQ, Intelligence Quotient; MMSE, Mini-Mental Status Examination; SD, standard deviation; SMCQ, subjective memory complaints questionnaire; TF, Tremella fuciformis.
Adherence to treatment
Study compliance was >90% in all three groups. The mean percentages of returned pill counts were similar among the three groups (one-way ANOVA, P = .79): high-dose TF group 8.0% (SD 6.5%), low-dose TF group 9.2% (SD 7.6%), and placebo group 8.1% (SD 6.6%). Adherence rate assessed by the intake diary also showed no significant differences among the groups (one-way ANOVA, P = .09): high-dose TF group 93.8 (SD 4.5%), low-dose TF group 91.9% (SD 6.5%), and placebo group 95.6% (SD 2.7%).
Primary outcome measure
The primary outcome of interest was the rate of improvement in subjective complaints of cognitive impairment. The rate of improvement in SMCQ scores was greater in individuals with the both high-dose (z = −3.16, P = .002) and low-dose (z = −2.68, P = .007) TF groups compared with those of the placebo group (Fig. 2). These results remained unchanged when Hamilton Depression Rating Scale (HDRS) scores were included as an additional covariate (high-dose group, z = −3.25, P = .001; low-dose group, z = −2.70, P = .007). There was no difference in changes of SMCQ sores between the high-dose and lose-dose TF groups (z = −0.61, P = .54).
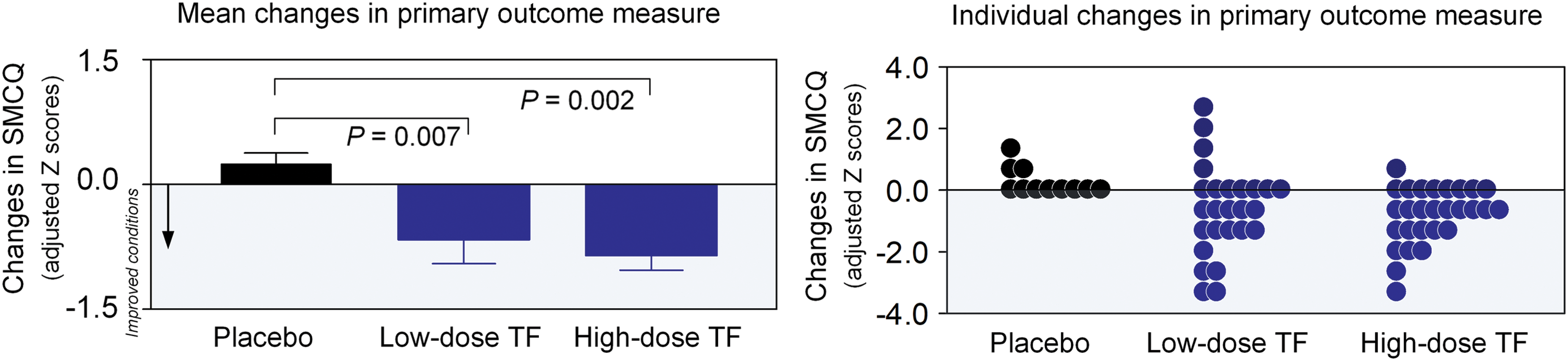
Changes in SMCQ scores in individuals with SCI randomly assigned to high-dose TF, low-dose TF, and placebo administration. Changes in SMCQ scores were analyzed using the mixed-effects model for repeated measures data. Main effects for treatment groups (high-dose TF vs. low-dose TF vs. placebo) and visits as well as their interaction terms were included into the model. P values for the treatment group-by-visit interaction on SMCQ scores were calculated. Absolute scores at baseline and at endpoint are presented in Supplementary Table 4. Error bars represent standard errors of the mean. SMCQ, subjective memory complaints questionnaire. Color images available online at
Over the treatment period, individuals of the high- and low-dose TF groups showed 9.18% and 3.97% decrease in SMCQ scores, while changes in SMCQ scores were minimal (1.02% increase) in those of the placebo group.
Secondary outcome measures: short-term memory and executive functions
Secondary outcome measures were changes in performance on short-term memory and executive functions over an 8-week period. We found significant treatment group-by-visit interactions on both short-term memory and executive functions. Improvement in short-term memory performance was greater in the high-dose (z = 3.35, P = .001) and low-dose (z = 3.31, P = .001) TF groups than in the placebo group (Fig. 3A). Significant improvement with high-dose TF (z = 2.33, P = .02), but not with low-dose TF (z = 1.75, P = .08), relative to placebo administration was also observed in executive function performance (Fig. 3A).
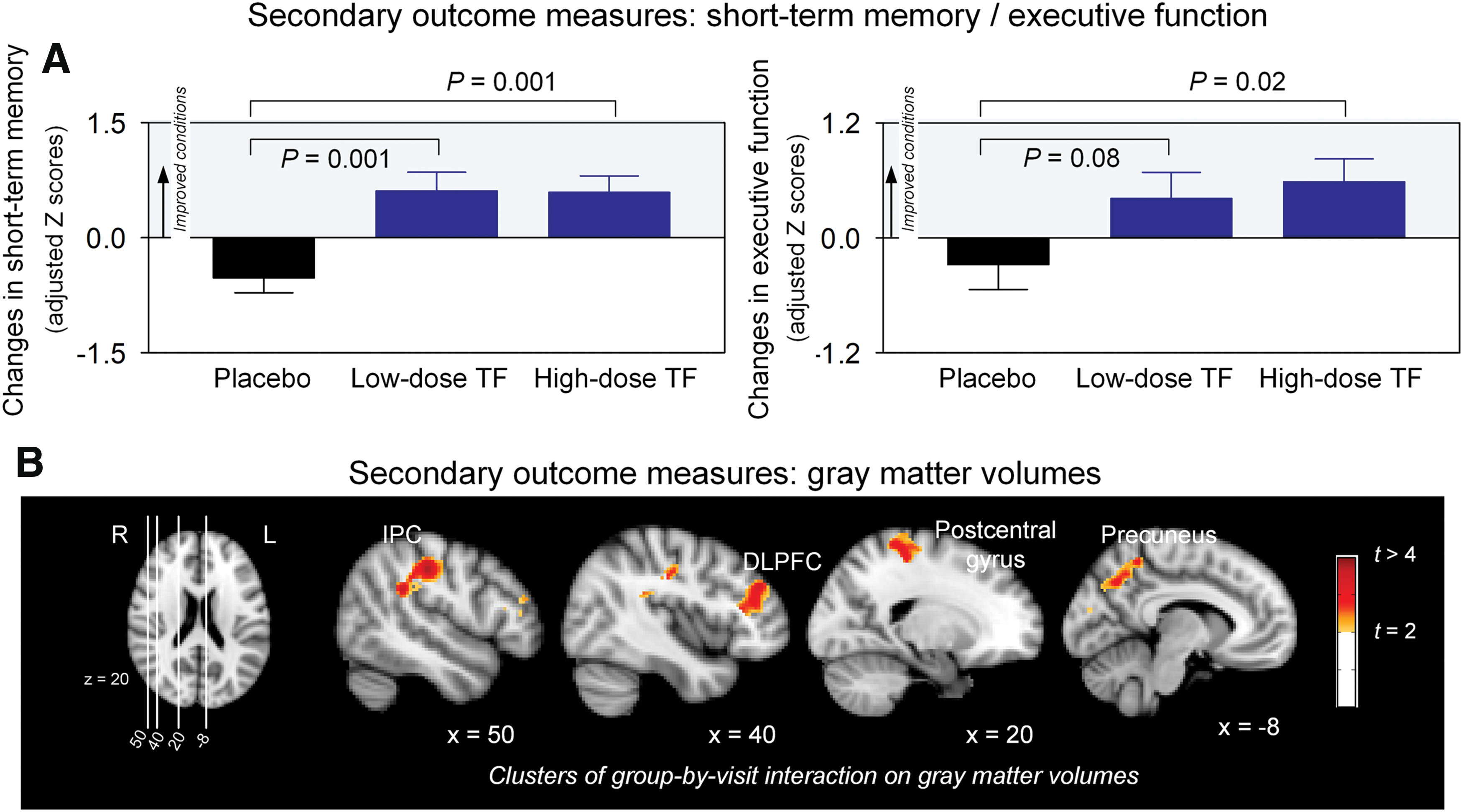
Changes in adjusted Z scores of short-term memory and executive functions in individuals with SCI randomly assigned to high-dose TF, low-dose TF, and placebo administration
However, there was no differences in the rate of cognitive improvement between the high-dose and low-dose TF groups (short-term memory function, z = 0.07, P = .94; executive function, z = 0.77, P = .44).
Secondary outcome measures: gray matter volumes
Changes in gray matter volumes were also examined using voxel-based morphometry as the secondary outcome measure. Significant treatment group-by-visit interactions were found in the left precuneus, right supramarginal gyrus, right middle frontal gyrus, and right postcentral gyrus (P < .05, with correction for multiple comparisons, Fig. 3B; Supplementary Table S1; Supplementary Data are available online at
We explored the relationships between changes in gray matter volumes and changes in cognitive performance in individuals treated with TF. Gray matter volume increases in the dorsolateral prefrontal cluster were correlated with improvement in executive performance in the TF group (r = 0.33, P = .02).
Safety and tolerability
No serious adverse events were reported. All reported adverse events are listed in Supplementary Table S2. There were no differences in the overall frequency of adverse events among the high-dose TF (n = 23, 40.4%), low-dose TF (n = 20, 35.1%), and placebo groups (n = 12, 41.4%) (χ 2 = 0.46, P = .793). The most common adverse event reported in the TF group was weight gain. However, there was no difference in changes of body mass index between groups (z = −0.64, P = .523). There were no participants who discontinued the trial because of adverse events in either treatment group. There were no differences in laboratory findings between the treatment groups (Supplementary Table S3).
Discussion
This randomized clinical trial demonstrated that oral administration of TF improved subjective memory complaints and cognitive performance in individuals with SCI. Specifically, subjects in the groups with TF oral supplementation showed greater improvement in short-term memory and executive performance than those in the placebo group. Along with these findings, TF supplementation was associated with increases in gray matter volumes of several brain regions, including the dorsolateral prefrontal cortex. The changes in the SMCQ scores have been used as outcome variables in a previous study of the SCI. 18 The results of the study extends the previously reported preclinical evidence of TF as a potential nootropics in middle-aged individuals with SCI. TF oral administration may be a safe prevention strategy for individuals with SCI.
TF extract is rich in polysaccharides, which consist of D-mannan backbone with various side chains, including glucuronic acid, xylose, and fucose. 4,24 The improvement in subjective memory complaints is consistent with a previous study, which reported that dietary saccharide intake is associated with greater ratings of self-reported everyday memory in middle-aged adults. 25 These results remained significant after adjusting for the effects of smoking, drinking, and exercise status. 25 The daily amount of polysaccharide intake could be inadequate if an individual consumes a minimal amount of fruit and vegetable, which are rich in saccharides. 26
Although there is little evidence about the effect of TF extract on cognition in humans, one randomized clinical trial has examined the effects of 12-week saccharide supplementation and reported benefits on short-term memory and well-being. 25 Another clinical trial explored the acute effect of nonstarch polysaccharide and reported higher levels of performance in short-term memory and executive performance. 27 Supplementing polysaccharide extracted from TF could be a safe and efficient approach to ensure sufficient uptake of saccharides and promote memory. 26
While the exact mechanism of subjective and objective cognition improvement is not clear, preclinical studies suggest that F extract scavenges reactive oxygen species, 28 modulates the immune system, 29 and reverses risk factors of metabolic syndrome. 5,7 Along with these indirect effects, TF extract also has direct neurological effects, including stimulation of neurite outgrowth, 3 promotion of hippocampal long-term potentiation, 30 increased acetylcholine release and choline acetyltransferase activity, and reduced scopolamine-induced impairment of learning and memory in rats. 1
This study is the first to use structural neuroimaging measures to investigate the efficacy of TF supplementation. There was only one experimental study that utilized functional brain measures with cognitive tests. 31 Acute changes in electroencephalography were found after administering a mixed carbohydrate formula, 31 but it is hard to determine the underlying brain changes related to cognitive improvement. In this study, several brain regions showed gray matter volume increase after TF administration, and it is worthwhile to note that the extent of gray matter change in the dorsolateral prefrontal cortex was associated with improvement in executive function. These findings may support the in vivo evidence of neurotrophic effect of TF. For instance, TF may increase the gray matter volume due to neurite outgrowth or synaptic plasticity, which was repeatedly reported in preclinical studies. 3,30
Individuals with SCI may suffer from subtle declines in short-term memory and executive functions in daily life, even though standardized neuropsychological tests fail to detect changes in cognitive performance. 10,17 Middle-aged adults who do not show a clear cognitive decline, but have early signs of brain aging, are an important target population that may benefit from nutritional interventions. 32 Short-term memory and executive functions are closely related to handling information needed in everyday activities. Thus, TF-induced improvement may promote better quality of life and the self-perception of memory in middle-aged adults with SCI.
High- and low-dose TF were well tolerated with similar overall rates of adverse events. There was no difference in laboratory findings and body mass index among the groups. In East Asia, Tremella is a common food widely used. To the best of our knowledge, there are no reports of major health risks associated with Tremella. One thousand two hundred milligrams per day of TF administration would be a safe and easily accessible intervention for individuals with SCI.
In this study, we did not find a dose-dependent response. Although executive performance was significantly improved only in the high-dose TF group, the dose group-by-time interaction effect was not significant. The negative findings could be interpreted as a ceiling effect or inadequate sample size to detect differences between the two different doses. The optimal dosage of TF should be studied in further large-scale studies.
Medicinal mushrooms are a good source of bioactive polysaccharides, which are increasingly receiving attention for various biological effects. The supplementation could exhibit different effects on cognition according to the types, preparation method, and the main source of polysaccharides. Further studies are needed to replicate our findings in a larger population and examine the effects in other cognitive domains and neuroimaging measures.
In conclusion, the results of this study demonstrate that oral administration of TF as a potential method to reduce subjective memory complaints in individuals with SCI is effective for improving short-term memory and executive performance. The safety and tolerability profile are favorable. Thus, we could consider TF as a promising option that could be used to prevent further cognitive decline in adults with subjective cognitive complaints.
Footnotes
Acknowledgments
Fire Fighting Safety and 119 Rescue Technology Research and Development Program funded by the Ministry of Public Safety and Security (MPSS-Fire Fighting Safety-2016-86), and the Brain Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (2015M3C7A1028376), grant from Pulmuone holdings.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.