
Abstract
Ingestion of bioactive compounds, such as hesperidin and naringin, found in citrus fruits and orange juice, can improve the homeostasis of gut microbiota. A controlled clinical study with temporal series intergroup design with 10 apparently healthy women (28.5 ± 8.4 years, 24.1 ± 3.3 kg/m2) were evaluated after continuous consumption of commercial pasteurized orange juice for 2 months. Samples of blood serum and stool were collected at basal time and periodically during the experiment for biochemical and microbiology assays. Intestinal microbiota was evaluated for total anaerobic bacteria, Lactobacillus spp., Bifidobacterium spp., and Clostridium spp. An independent culture evaluation was performed using Denaturing Gradient Gel Electrophoresis (DGGE). The pH, ammonium (NH4 +), and short-chain fatty acids (SCFAs) were evaluated for microbial metabolism. The results showed that daily intake of orange juice did not change women's body composition, but improved blood biochemical parameters, such as low-density lipoprotein-cholesterol, glucose, and insulin sensitivity. Orange juice positively modulated the composition and metabolic activity of microbiota, increasing the population of fecal Bifidobacterium spp. and lactobacillus spp. Polymerase chain reaction–DGGE of microbiota showed similar composition of total bacteria, and microbial metabolism showed a reduction of ammonia and an increase of the production of SCFAs. These results suggested that a daily consumption of orange had a positive effect on the intestinal microbiota and metabolic biomarkers of young women, which may be an effective alternative for a healthy drink.
Introduction
It is estimated that the gastrointestinal tract is inhabited by 10 11 cells per milliliter of luminal contents, comprising of 400 to 500 bacterial species. 1 The gut microbiota is composed primarily of strict anaerobic bacteria, which outweigh the facultative anaerobic and aerobic bacteria. 2 The main microbiota phyla are Bacteroidetes, Firmicutes, Proteobacteria, and Actinobacteria. The most common genera found are the Bifidobacterium spp., Clostridium spp., Eubacterium spp., and Ruminococcus spp. 3 The composition of the intestinal microbiota is influenced by immunological and dietetic factors. 2 The diet has an influence on the environment of the intestine, including pH, intestinal transit, and changes in intestinal microbiota. 1 The microbiota exerts the functions of degradation of nondigestible dietary components, such as fiber, modulation of the immune system, synthesis of vitamins K and B12, and production of short-chain fatty acids (SCFAs). 4
The host's health can be benefited on the balance between commensal and pathogenic bacteria in the gut. 5 According to Eckburg et al., 6 the intestinal microbiota is steady and balanced, or in homeostasis, during adulthood, but can destabilize through stress, chemotherapy treatments, remedies, and diets. However, the balance of microbiota can be achieved through the ingestion of probiotic foods, prebiotic ingredients, and bioactive compounds, such as phenolic compounds. 1 The phenolic compounds are transformed by the intestinal microbiota in bioactive metabolites, which may promote the maintenance of intestinal homeostasis and stimulate the growth of beneficial bacteria (Lactobacillus spp. and Bifidobacterium spp.) and inhibit pathogenic bacteria (Clostridium spp.). 7
The phenolic compounds are characterized by the presence of one or more aromatic rings linked to at least one hydroxyl radical. The main groups of polyphenols are flavonoids, phenolic alcohols, stilbenes, and lignans. 8 The main sources of flavonoids include fruits (grapes, cherries, apples, citrus fruits, among others) and vegetables (pepper, tomato, spinach, onion, and broccoli). 9 In vitro studies have shown that citrus flavonoids, hesperidin and naringin, from orange juice show a variety of biological activities, as antioxidants, anti-inflammatory, antitumor, reduction of high cholesterol, and increased insulin sensitivity. 10 Orange juice along with citrus fruits have been highly valued as an essential part of a tasty and nutritious diet. The flavors provided by orange juice and citrus fruits are among the most popular in the world. In addition, the orange juice and citrus fruits are rich sources of vitamins, minerals, and dietary fiber that are essential for the growth and development of global nutrition. 11,12
The daily consumption of orange juice has been associated with a reduction in the onset of chronic diseases, improved lipid profiles, and decrease of the total cholesterol and inflammatory markers. These effects are due to the presence of bioactive compounds, such as ascorbic acid, carotenoids, and flavonoids (hesperidin and naringin). 13,14 This is the first clinical trial reported on the intake of orange juice and its effect on the gut microbiota, microbial metabolism, and bowel function. Using a clinical trial, we evaluated the effect of chronic intake of pasteurized orange juice (POJ) on the microbiota composition and metabolism of healthy individuals.
Materials and Methods
Individuals
Ten healthy female volunteers were selected among students of the Pharmacy School, UNESP, in Araraquara, Brazil. The women's baseline characteristics were 28.5 ± 8.4 years, weight 63.4 ± 9.6 kg, and body mass index (BMI) 24.1 ± 3.3 kg/m 2 . The subjects were nonsmokers and not vegetarians, and they were not taking hormones, dietary supplements, and medication for any gastrointestinal or metabolic disease, no probiotics or prebiotics in the last 3 months, and no antibiotics in the last 6 months. They did not regularly drink alcohol or perform intensive physical exercise. The study was approved by the Ethics Board of the Pharmacy School, UNESP (protocol #1,644,906), and enrolled in the Clinical Trial Protocol Registration and Results System (ID: NCT03032861).
Orange juice
Commercial pasteurized 100% orange juice was provided by Citrosuco (Matão, Brazil). The juice stored at −20°C was distributed weekly to volunteers, in 2-L PET bottles, without label identification, and thawed before consuming 300 mL daily.
Experimental protocol
A controlled nonrandomized clinical study with temporal series intergroup design, which includes: (1) 30-day Basal period, which included similar food pattern for all participants, without restriction of energy, avoiding rich sources of flavonoids, probiotics and prebiotics, and alcoholic beverages, followed by (2) Experimental Period of 60 days consuming 300 mL/day of orange juice, and (3) Washout of 30 days, without orange juice, totaling a 120-day trial period (Fig. 1). All participants did not consume fruit or citrus juices or alcohol for 3 days before the start of treatment with the orange juice (Experimental Period). Sampling of blood serum and feces was made on the first day of Pretrial, on the 30th, 60th, and 90th day of the experimental schedule.
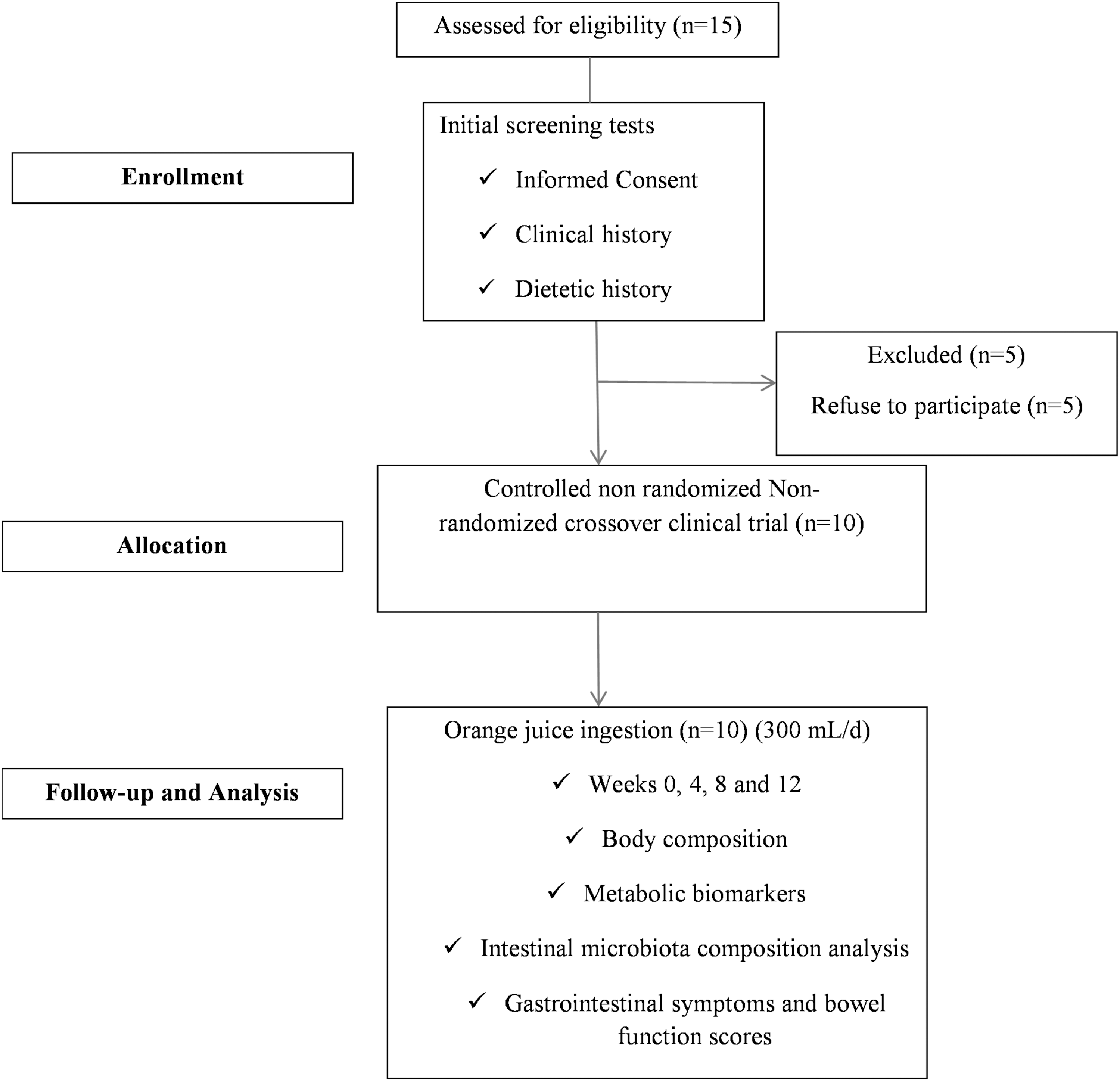
Controlled nonrandomized crossover clinical trial design.
Body composition
Body weight (kg), height (m), muscle mass (kg), fat mass (kg), and body fat percentage (%) were measured with bioimpedance (Inbody 720®) during the experimental protocol. The BMI was interpreted according to the World Health Organization (2000). 15
Blood collection and biochemical parameters evaluation
Fasting blood samples of the volunteers were drawn 30 days before the Basal period; after 30 and 60 days of consumption of orange juice (300 mL/day) (Trial period); and after 30 days without orange juice (Washout). All samples were collected at a local clinical laboratory and analyzed for total cholesterol, high-density lipoprotein-cholesterol, low-density lipoprotein-cholesterol (LDL-C), triglycerides, glucose, and insulin. Glycemic and insulin curves were performed after glucose load at 0, 30, 60, 90, and 180-min time schedule twice: at the Basal and after Trial period. Insulin resistance was estimated by homeostatic model assessment insulin resistance (HOMA-IR) equation, as following:
Stool collection
Total 24 h feces were collected on the eve of the beginning of the experiment (Basal period) and subsequently every 30 days until the end of the experiment (Trial Period and Washout). The feces were homogenized, and a sample was stored in a sterile plastic tube (10 mL) and kept at −80°C in ultrafreezer (Haier Biomedical, Qingdao, China) until analysis.
Microbiological analysis
The intestinal microbiota composition analysis was based on the presumptive enumeration of Lactobacillus spp., Bifidobacterium spp., total anaerobes, and Clostridium spp. Serial dilutions in sterile peptone water were prepared and the inoculation held in selective growth media. Total anaerobic bacteria were determined by Standard Methods Agar (Himedia, Brazil) and incubation at 37°C/48 h for anaerobic form, and respectively, MRS Agar (Himedia) with incubation at 37°C/48 h, anaerobically, was used to determine the number of Lactobacillus spp., agar BIM-25 16 with an incubation at 37°C/72 h, anaerobically, was used to determine the number of Bifidobacterium spp., and the Reinforced Clostridial Agar (Himedia) 37°C/48 h for anaerobic form was used to determine the number of Clostridium spp.
Molecular methods (polymerase chain reaction (PCR)–Denaturing Gradient Gel Electrophoresis [DGGE]) were used to analyze the effects of the orange juice ingestion on the community of total bacteria. The DNA of the samples used was extracted through the Fast QIAamp DNA Stool Mini Kit (Qiagen, Hilden, Germany). The initiators used to replicate the DNA were 968FGC (5′-CCG GCC GCC GCC GGG CGC GGC GCA GCG GGG GGG GGG CGG CGC GAA GAA GAA CCT TAC-3′) and 1401R (5′-CGG TGT GTA CAA GAC CC-3′). 17 For the polymerization of DNA GoTaq® Green Master Mix (Promega) was used, the samples were then amplified in a thermal cycler (Applied Biosystems) using the following conditions: initial denaturation at 95°C for 7 min; 35 cycles of denaturation at 94°C for 45 sec, annealing at 56°C for 45 sec, extension to 72°C for 1 min, and final extension 72°C for 10 min, followed by cooling to 4°C. For electrophoresis, an 8% polyacrylamide gel with a denaturing gradient of 45–65% was used during 16 h at 75 V in a buffer ATE 1 × at constant temperature of 60°C, as described by Dos Reis et al. 18 The gels were stained with ethidium bromide 19 and scanned (400 dpi) and analyzed using the BioNumerics software, version 6.0 (Applied Maths, Belgium). Distance matrices for each DGGE were based on the similarity coefficient of Pearson. These matrices were used for cluster analysis. The analysis was performed using the BioNumerics software, version 6.0.
Determination of ammonium (NH4 +), pH, and SCFAs in fecal samples
NH4 + was determined by ion-selective meter (model 710A; Orion) coupled to the ion-selective electrode of ammonium chloride (model 95–12; Orion). The samples were added to a 0.5 mL solution with pH and ionic strength adjustment (Ammonia pH Adjusting Ionic Strength Adjuster Orion) and had the content of NH4 + measured three times. 20 Concentrations of SCFAs were determined in a 1:19 dilution of 100 μL supernatant. The analysis of pH was made from 1 g (the same used to make ammonium chloride), in which the same was diluted in 9 mL of distilled water, measured by a pH electrode.
The SCFAs were analyzed using a gas 2010 Chromatograph Model (Shimadzu, Japan) equipped with a split/splitless injector, a flame ionization detector, and an automatic sampler CombiPAL for head space analysis. The SCFAs were separated using a HPINNOWAX column (30 m × 0.25 mm × 0.25 μm) (Agilent Technologies). The carrier gas was hydrogen and the flow rate was 1.45 mL/min. The temperature of the injector and detector was 240°C. 21
Gastrointestinal symptoms and bowel function scores
Weekly diary was applied to record the individual gastrointestinal symptoms (diarrhea, abdominal pain, bloating, nausea, vomiting, flatulence, and blood in stool). During the entire study period, the participants were required to record the bowel function (consistency of stool, frequency of bowel movements, effort to evacuate, and painful bowel movements). The consistency of the stool was classified by the Bristol stool form modified, 0 (watery); 1 (smooth); 2 (segmented); and 3 (dry). The average frequency of evacuations was calculated by the number of stools per week, 1 (daily); 2 (every other day); and 3 (less than three times a week). The effort to evacuate was classified as 1 (very easy); 2 (easy); 3 (hard); or 4 (very hard). Painful evacuations were classified as 2 (rarely); 3 (a few times); and 4 (always).
Statistical analysis
The results are presented as average and standard deviation for Pretrial, Basal, Trial period (intervention with orange juice), and Washout (30 days). Data were analyzed by repeated analysis of variance measures and Tukey post-test, with significance level of p < 0.05, using Sigma Stat 5.0 software.
Results
Evaluation of body composition and biochemical parameters
No change was observed in the body composition before (Basal), during the Experimental Period with orange juice, or after Washout (Table 1). All individuals showed biochemical variables within the reference values for all periods of the experiment, which were compatible with apparent health. After 30 days of consumption of orange juice, there was a slight reduction of glucose, insulin, HOMA-IR index, triglycerides, total cholesterol, and LDL-C (Table 1). At the end of the intervention period (60 days of orange juice consumption), there was a significant reduction in blood glucose by 6.3%, insulin by 33%, HOMA-IR by 44%, triglycerides by 30%, total cholesterol by 14%, and LDL-C by 16%, in comparison to the Basal values (Table 1). A significant increase by 6.5% was verified for glycemia, 40% for insulin, 47% for HOMA-IR, 21% for triglycerides, 12% for total cholesterol, and 5.2% for LDL-C (Table 1). The area under the curve (AUC) and maximum concentration (Cmax) of glycemic and insulin curves are shown in Figure 2. Glycemia AUC was reduced by 5.2% (p < 0.05), and both insulin AUC and Cmax were lowered by 16% (p < 0.001) (Fig. 2).
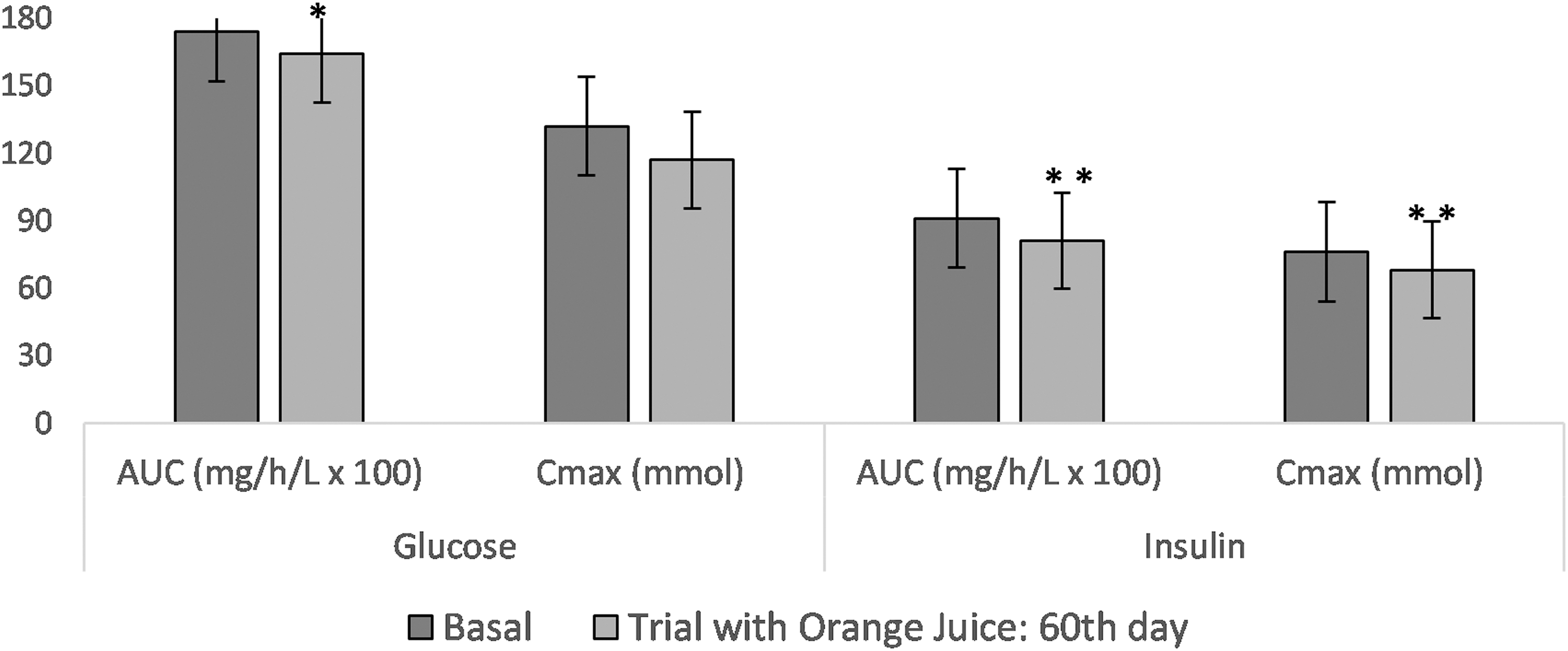
AUC and Cmax of the glycemic and insulin curves at basal and after 60 days of consumption of 100% orange juice (300 mL/day). *p ≤ 0.05, **p ≤ 0.01 (Basal period × Trial with Orange Juice: 60th). AUC, area under the curve; Cmax, maximum concentration.
Anthropometric, Blood Serum Biochemical, and Intestinal Health Features of Ten Female Volunteers Assessed for 120 Days of Orange Juice Clinical Trial
Different letters represent significant difference (p < 0.05) between periods (n = 10).
Consistency of stool: 0 (watery); 1 (smooth); 2 (segmented); and 3 (dry).
Frequency of bowel evacuations was calculated by the number of stools per week: 1 (daily); 2 (every other day); and 3 (less than 3 times a week).
Effort to evacuate was: 1 (very easy); 2 (easy); 3 (hard); or 4 (very hard). 4 Painful evacuations were: 2 (rarely); 3 (a few times); and 4 (always).
BMI, body mass index; HDL-C, high-density lipoprotein-cholesterol; HOMA-IR, homeostatic model assessment insulin resistance; LDL-C, low-density lipoprotein-cholesterol.
Effect of orange juice on the growth of intestinal bacteria
Populations of Lactobacillus spp., Bifidobacterium spp., total anaerobic, and Clostridium spp. in fecal samples of eutrophic individuals are presented in Figure 3. A significant increase from 5.89 ± 0.90 to 7.12 ± 0.50 log10 cfu.g−1 of Lactobacillus spp. population was observed during the intervention with orange juice. There was an increase of 6.12 ± 0.84 to 6.87 ± 0.36 of log10 cfu.g−1 for Bifidobacterium spp. Total anaerobic bacteria population increased from 6.18 ± 0.71 to 7.12 ± 0.50 log10 cfu.g−1 ; but after washout, there was a nonsignificant reduction for 6.94 ± 0.48 log10 cfu.g−1 . Growth of Clostridium spp. was not significantly increased from 6.19 ± 1.04 to 6.91 ± 0.59 log10 cfu.g−1 throughout the experimental period. In summary, these results suggest that the commercial pasteurized 100% orange juice may stimulate the growth of Lactobacillus spp., Bifidobacterium spp., and total anaerobic bacteria in the intestinal microbiota of healthy women.
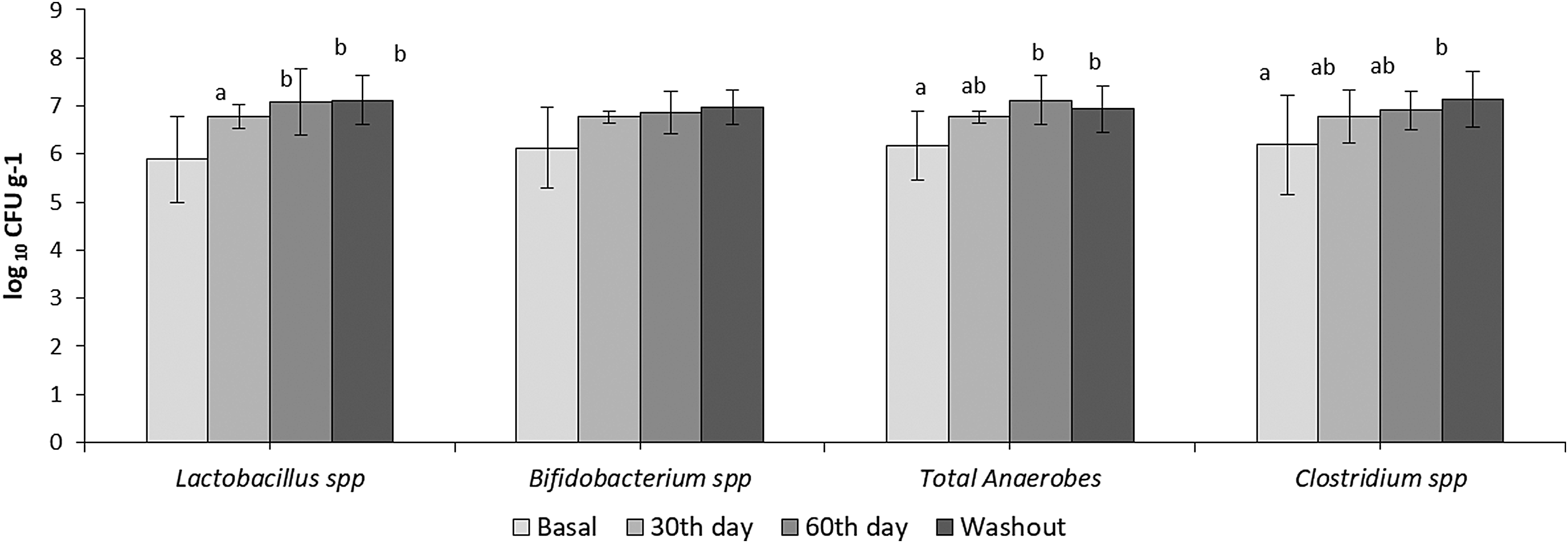
Growing of four bacterial groups (log10 cfu.g−1 ) from 24-h feces of female volunteers (n = 10). Samplings were from Basal period, Trial with Orange Juice: 30th day, 60th day, and Washout. Different letters mean significant differences between periods for the same microorganisms (p < 0.05).
Qualitative monitoring changes assessed by DGGE analysis showed changes in the composition and structure of total bacteria in the feces of four individuals during the whole experimental protocol. A cluster analysis of the DGGE profiles showed great similarity among these four individuals (73 at 93%) independent of the experimental period (Fig. 4).
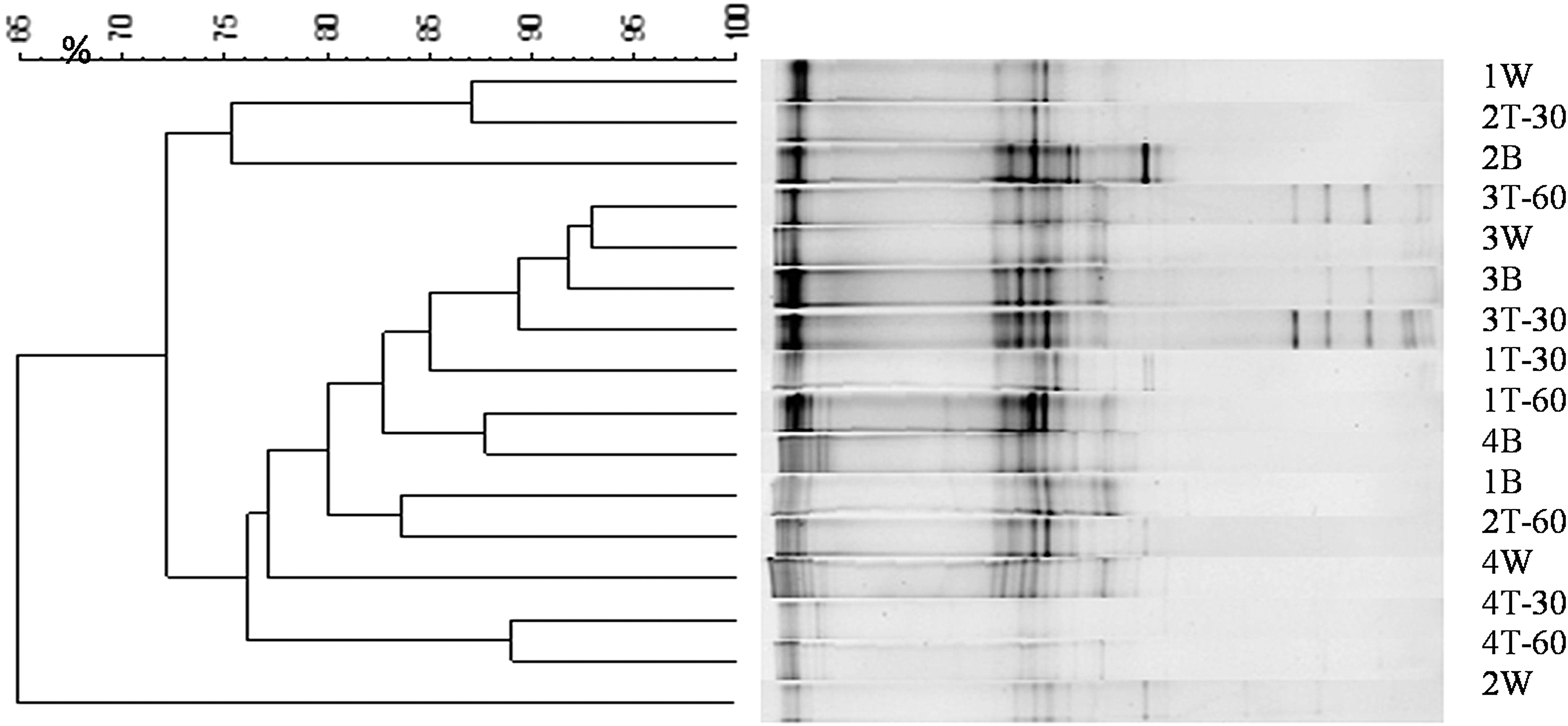
DGGE of total bacteria showing four subjects (1, 2, 3, and 4) at Basal (B), 30th day trial (T-30), 60th day trial (T-60), and Washout. DGGE, Denaturing Gradient Gel Electrophoresis.
Effect of orange juice on the intestinal bacteria metabolism
After 60 days of the orange juice intervention, there was a significant reduction of NH4 + metabolites from intestinal bacteria, but after washout it went back to the initial values. pH values showed no significant variation during the experimental period (Table 1). Production of SCFAs were significantly increased throughout the experimental period for acetic acid, but decreased for propionic acid after 60 days of orange juice consumption and after washout decrease for propionic acid (Fig. 5).
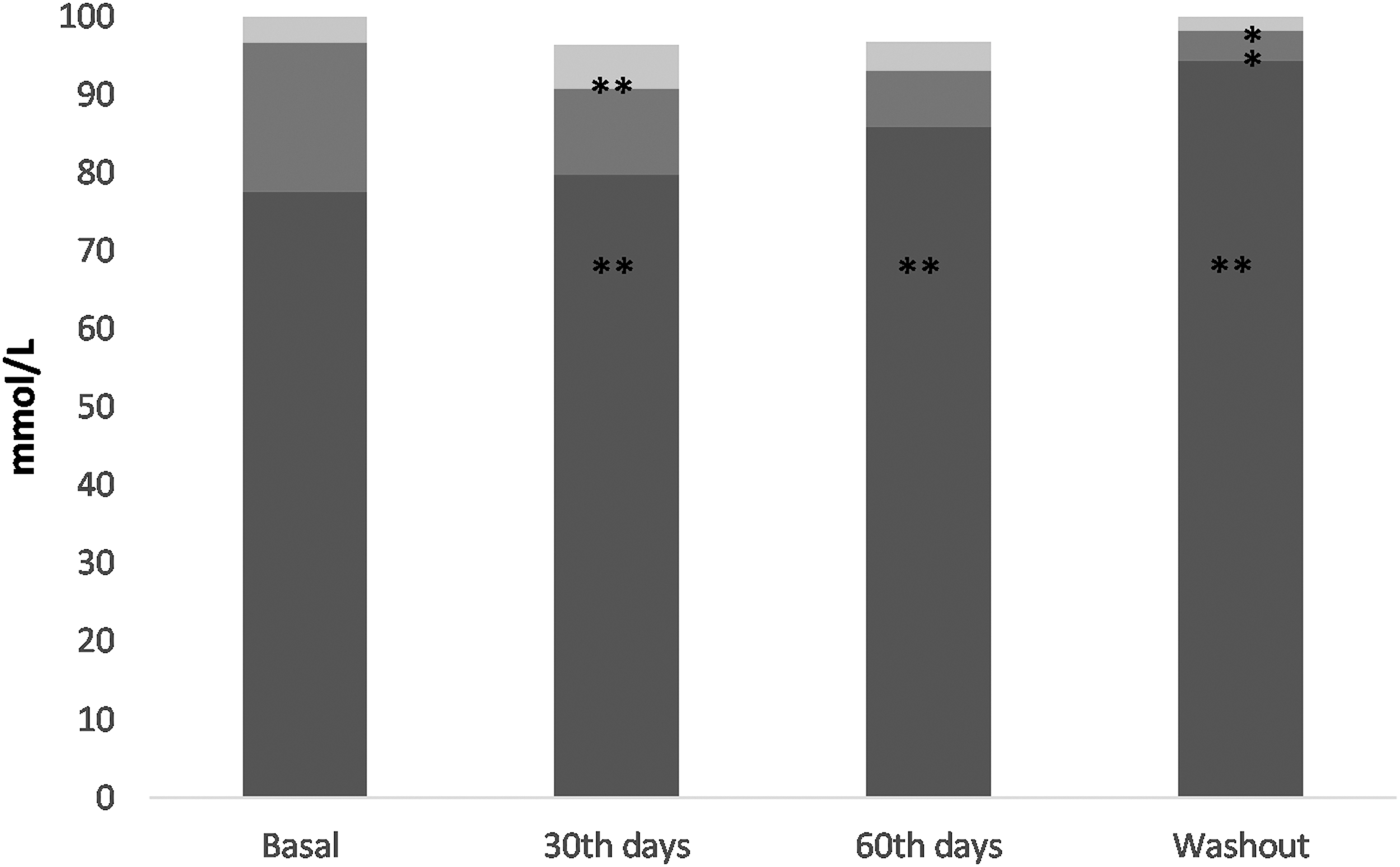
SCFA ratio upon feces. Relative SCFA levels are indicated in each bar (%). Samplings were from Basal period; Trial with Orange Juice: 30th day, 60th day; and Washout. Black, acetic acid; gray, propionic acid; light gray, butyric acid. Significant increases are indicated by **, whereas significant decreases are indicated by **(p ≤ 0.05) (n = 10). SCFA, short-chain fatty acids.
Effects of orange juice on intestinal function of individuals
The effect of orange juice on intestinal function of volunteers is shown in Table 1. Stool consistency levels, frequency of bowel movements, effort to evacuate, and painful evacuations did not present significant differences during the periods examined. It is observed that after the intervention of orange juice for 60 days, there was an improvement in the consistency of the stool from 0.94 ± 1.0 to 1.2 ± 0.63, but average frequency of evacuations remained in 1.4 ± 0.69, moreover, orange juice helped to lower the effort to evacuate from 2.4 ± 0.69 to 2.2 ± 0.4, and in decreased painful bowel movements from 3.5 ± 0.52 to 2.4 ± 0.51.
Discussion
There is growing scientific interest in the pharmacological effects of nutraceuticals and functional foods on human health, and more recently on the gut microbiota. In this sense, orange juice contains a set of powerful bioactive molecules, including flavonoids, carotenoids, vitamin C, folate, and other phytochemical compounds that may affect systemic and intestinal metabolism. 22 Clinical studies currently show that daily consumption of orange juice is associated with the reduction of chronic diseases, improvement of lipid profile, decrease of total cholesterol, and arterial blood pressure. 12,14 In addition, studies using a colonic model have shown that orange juice has a positive effect on the intestinal microbiota, such as increased bacterial population of Lactobacillus spp., Bifidobacterium spp., and reduction of Enterobacteria. In vitro studies also showed that orange juice increased the production of SCFAs and decreased the content of NH4 +. 23,24
This study provided insights about regular orange juice intake and blood glucose, lipids, and gut microbiota metabolites of healthy women. First, we evaluated the effect of orange juice on body weight and BMI of eutrophic women, based on the assumption that the regular consumption of orange juice does not affect body composition over time, according to our previous findings. 25 These results agree with other clinical studies that showed the daily intake of orange juice did not affect body weight, BMI, or abdominal fat in obese subjects. 26,27
We also observed a significant reduction in blood serum of glucose, insulin, triglycerides, total cholesterol and LDL-C, and HOMA-IR index after 60 days, but intermediate lower values are observed at the 30th day for all variables, except LDL-C that dropped significantly by the 30th day. Clinical studies have also reported that hesperidin, a citrus flavonoid from orange juice, has the ability to reduce hepatic enzymes responsible for synthetizing cholesterol and transferring triglycerides and assembling VLDL and, consequently, lower LDL-C in the bloodstream. These changes increase hepatic receptors that speed the clearance of circulating LDL-C particles. 28 In addition, studies have shown that hesperidin indirectly affects insulin resistance status. One of the suggested routes shows that POJ can stimulate the growth of intestinal microorganisms, which increases the production of SCFAs that modulate adipose tissue, skeletal muscle, and liver tissue function, improving glucose homeostasis and insulin sensitivity. 29
Interestingly, in this study we observed a significant growth of presumptive Lactobacillus spp., Bifidobacterium spp., and total anaerobic bacteria in fecal samples after 60 days of orange juice intake. These positive changes in the prebiotic functionality are maintained through the washout period. Similar results were observed by Duque et al., 24 assessing the influence of fresh and POJ on the intestinal microbiota using colonic model (SHIME®). Studies involving the effect of orange juice on the microbiota are still rare. Some authors suggest a relationship between diets rich in polyphenols and the increase of Lactobacillus spp., and Bifidobacterium spp. 14,30,31
Previous conventional quantitative microbiological analysis showed that less than one-half of the gut microbes is cultivable with the standard laboratory protocols. 7,32,33 Therefore, a qualitative analysis of total bacteria was performed using the cultivation-independent PCR-DGGE method. PCR-DGGE analysis can be used to monitor the profile and changes of the microbial community under different treatments. 34 In this study, PCR-DGGE analysis showed high similarity of total bacteria among the subjects, independent of the experimental protocol period. These results indicated that the regular intake of 100% orange juice helps to maintain the total bacteria community. However, the similarity of the microorganisms found in the participants' microbiota may have been affected by standardization of their diet during the study.
Another way to evaluate the dietary influence on microbiota are the release of metabolites, which are intermediates, or end products of food components by commensal metabolism can exert necessary actions on immunity of the host. In our study, a significant reduction of NH4 + after 2 months of orange juice consumption was obtained. The concentration of NH4 + in the intestine results mainly from amino acid deamination and hydrolysis of urea by intestinal bacteria. 35 On the contrary, elevated NH4 + concentration may have a detrimental effect on intestinal health and affect energy metabolism of colon epithelial cells, inhibiting the oxidation of SCFAs and suppressing cell proliferation. 35,36 Previously others have shown that the regular intake of probiotics and prebiotics was effective in reducing NH4 + concentration. 20,37
Some of anaerobic gut microbes have the potential of converting dietary carbohydrates into organic acids, including lactate, and SCFAs, the latter principally referring to acetate, propionate, and butyrate. 35,38 SFCAs are recognized as essential for gut physiology because they function as a primary source of energy to the enterocytes, stimulate epithelial cell proliferation, improve blood flow, increase the absorption of sodium and water that can stop diarrhea, decrease the intraluminal pH and, finally, decrease the absorption of ammonia. 39 In fact, after 30 days of orange juice, the female volunteers showed a significant increase of butyric acid and acetic acid. Similar results were observed in similar studies that evaluated the influence of orange juice on the intestinal microbiota using a colonic model. 24,40 The increase of acetic acid can be attributed to citrus flavonoids. Orange juice flavanones are poorly bioavailable, and approximately 70% of them pass intact through the small intestine to the colon, where they are hydrolyzed by the microbiota to flavanone glycosides. 41 A previous in vitro colonic study showed that naringenin, after suffering ring fission, yields 3-(4-hydroxyphenyl) propionic acid, and thereafter by gut microbiota-mediated dehydroxylation produces sizable quantities of 3-(phenyl) propionic acid, and smaller amounts of 4-hydroxyphenylacetic acid as result of a shortening of the side chain. In addition, other recent studies have shown that the intestinal microbiota is capable of transforming phenolic compounds into SCFA, which can help to achieve better intestinal health. 7,42,43 The increase of SFCA can also be attributed to the carbon sources present in the orange juice, since carbon serves as substrate in the fermentation of intestinal bacteria and effectively participates in the production of SFCA in the colon. 34 The carbon used by Bifidobacterium spp. and Lactobacillus spp. is responsible for producing large quantities of SFCA. 44
The increase in acetic acid production is beneficial because it may downregulate the cholesterol synthesis after absorption 45 and promotes calcium absorption in the colon. 46 The increases of butyric acid is beneficial, since it is the main energy source of the colonocytes and has anti-inflammatory and anticarcinogenic properties and propionic acid is widely absorbed by the liver. 47
There is a potential role of SCFA as signaling molecules regulating hepatic glucose homeostasis, but has not been fully elucidated in humans. Interestingly, we observed after 60 days of orange juice consumption, a significant reduction in blood serum of glucose, insulin, triglycerides, total cholesterol and LDL-C, and HOMA-IR index. In fact, acetate, propionate, and butyrate can regulate hepatic lipid and glucose homeostasis in an adenosine monophosphate-activated protein kinase-dependent manner involving peroxisome proliferator-activated receptor-γ-regulated effects on gluconeogenesis and lipogenesis. 48
On the other hand, the measurement of stool pH showed that the intake of orange juice did not change the chemical acidity of the gut environment during the experimental period as shown previously in humans consuming orange juice containing microencapsulated probiotic. 41 Finally, the bowel habits of all participants in our study were evaluated based on the stool consistency, frequency of bowel movements, effort to evacuate, and painful bowel movements. The results showed a small improvement in the stool consistency and frequency of bowel movements, which can prevent constipation, abdominal pain, headaches, dizziness, and lack of appetite. 49
Our study provided significant insights about the influence of regular intake of 100% orange juice on the intestinal microbiota, and an improvement of blood serum biomarkers, which probably was influenced by SCFA production by the microbiota. These results suggested a prebiotic effect of orange juice as an alternative healthy drink, with the positive effect on the intestinal microbiota and metabolic biomarkers of young women.
Footnotes
Acknowledgment
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
Author Disclosure Statement
No competing financial interests exist.